The Many Faces of Adrenal Insufficiency
40.33k views4026 WordsCopy TextShare

Southern Medical Association
Educational video made available by the Southern Medical Association.
Please support our mission to ...
Video Transcript:
[Music] why the heck adrenal insufficiency well the endocrine Society says that adrenal insufficiency is not managed well in the United States so they got this committee together and they fed them and you know probably high fat food and they said make up some new guidelines about adrenal insufficiency and they did so we're gonna whiz through these don't worry you'll get to the beach we're going to take a look at the evaluation and management of adrenal insufficiency and they said you know virtually everybody who treats patients and anybody who treats them with steroids needs to know how to manage adrenal insufficiency so how many of you use steroids in your practice how many treat Mary Jo is Stewart oh you're good guys most of you we we like you because endocrinologist look at folks who use steroids and like rheumatologists and say oh those people just create problems alright so here's a lady she's 32 years old she had hypothyroidism she had that already and she comes to my office once a year to say hi and get her prescription renewed and see if she has any problems so she said you know my skin is getting darker particularly my gums and lately I've been feeling dizzy I stand up and I haven't done my strength training exercises and I'm feeling kind of dizzy so she brings a picture from a year ago last week she brings her two pictures on her phone isn't that great you know you're pitting your patients my patients send me stuff saying I got this rash do you think it's from my medicine and and it's attached to the epic on this little you know phone picture it's just amazing so anyway her blood pressure I took her blood pressure in my offices 102 over 70 sitting at 80 over 60 standing oh that doesn't sound good her lab had a potassium of 5. 5 which is a little above our upper limit of normal sodium 132 a little bit low and a little bit acidotic here oh so she has hyperkalemia and she has hyponatremia she's a little acidotic she has or the static - tension nausea dizziness uh-huh and here's her picture so here's her picture last year and here's her picture this year she's right she's turning brown what the heck could that be and here these aren't her gums she obviously didn't have a mustache but yeah this is characteristic of Bob oh gosh we're talking about adrenal insufficiency right so primary or secondary what does she have she have a problem with her pituitary or her a dream okay well let's keep going she had remembered that the laboratory evaluation of this requires a CBC sometimes they have anemia they have relative lymphocytosis they can it is an affiliate chemistry you want to know about the glucose ii of hypoglycemia with adrenal insufficiency hyponatremia metabolic acidosis rarely hypercalcemia hyperkalemia is seen primarily in adrenal insufficiency primary adrenal insufficiency so in our patients case somebody got an ACTH which was 5,000 normal was up to 150 her random cortisol was 4. 5 and normal 7 to 20 so she has an elevated ACTH and a slightly low cortisol so where is the problem you think it's how many people think the problems in pituitary you people have to start this conference from the beginning and sit through the whole thing again how many people think it's in the adrenal yes you people can go home after this lecture okay so you've made the diagnosis she has a high ACTH and a low cortisol and when you see someone in your office and you think oh gosh they may have primary adrenal insufficiency don't just get a random cortisol like everybody does get an ACTH and a random cortisol ACTH is high cortisol is low you've made the diagnosis you don't need any test only works in primary adrenal insufficiency only works well okay so here we go this is what you got weakness fatigue and erection nausea vomiting almost nobody has joint pain patient comes to my office says oh I just a call over I'm sure it's my adrenal oh it's your fibromyalgia go down the hall okay dermatology is down to all of us okay so adrenal insufficiency weakness fatigue anorexia weight loss patients comes to my office they're sent over they say Mary Jo gained 30 pounds in the last six months and she's feeling dizzy and fatigued she has adrenal insufficiency never on this earth even if you have congestive failure and adrenal insufficiency you lose weight because you have a sodium leak directly out the kidneys you don't have any aldosterone things don't go well the other thing you have is hyperpigmentation why well there's controversy about that so I'll just answer that for you the ACTH doesn't come pop out of the pituitary acth it's made as a large pro molecule that oozes out of the pituitary and is cleaved as it's leaving the pituitary and part of that molecule has melanocytes stimulating hormone capacity and so it stimulates the melanocytes and you turn brown so the ACTH is very high you're very reliable to get hyperpigmentation okay this is case two she's a 38 year old lady who came to the IDI with nausea dizziness outstanding weight-loss back pain for several weeks blood pressure 130 over 70 but no worth the static change her eat group was normal and someone got a random cortisol if I could just stop people from ordering random cortisol my life would be so much simpler it was zero leading to panic and a call the middle one night and I said well as she walked talking to you yeah she's awake and she's standing up oh yeah blood pressure is 130 over 70 had the cortisol may be zero but but but she has steroid on board somewhere right otherwise he'd be dead okay so just become patient comes to your office they're feeling a little funny you get a random cortisol right away that was a mistake but you get a random cortisol and it's point to forget it she's got steroid on board we had a guy who had a we couldn't figure it out he had a cortisol it was like 0.
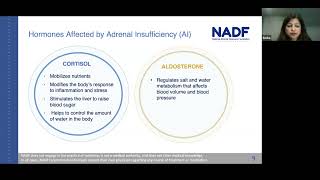
