Normal Skin Histology - Explained by a Dermatopathologist
316.72k views14784 WordsCopy TextShare

Jerad Gardner, MD
A complete organized library of all my videos, digital slides, pics, & sample pathology reports is a...
Video Transcript:
Alright I'm Jerad Gardner and today we're going to talk about normal skin histology. So this is the skin and what we're looking at up top the purple layer up here that's the epidermis the top part of your skin that protects you from the outside world. Underneath that all of this pink that's the dermis made mostly of collagen and its job is to support the epidermis and there are blood vessels here and other things that support and make sure the epidermis stays happy. And then when you go down below, deeper down below. Well there's not on
this slide but there should be fat down in the subcutis. We will look at that in a minute on another slide. So let's go and take a closer look at the epidermis. A lot of skin diseases involve the epidermis. Rashes, dermatitis, all these things and also lots of different tumors come from epidermis. If you want to be good at skin pathology, dermatopathology, you have to be a master of normal skin histology. If you don't know what normal looks like it's really difficult to know what abnormal looks like. Alright, so there's little color changes in light
changes there as I'm changing my objectives and that's why that's happening. Alright so let's look at will go at one closer than this. Let's look at the layers of the epidermis okay. There are in the skin cells begin their life down here at the bottom this is called the basal layer of the epidermis it's the bottom layer or the stratum basale if you like the Latin names for things. In the basal layer there are occasional little stem cells in here that give rise and reproduce and dividing give rise to squamous cells. So the epidermis is
a stratified squamous epithelium it means it's stratified means multiple layers you can see there's layer after layer of cells here so it's stratified and it’s squamous that's the type of cells these are kind of they’re round or some people say polygonal shape meaning they look kind of a little bit like a maybe a hexagon or a pentagon or something if you have a really good imagination. And they’re pink because their cytoplasm is filled up with cytokeratin which is an intermediate filament and that filament acts like strong kind of you know steel cables basically going back
and forth across the cytoplasm hooking up to desmosomes around the cell membrane which then hook up to neighboring desmosomes and all of that together makes that the epidermis a really strong network that resists damage from friction or pressure. So that's why when you rub on your skin it doesn't fall off. Okay so anyway back to what we were talking about here the basal layer of the epidermis the cells there they begin their life and then they start moving up there pushed upwards by the production of new cells and as they move up they go into
a new layer this is called the spinous layer or the stratum spinosum. And the reason it's called that is because there are actually little tiny spines which are desmosomes in between each of the cells. You can barely see them here we’ll look at another a slide in a minute that shows that much more clearly. And you can see the nice round nuclei of the cell and then as the cells get up towards the top they begin to pick up these purple dark purple granules in their cytoplasm and so this is called the granular layer. It
makes sense right because they have dark granules in the cytoplasm these are these are keratohyalin granules. Keratohyalin granules contain a variety of different substances like loricrin and involucrin, kind of fancy things like that that dermatology residents need for their board exam but probably medical students don’t need to know. But the job of those granules is to kind of help the keratinocytes come to the end of their life and die and lose their nucleus and the skeleton of proteins left over from inside the cells gets transferred up here and becomes the corneal layer or the stratum
corneum and the granular layer kind of helps seal these cells together, kind of cements them together like with glue. And the reason that we do that is because you don't want, you know, water things that are outside this is like an extra barrier against them. And then a water things like that getting past your epidermis. So that when you rub your skin and those little dead cells flake away from the skin that's what's flaking away there. That's the corneal layer. That layers actually dead it's not living any longer and so that eventually will fall off
over time. The time it takes for a squamous cell to get from the basal layer, where it's born all the way up to the top where it kind of dies and becomes the stratum corneum is roughly 28 days depending on what source you ask. Now in some diseases the epidermis starts growing really quickly. For example, psoriasis it takes about 7 days from when a squamous cell goes from the basal layer up to the top. And then this little pink line here that you see this is known as the stratum lucidum. And even though that that
name implies that it's clear or easy to see through, it's actually usually more pink than clear. And there's only two situations that you actually see a stratum lucidum in the human body. Number one is on acral skin, the skin of the palms and soles. And number two is any skin that's been rubbed or scratched chronically begins to get a thicker granular layer and it begins to get a stratum lucidum. And eventually if you rub and scratch skin long enough the whole epidermis will thicken and begin to look like the skin of the palms and soles.
And that's a protective mechanism to avoid injury of the skin. Now a couple of things we can point out about the epidermis while we're here. Number one there other cells that live in the epidermis, not just keratinocytes. So these squamous cells are keratinocytes, those names are interchangeable. They make up the bulk of epidermis, but we have a couple other neighbors here that that play a role in the epidermis. So this one guy right here you can see he’s kind of gray, it's a little hard to get him in focus, but he's a little bit gray
and not quite as pink. And he has a little vacuole around the outside, that little white space, that's an artifact of a tissue processing when we soak the tissue. You know tissue doesn't come out your body pink and purple like this, we have to actually soak in formaldehyde or formalin and run it through a series of different chemicals to make sure that the tissue doesn't break down. And then we dip it in a series of stains. And so this pink and purple stain that we see here is called hematoxylin and eosin, or H&E. So the
H&E stain is probably over 100 years old and we've been doing it relatively the same way for about 100 years. It's still it's that the bread and butter of what we in pathology is look at tissue under the microscope on H&E. So a lot of people think pathologists just do autopsies all day long, some of us do, but I haven’t done an autopsy in a long time and what I do is look at biopsies from living people mostly from their skin and decide if they have cancer or not. So that's the kind of job pathologist
do. But anyway back to this little cell here, this little gray cell does have a vacuole around the outside and that that's an artifact in the reason he has that vacuole is because if the cell shrinks during processing and its cytoplasm clumps up to the nucleus and the vacuole forms are on the outside because it doesn't have any desmosomes to hang onto its neighbor. So that's a melanocyte. Melanocytes are not hooked up to their neighbors. In contrast look at these nuclei are over here these are keratinocyte nuclei and they actually about little halo, a little
vacuole around their nucleus. The nucleus is kind of naked floating in the middle of that little space, that's because when they shrink up all of their cytoplasm is hooked up to the desmosomes of outside of the cell and it can't go anywhere. It's attached to all of the neighbors. So that poor little nucleus shrinks up it is naked and alone. So when you see vacuoles in the epidermis and you're trying to decide is it a keratinocyte or a melanocyte. If they have the little halo right around the nucleus, it's probably keratinocyte. If the nucleus as
a little blob of spidery cytoplasm around it, like that guy, it’s probably a melanocyte. So these two guys here are melanocytes. And normal melanocytes live along the basal layer. Here's another one there. You can kind of tell because you would think melanocytes their job is what it's to make melanin pigments that makes your skin turn colors when you when you tan your skin gets darker people that are have brown or black skin darker skin patients they have more melanin production not more melanocytes. But they're melanocytes are just more active and make more melanin pigment. But
you'd say well why are the melanocytes gray and not brown. That's because the melanocyte has an unusual job. It makes melanin pigment and then instead of keeping it and hoarding it all to itself, it actually shares it with all of the keratinocytes around it. So these little finger like process called dendrites. And it sends these all dendrites out to the keratinocytes it live directly adjacent to it. And the keratinocytes actually kind of eat the little fingers off of those little dendritic branches and that's how they ingest on the pigment into their cytoplasm. So you can
actually see this here it's a little easier in some places. Here we go. If you look at these cells right here let's see if we can get maybe one higher. One higher power, a little closer view. So this is 600 times magnification. So we don't usually use this in real practice but for a video this'll help. What you can see is that these cells. Oh hold on, I've lost my arrow, there it is. If you can see the cells right here, see how they have a brown pigment in the cytoplasm. That pigment is kind of
over top of the nucleus. You can see it up here too. It's kind of like a little umbrella or a cap. And if you look, if you go up this way, that's where the outside world is. That's where the sun is. So the sun would come down and would normally hit these little keratinocyte nuclei. And you know sunlight contains ultraviolet rays and ultraviolet rays damage DNA, and the DNA of cells lives inside the nucleus. And if you damage that DNA you get skin cancer and things like that. So the job of melanin is to kind
of try to protect your skin to absorb some of that light and protect your skin from the damaging rays the sun. So I like to think of it is that the melanocyte makes the pigments. So here's another melanocyte. You know how I know? Look it's got a vacuole on the outside and then a little blob of but gray cytoplasm stuck to the nucleus. Okay. So he feeds the melanin to all these keratinocytes around him. I don't know that the cells are actually all boys, but I just like to talk to them like the cells are
people. If you're a pathologist too long that's all happened to you too. So I'm just kidding. Okay, anyway, the pigment up there, that little it's like a little hat or a little umbrella I think to protect the nucleus of the keratinocyte from the sun. So when you see a brown pigment cell in the epidermis, it's actually probably a keratinocyte, not a melanocyte. You would think that it should be melanocyte. So you know with a little practice you can do this. That little gray guy out there, that's a melanocytes. All these guys appear that a brown,