5 but he was perfectly fine he was asymptomatic there were no problems and I said somewhere you have steroids on board so he said no I don't use a dexamethasone inhaler no I haven't taken prednisone for poison ivy no one has injected me in the back or the hip or the leg with anything okay he had pericarditis and someone was injecting him to calm down the pericarditis with steroids took us about three or four weeks to figure that one out okay so look at this lady dr. Clark keeps telling us to look at these people and describe what we see well does that lady look like she stumbled into the wrong lecture why I know I'm taxing your brain here but but look at her she has a red round face look at those super clavicular fat pads folks this lady looks like she has heels temporal fat pads that are enlarged this lady looks like she has Cushing's right so what's she doing in this lecture well we took a history that was unique for the ER I learned here our Doc's here thank goodness they've all left early anyway that was that we went down and I said to the fellow take a history she looks cushingoid so why is she in here for adrenal insufficiency well over the past year she was getting prednisone 40 milligrams a day for connective tissue disease she decided wasn't doing her any good and stopped it oh hey that just makes you sick so we explained to her that was a poor move and left the year okay case three case three is anyone aged 25 to 70 comes to your office with complaints of nausea dizziness on standing weight loss fatigue who has just recovered from meningitis stroke traumatic brain injury all sorts of illnesses that affect the brain in total and those people can also get adrenal insufficiency now it's not from their adrenals these last two cases the adrenal isn't having problem the pituitary and the hypothalamus are shut off so the e group is generally normal and these people the ACTH maybe low normal the cortisol is just a little bit below normal something isn't working right okay so now we have a bit of boring biochemistry remember the hypothalamus makes kurtik control from releasing hormone that goes to the pituitary anterior pituitary causes you to make ACTH which goes the adrenal causes you to make cortisol and aldosterone to an extent most of the aldosterone is regulated by the renin-angiotensin system right right okay so only a third of its regulated by the pituitary so the aldosterone and the cortisol mostly the cortisol feed back to the pituitary and the hypothalamus all right so what happens in primary adrenal insufficiency like our first lady dreams gone so ACTH is high-court external releasing hormone is high and they don't make aldosterone because the adrenal is defunct so they get hypotension all right what happened to our second person pituitary was shut off by a large amount of steroid large dose history pituitary is shut off adrenal doesn't work very well minimal adrenal hormone production sometimes you can't even measure it and the cortex drove releasing factor is high the ACTH is low and the cortisol is low so they're both low its pituitary problem that's patient number two patient number three Oh traumatic brain injury I see that all the time because we take care of folks from fort hood which is one of the biggest army bases in the world a lot of sad traumatic brain injury and those people lose the higher centers and so they don't make corticotropin-releasing hormone well and so they make some and the pituitary makes some ACTH and the adrenal kind of gets the idea but these people sort of limped along and they're hard to diagnose and just initially in your office because this don't feel well and you say oh heck you're like the fibromyalgia lady that's telling me you have adrenal fatigue no no these people actually have adrenal directional problems it's like the lady who doesn't have regular menses and ovulation because her banana truffle releasing hormone isn't coming out right I think this audience kind of reflects with that doesn't it okay so let's go to what happens when you just measure a random cortisol I hope I've talked you out of there by now but but here you are in the morning you see the corn soul like the ACTH comes out and bursts so if you measured up here you say oh this is from a live house Cushing's syndrome if you measure down here you know say no no mrs. Schmidt alive has Addison's disease or adrenal insufficiency so one random cortisol doesn't do it you have primary adrenal insufficiency and it's low and a tandem ACTH is high you've got the diagnosis secondary and tertiary neural insufficiency you can't do the random cortisol so please don't waste everybody's money getting that so what do you do you stimulate with ACTH so and ask you what happens when I give you AC th do you make cortisol doesn't matter you yes you do I have to answer my own questions here that's alright yes you do if I give you AC th early in the morning while you make cortisol yes you will if I give it to you after lunch will you make cortisol yes you will if I give it to you when I've given you a big dose of steroid yes you will but I don't be able to measure it cuz I gave you a big dose of prednisone across reacts so again whenever I give you ACTH you will make cortisol if your adrenal is working so you use the business part of ACTH which is courtesan and you give it and you measure this cortisol at 30 and 60 minutes and if is 18 to 20 the patient does not have any problems and I don't care if they are fatigue and nausea and weight no no they don't have any problems okay so what is a normal stimulation test there you go I give you ACTH you make cortisol how about primary adrenal insufficiency I give you AC th let me see if though that doesn't look like it's doing well here I gave you AC th and I get nothing as a matter of fact they wept that off the bottom of this line and if you have secondary or tertiary adrenal insufficiency I get something but nothing like what I should have gotten okay so you can differentiate those two with a courtesan stimulation test what's this microphone says its battery is dead can you still hear me yeah okay okay alrighty so ACTH is the key to location if it's high it's primary if it's low its secondary or tertiary so you get if you're going to persist and get that 8 a.
m. cortisol get the ACTH it tells me where it is high primary low secondary or tertiary so what causes primary adrenal insufficiency well in the United States autoimmune disease far and away congenital adrenal hyperplasia is and in ability to synthesize cortisol and aldosterone if it's total gives you primary adrenal insufficiency but it's found at birth and so if you're not a neonatologist you can forget that one worldwide tuberculosis is one of the most common causes of primary adrenal insufficiency goes into the medulla destroys the medulla and the cortex secondary adrenal insufficiency Oh far and away you cause it actually the rheumatologist the gastroenterologist cause it people giving folks injections with steroids steroids or poison ivy steroids or bronchitis cause adrenal insufficiency so again that's the most common kind in the United States you can also have pituitary surgery hypothalamic trauma again but not very common so how are we going to treat this primary adrenal insufficiency requires both something to replace cortisol