those are keratinocytes. Okay so we said there are several cells that live in the epidermis, there's another one too. Let's see if we can find one of them. And we might have to hunt around a little bit. In the mid-level of the epidermis near the spinous layer, we have a type of cell, that's probably one right there is a little hard to see him. But this little cell here that has a little bit of a kind of bean shaped nucleus, that's called a Langerhans cell. So Langerhans cells are basically, they're kind of related to histiocytes
and macrophages. And they live in the mid-level of the spinous layer. And the reason for that is that if the skin barrier function breaks down antigens, things from bacteria, fungus, stuff from the outside world, will come through the skin. And the Langerhans cell, their job is to cut it eat that stuff up and break down the proteins. And then they come out of the epidermis and go into the dermis, into lymphatic channels, and go all the way back to lymph nodes, and then alert the immune systems and basically say, “Hey here's some stuff we found.
Should we, should the body fight against this or not?” And then the immune system decides whether or not it's a bad thing or a good thing. And so that's why the Langerhans cells live in the epidermis because of the first line of defense against an incoming infection or allergen or something like that. So they are antigen presenting cells, and they are basically related to histiocytes, and they live in the mid-level of the epidermis. And they are a lot easier to see on immunostains. You can the stains for S-100 protein or CD1a, which will highlight those
Langerhans cells. In some diseases, like some rashes, like contact dermatitis, you tend to see lots of Langerhans cells. And we will look at that in a minute. So that's the epidermis. Now let's move down into the dermis and see what's down here. The dermis has, we'll go one lower power, the dermis has two different parts. The first part is called the papillary dermis, and the second part is called a reticular dermis. And the way to tell them apart is this… Well we actually didn't talk about one thing about the epidermis I forgot to mention. You
can notice that all of the epidermis has these little fingers that point down. There is one. There's one. There's one. Here's one. There's one. There. There. There. Those are called rete ridges and most areas of the skin have these, little fingers that kind of undulate down into the dermis. Those are rete ridges. In between the rete ridges, the pink stuff, is part of the dermis. And that part of the dermis is called the papillary dermis. And each one of those little pink fingers pointing up in between the rete ridges, each one of those is called
a dermal papilla. And the dermal papilla has an important job. Look what's inside of each papilla. This is kinda hard to see, but this little tiny area in the middle, that's a little tiny blood vessel or little capillaries. And the reason capillaries are right here, right next to the skin, is because inside of the epithelium, in the epidermis that is, you don't have any blood vessels. So the way that the epidermis is nourished is by absorbing oxygen and nutrients from blood vessels that are located just below the epidermis. And so these blood vessels here basically
bring oxygen and nutrients, and that soaks out across this little space here and gets up in the epidermis and feeds those cells. And then it also takes away waste products from the cells. And that's true of all epithelia lining layers in the body. They don't have blood vessels within the epidermis, I’m sorry, within the epithelial layers. They always have in the stroma or the underlying supporting collagenous tissue that basically provides a supporting structure for the epithelium set to live and grow on. So the collagen, this little pink, the little pink fibers here, that you're seeing
this is collagen. Okay collagen is one of the most common proteins in the human body. It's all of the soft tissue, and your bone too. All of the supporting tissues in your body are mostly made up of collagen, which are really strong kind of protein fibers. And you can see that they're kind of, these fibers in the papillary dermis, the fibers are very small and thin and fine. And as you go deeper into the dermis, all of a sudden the fibers become much bigger, darker, pink in color, much larger. So this is that the reticular
dermis has really thick fat collagen fibers, and the papillary dermis has really fine collagen fibers. So you can tell the papillary dermis apart because it's actually up it's the layer that's right up here in between the rete ridges. But you can also tell it apart because it has really fine, delicate collagen, whereas the reticular dermis has really thick, fat, big collagen bundles. And the other thing is a little layer of larger, not larger but larger than these capillaries, a little bit slightly larger vessels appeared. There's a vessel there. Here's a blood vessel there. Blood vessels
here. So this layer of blood vessels runs along the whole area of the skin right underneath that separates the papillary dermis from the reticular dermis, and this is called the superficial vascular plexus. It's a branching network of blood vessels that runs right underneath there. Its job is to kind of feed blood up into the dermal papilla a so that the epidermis can get nourishment. Okay. So that is the papillary dermis. And then down here we have the superficial vascular plexus. And then underneath that we have the reticular dermis. Okay, the reticular dermis is kind of
the main supporting structure of your skin. It's the thickest layer until you get down to the fat, and what you have is some larger blood vessels in here. Let's take a look at one of these vessels. So this empty space is a blood vessel. So whenever you see a white space on a histology slide, what you're seeing is nothing basically. White is basically clear in histology. It means the white light for the microscope is coming straight through with nothing blocking it. So if you have a white space on a tissue slide, it's always one of
3 things. Either number one, it's a vascular channel, lymphatic or vein or artery, a lymphovascular channel, and that's what we have here. And we know that that's the case because the space is lined by a thin single layer of endothelial cells on the outside. That's the lining cells of blood vessels and lymphatics are called endothelial cells. And you can even see that little red guy in there, that's a red blood cell. So normally these are filled with red blood cells, but during processing some of that blood washes away and then oftentimes they leave empty space
instead. So that's one thing an empty space can be, a vascular space. Number 2, we're going to move to a different part of the slide to show you. Well hopefully we have one… Yeah. Number 2 empty spaces can be lined instead of by endothelium, they can be line by epithelium. And we can tell that this is epithelium because it's a couple layers thick and has a lot of extra pink cytoplasm around it. And actually in the middle of this little space is also some little bluish goo. That's actually sweat. These are actually sweat glands. We
will come back to in a minute. So the other times when you see a space that's not lymphovascular, that space would be a glandular or cystic space that's line by, not endothelium, but by epithelium. And then the third time that you see a white space is what we call artifact. That means that there's something that used to be there in the tissue that either dissolved during our tissue processing procedure in the pathology lab, or the tissue tore or ripped when we tried to cut it because they make these slides, we cut thin little slices, just
like you take a slice off of a piece of our lunch meat or salami, only instead of being that thick it's actually, these are four micron thick sections. Four micrometers ,very, very thin. That should have to be a topic of another video for how we do that. But see these cells are here, these are fat cells. These inside the human body, in real life, these are filled with fat, with lipid. But during processing, the chemicals we use dissolve the lipid and leave an empty space there. So even though this looks like white space, this wasn't
white space inside. Wasn’t a hole or a space inside the patient, there was actually fat filling the space, but now it’s artifact we washed out. So sometimes artifacts are a sign of a certain type of cell, like fat cells, and other times I think we had a piece up here, like that, that white space right there. It's not line by any layer. This is a break, a little break, or tear in the tissue. When we cut the tissue, it folded and ripped a little bit and it left a space there, and that's just an artifactual
space. So now you know if you see a white space and tissue is one of three things: a lymphovascular type space, a glandular or cystic type space, or an artifactual space, that's an artifact of our processing. So let's get back to blood vessels. Here are vessels here. And in fact, we have kind of a little cluster of things here. We have a small thin walled blood vessel, and then this vessel is actually a little thicker wall. This is probably an arterial of the tiniest branch out of an artery. This is probably a little venule or
a small vein. So that arterials are bringing blood from the heart out to the tissue and then the venules are bringing blood back to the veins, which will drain back into the circulatory system. Sometimes when they're small, it's hard to tell arteries and veins apart. When they're larger, it's easier. But these are both vessels of some sort, and you can see that they've got the little luminal lining of endothelial cells, and then this little structure right next to this, is a nerve, a tiny little nerve. These are Schwann cells, and around the outside of the
nerve is a thin layer called the perineurium. And the nerves, there's another little tiny, tiny baby nerve right there, it's hard to appreciate, but nerves run next the blood vessel. And so together that's called a neurovascular bundle. And kind of we see this throughout the body, for all the way from the really large vessels all the way down to the tiny ones, that nerves and arteries and veins, they have a tendency to want to run together in little, in a little group together, they kind of travel together throughout the body. Okay, so we talked about
the dermal reticular collagen, we talked about vessels, and we talked about a little bit about nerves. Here's that vessel we started on before I got distracted and look great there is another up above it you can see this vessel, the cells are little more plump, but it's just a single layer lining cells. That's a good sign that it's going to be a blood vessel space okay. Let's see. Okay then we have another type of bundle of pink stuff here, this is some pink bundle that looks a different shade of pink than the collagen. The dermal
collagen is right there, and then this bundle of kind of organized like lighter pink color, and it's made of these spindled cells, these elongated cells that are kind of running together in the same direction. This is smooth muscle. And in the skin, smooth muscle is in one of two places. It's either in the blood vessel walls or it's in these little bundles called arrector pili. And that's true of most skin, there's a couple exceptions and a few other places have extra types of muscle like the nipple, the scrotum, and the labia of the female genitalia,