and something to replace aldosterone so a glucocorticoid and a mineralocorticoid secondary and tertiary adrenal insufficiency are usually diseases from which you recover and they just require glucocorticoids well in texas sometimes it's really hot people get dehydrated I give them a little bit of mineralocorticoid for the most part secondary and tertiary require only glucocorticoid replacement and the patient may recover primary adrenal insufficiency requires both glucocorticoid and Marinella corticoid replacement patients don't recover very very seldom to recover from primary adrenal insufficiency or adrenals gone that's it now the other thing you need to teach is people about emergencies and I know that bracelets except fitbit's although I had a guy with a Fitbit that has it's adrenaline sufficiency tag on it you've got to have a tag a necklace somewhere we've got to know your phone isn't going to work you have an automobile accident they leave the phone on the seat they bring you the ambulance somewhere we need to know you have adrenal insufficiency because you only have steroids and on board for one day it's an intensive care unit we got to figure it out it's a paint on that could cost a lot of money and you may die so I convinced my patients to wear some sort of a tag or a necklace telling folks they are steroid dependant and have adrenal insufficiency how do you replace them glucocorticoids I've just told you hydrocortisone 10 to 20 milligrams in the morning 0 to 10 milligrams in the evening prednisone is five to seven and a half milligrams a day those are the two you oughtta use you don't want to use unusual things to replace adrenal insufficiency divided doses are given and you're going to get the last dose in the afternoon because you can create a insomnia out the wazoo by giving the last dose as the patient goes to bed it'll keep you awake they're really great if you can't wake up steroids are a really great way to do that no just kidding okay so if you want you can try a single dose in the morning to help with compliance if they always forget the afternoon dose how much well I gave you the doses but really probably we're treating people with too much which is the other thing the endocrine Society said we have to emphasize too much steroid and most of our patients hydrocortisone 20 and 10 is probably too much and if you see signs of cushingoid features you get the red face you get round patients begin to get a little upper abdominal obesity try and reduce the dose particularly the evening dose also make sure the patient has an injectable steroid they know how to use in case they throw up for a whole day how long does your POS steroid last one day so if you throw it up all day you're going to be stirring deficient you don't want to end up in the IDI so please show them how to use Sonya cart if it's really easy you can get it in a prefilled syringe in most pharmacies and tell them when to double the dose you don't double the dose when you're dumping dyes or when you break your tote you double the dose when you have pneumonia Titus you tell the anesthesiologists when you're going to surgery so they can give you a bolus it's for really significant events you double the dose mineralocorticoid replacement is only indicated we said in primary adrenal insufficiency and you use Florin if there's only one thing fludrocortisone and you have to tailor it to the patient and you start out with point zero five milligrams a day some of my older patients that have fluid retention only need to take it twice a week some people need to take more depends on whether you're salt sensitive or not so just you have to tailor that to the patient start off low and if their feet begin to swell up produce the dose if they're hypotensive or the potassium is high you raise the dose okay now how about you've put somebody on steroids and you need to get them off well mainly you're putting them on steroids for something right I mean you just didn't do it because you felt like it on Tuesday you're putting it on because they have polymyalgia rheumatica they have polymyositis they have you pick pain and you injected them so you're giving them extra steroid because of an underlying condition injectables taper themselves so you don't don't worry about that but if you're giving them pio steroids and high-dose you can taper down to replacement doses you just look down on the previous slide replacement dose and then you've got to be careful of adrenal insufficiency down to replacement dose you're tapering to based on the disease you're tapering on based on the disease you don't want to get flares in the disease you're going to taper down to replacement dose and then you say gosh patient is better from there underlying disease I want you I get these people my office Andros to get them off steroids okay I'll do it and how you do it remember the view treated them for more than replacement for more than three weeks they're going to need to have a little taper so if you're gonna if you give people something for poison ivy your bronchitis oh I beg of you use one of those packs that just tapers itself because then you have to worry about it I mean they really do work they they're actually evidence-based so I'm just going to put on high-dose or something for a long time like polymyalgia rheumatica we're probably going to have to taper them very gradually off once they get to replacement dose so how do you do it everybody has their own way to do this every endocrinologist I've ever talked to has their own way to do it this is my partner's way she likes this one better and I said okay you find the smallest dose you can like one or two and a half milligram tablets and you have people back off remember the half-life of prednisone for example is 12 hours so every three days you have five high flights you back them off by one tablet either in the morning or the afternoon you alternate back and forth morning or afternoon and if they get sick you go back to the previous dose and what I do is I actually take the I print out a sheet so that they know where they're going and I print I put dates on it so they know on what date they're gonna be taking what dose and it's pretty effective in getting them off you probably ought to keep the a. m.
Related Videos
1:03:19
Living with Adrenal Insufficiency: Underst...
NADF
8,645 views
51:22
Evaluation and Management of Adrenal Insuf...
MedStar Georgetown Department of Medicine
8,066 views
51:32
Adrenal Insufficiency | Clinical Medicine
Ninja Nerd
78,175 views
23:43
Understanding Cortisol and the Adrenal Axis
Zero To Finals
42,060 views
1:41:04
2024 Secondary Adrenal Insufficiency, Dr. ...
Acromegaly Community
1,248 views