those all have extra smooth muscle bundles. But elsewhere in the body, you just have these bundles which are arrector pili muscles, or you have smooth muscle that are in the vessel wall. So arrector pili, you can kind of see here, it's getting close to hooking up to this sebaceous gland, which is hooked up to a hair follicle. So these muscles, when they contract, they make your hair stand up straight and that's why you get goose bumps or why the hair stands up on the back of your neck when you're scared or something like that. So
those are those three pink bundles here, those are called arrector pili muscles. Right, this we talked about. I mentioned it briefly. This is a sebaceous gland. So this is a lobule, a cluster of cells together and these cells have a very different look than anything we've looked at yet. Each individual cell has a tiny little white space in it. Those little white spaces are also artifact. This is because there used to be lipid or fat in here, so that each cell, here's one whole cell, this one right here is one cell. It's got a nucleus,
the little purple thing. And then all the cytoplasm is completely filled up with these tiny white little bubbles. And these are perfectly round because these were fat in the human body is made up of water, and when you mix oil or fat with water, what does it do, it makes perfectly round little droplets, little spheres. So anytime you see a perfectly round little white circle inside the body, it's usually a good sign that you might be dealing with something that was fat that's been dissolved during processing. Because fat only can make little perfectly round droplets.
So these cells are called sebaceous cells or sebocytes, and their cytoplasm is filled with little tiny vacuoles of fat. And when these cells, we will look at it another section, when these cells all break down, they come, they squeeze out of the gland into the hair follicle and they make a type a secretion called sebum or sebaceous secretion. And so this kind of secretions are more common in the groin and the axilla and the kind of, you know, the kind of place of the body that don't smell quite as nice. And the reason that happens
is that the sebaceous secretion when it comes out on to the skin surface, certain types of bacteria break it down and make it smell bad because it makes bad smelling compounds and so that's where body odor comes from. It might be kind of gross but it's important to understand where all these things, why all these things happen. So anyway, these are sebocytes and this is a sebaceous gland. Around the outside of the gland, the cells are a little bit more blue and what we call basaloid, so that's kind of the what we call the germinative
layer there, the layer of cells that give rise to the more mature sebocytes. And then as the cells mature, they pick up lipid in their cytoplasm, become more white and bubbly looking. Alright so that's a sebaceous gland. Over here you can see, oh this is nice, here is a hair follicle. Let's go to a lower power, and you can see that this is a follicle, but it doesn't look to connect the surface. And that's one thing that's a little hard for some people to learn about pathologies, you have to think a little bit. We're looking
at a 2 dimensional slice of 3 dimensional tissue. So that follicle definitely connects up to the surface, you can kind of see the top of it up here, it just kind of is out of the plane that we slice through. So if you sliced a little deeper, you might see where it actually starts to connect up to the top there. So you have to get kind of used to looking at pieces of things that are always perfectly showing the entire detail. But here you can see it kind of the base of one of these hair
follicles, and in the center, this little piece right here, that if you kind of put your finger underneath the light you can kind of see it kind of move in and out, that is actually the hair shaft. That's a hair shaft, that's what your hair looks like inside your skin, and the follicles, this layer of epithelium surrounding the hair shaft. And you can see the sebaceous glands, one here and one here. Their job is to drain straight into and kind of coat the outside of the hair shaft. And so that sebaceous secretion will drain into
the follicle and it come out of the top of that the follicle on the skin surface right around where the hair shaft exits. And see here's the opening of the follicle. So we will look again at follicles in a minute. We covered many of the structures. I think we have one more, one I wanted to show you in here. Oh yes, these. So this, I said earlier, I showed you that this is a sweat gland. This is an eccrine sweat gland. The kind of liquid-like watery sweat that you get when you get sweaty palms, if
you're nervous, that comes from these glands. And these are called eccrine sweat glands, or the word we often use the eccrine coil because what it is a simple little gland, a tubular gland and that's all tangled up into a coil and it makes the sweat. And then the sweat is secreted out through this little tube called the duct, the sweat duct. And again, you can’t see all the sweat ducts travels all over the surface, it kind of seems to disappear. But it goes all the way up to the surface and empties out. And if you
look around we may be able to find another one where another one empties out. Or maybe we won't. Maybe this piece of tissue doesn't have one. You don't always see every structure that you're looking for on every piece of tissue. Alright, well we will have to see one in another piece of tissue. So here, these eccrine coils they have a unique kind of lining. They're lined by a double layer of cuboidal epithelium. So cuboidal cells have round nuclei, and kind of are slightly square or cuboidal in shape. Now I know you have use your imagination
to think that these are square but they're kind of, they're not taller than they are wide, like a columnar cell would be. So you can see that they have these rounds nuclei, and they're kind of 2 layers of them. I think you can best appreciate the double layer here in the duct. So you can see the double layer here, the inner layer, is this layer here, that's more pink, and this outer layer, which is actually made of a special cell type called myoepithelial cells. They kind of have a little bit of contraction properties supposedly. I
don't know how much of that it's actually used here but they do have some contractile filaments in them, so they have a little bit of muscle like quality. So anyway that's the myoepithelial layer on the outside or the basal layer, some people might call it. Then the inside is the apical layer, these larger nuclei with pink cytoplasm. So it's double layer cuboidal cells, and really there's only, I think, there's only two places you really see that in the body that I can think of. I'm not a histology expert, but I do look at a lot
of tissue. You see them in the ducts of sweat glands, and you also see them in the ducts of the salivary glands. You can see kind of a double layer of cuboidal epithelium and that's I think because the sweat glands and salivary glands have a lot of things in common. And when you get tumors in your salivary glands, they tend to have a lot of overlapping features with tumors that grow on the skin from sweat gland origin. And this is a good example of, here is lumen, the center part of a gland or center part
of a vessel, so that anti space we call lumen. So this is a lumen and then here is the sweat ducts and out here is a comparison. This is a blood vessel space, see it's got a red cell in it, and it's got one layer lining it. You might say, “Well what about this out layer here?” That's actually, those are modified smooth muscle cells called pericytes. And that's a little thin layer of muscle around the outside of the vessel. So if you did different special stains, immunostains, you can show that this is made of epithelial
cells and this is actually made of endothelial cells and muscle. And then right up above we have a nerve. There's a tiny little nerve right there. And another you can compare, this is nerve. And this is smooth muscle. And actually another thing one of my professors, Dr. Jae Ro, taught me lots and lots of histology. He liked to teach triads. And he said that whenever you see pink bundles of spindle cells in the human body, they’re one of three things. Number one, they’re dense regular connected tissue, they're made up of dense collagen. And so even
if this isn't really a bundle, you can see this dense pink here, that's collagen, like the dermis is made of. Number two, they’re nerve. This is nerve right here and you can see it's nerve lined by this little layer perineurium on the outside and it's a little hard to tell nerves when they're small. When they're bigger, it gets easy to see. We will look at a bigger one in a minute. And then over here, this is smooth muscle, arrector pili. The cells have more of a kind of cigar-shaped nucleus, the cytoplasm is a little bit
different color. So you can see right here, collagen, nerve, smooth muscle all in one picture. And there's a little blood vessel up there. See you guys are probably already pros. You starting to probably recognize all the structures, it just takes practice. But looking at the stuff in real life. So there's that eccrine coil. And that eccrine coil usually resides deep in the dermis, right at the junction between the dermis and the subcutis. And you can see there's a little bit of fat. This stuff here, these are adipocytes, and this is a little pouch, outpouching of
the subcutis, where the fat kind of pushes up and surrounds the eccrine coil. But usually, when you're down to the level of eccrine coils, that means you're almost at the bottom of the dermis and you're about to enter into the subcutis. And when this skin excision was done, there was cut at the level of the deep dermis, and so we don't actually see any subcutis here. That black stuff is ink that we add in our laboratory to help us see where the edge of the tissue really is, the true edge the surgeon cut. Or the
dermatologist in this case cut. So that is enough from this piece. Let's move to another piece of tissue. So this is an example of acral skin, skin on the palm or sole. And you can tell that because it's got a very thick corneal layer here at the top. It's got that stratum lucidum that we talked about previously. And the reason I'm showing this, this is actually not normal skin. This is skin that's involved by contact dermatitis, like you get if you touch poison ivy. And there's some extra white space up in the surface here, that's
making a little blister. And there’s some of this stuff that's called parakeratosis. We can go closer and look. So normally you don't have nuclei left in the corneal layer, but when skin gets irritated, and starts growing quickly, the nuclei get retained. We talked a little bit about that earlier. The granular layer kind of goes away, or gets diminished, and that parakeratosis, the presence of nuclei in the corneal layer, shows up. And so that's a sign that the skin’s abnormal, that's not a normal finding. To have parakeratosis means the skin's been irritated from dermatitis or rash.