14:27
How to Raise Cortisol Levels Naturally
Dr. Kate Lyzenga-Dean
10,662 views
11:59
Primary adrenal insufficiency (Addison's d...
Osmosis from Elsevier
748,977 views

21:07
My Story: Adrenal Fatigue | A Thousand Words
A Thousand Words
244,233 views
10:04
NEW: My Life-threatening Condition Explain...
That Tilly Rose
23,477 views

24:15
Symptoms of Adrenal Fatigue
Peter Osborne
23,467 views
27:07
Hyperaldosteronism | Clinical Medicine
Ninja Nerd
37,059 views

1:23:19
#411 Adrenal Insufficiency with Dr. Atil K...
The Curbsiders Internal Medicine Podcast
5,621 views

56:44
Everything you need to know about Cortisol...
Precision Analytical, Creators of the DUTCH Test
7,863 views

58:42
Adrenal Insufficiency with Dr. Basina
Health4TheWorld Academy
1,909 views

35:22
Cushing's Syndrome and Disease | Clinical ...
Ninja Nerd
92,938 views

53:16
Wired and Tired: Fixing Adrenal Burnout
Mark Hyman, MD
245,405 views
31:42
Adrenal Insufficiency with Dr. Malika Rawal
UofL Internal Medicine Lecture Series
6,336 views

1:04:49
Adrenal Insufficiency and Cortisol Replace...
Raymond A Wood Foundation
9,224 views

13:58
NEW: My Addison's Disease Journey
That Tilly Rose
27,730 views

14:28
What Is an Adrenal Insufficiency? (Seconda...
Fashioneyesta
11,201 views