Or it's a tumor or a pre-cancerous, growth something like that. Right. And then here in the dermis, you can see that around the vessel, see here's a little blood vessel, right here little thin one, but rather they're all these blue cells. Those blue cells are lymphocytes and maybe some histiocytes, also macrophages if you like. The reason I show these is that even though these are, when we have a lot of them it is kind of an abnormal finding, almost all skin that we see biopsied has at least some degree of lymphocytes around the vessel. So
a little bit of lymphocytes is actually normal, and it's not anything to get too worked up about. So we see these blue cells around vessels, they're probably just lymphocytes. Don't be too concerned. And they're also the other reason I show this… Ah here. See we will go higher power and see if we can see them better. These bright little guys here, it's really hard to pick them up because their granules don’t show up, but they’re bright orange. They’re like brighter than, those are red blood cells. These bright orange cells, these are eosinophils and they have
two lobes of their nuclei, looks like little pair of like aviator sunglasses or something. And then they have these bright orange granules. So eosinophils are involved in a variety of processes, including allergic processes. So in this case, this is allergic contact dermatitis, that's why they're here and also they're involved in fighting off parasites and other things like that. And then, sometimes you talk about neutrophils. So in contrast, these dark guys that are almost purple and black in color, those are lymphocytes. See that guy, there, that has multiple nuclei, that's actually a neutrophil. And he's just
there in a blood vessel. That's normal. When you see a lot of them that usually means something else. Alright, so the reason I want to show this slide is that when you go over here, there's this space and looking next to the space, you can see there's a lot of extra white space between each of the keratinocytes in the epidermis. And this is called edema, or when edema is present in the epidermis, it’s called spongiosis. And so spongiotic dermatitis is things like eczema or eczematous dermatitis, atopic dermatitis, contact dermatitis, there's a large number of different
rashes that give you this finding microscopically. The reason that I'm showing you in a normal histology video is that when you look at this on higher power, what you can see, it's hard to get a focus, but between each keratinocyte, see those little lines. Those are the spines. That's why we call this the spinous layer because those spines, those are desmosomes. And you can see them much more clearly, when they're stretched out by all that edema fluid in between each individual cells. So that space there is because of all the fluid that's pushing apart, but
it lets you really see how prominent those spines are there. Usually kind of difficult to see on normal skin, but here when you have spongiosis, it's a nice way to showcase just how dramatic the spines are. And they're really strong because even though they're being pulled apart by all this fluid, they're holding on for dear life to their neighbor. And sometimes when they get pulled too hard, they lose connection and that's when you get this little blister here. That's when you get these little bumps. And those little cells inside there, these are Langerhans cells. And
so we talked about Langerhans cells living in the on mid-level part of the epidermis, and the reason they live there is because when you get contact with, when you touch an antigen, those cells go in and find that antigen and eat some of it and then take it back to the lymph node and shows the immune system to see if you should mount an immune response. So these little guys here, those are Langerhans cells. And they're kind of collecting together, and in contact dermatitis, you get that. Again look at these beautiful spines. There's really, really
very nice example. And a look that's a mitosis too while we’re here. See that’s a little mitosis that's probably in anaphase. It's on its way to becoming two new daughter cells. So this skin is revved up and irritated, and so it's dividing and making new cells to try to repair itself. Alright, so those are the spinous processes. Now let's look at some more acral skin. And this is normal acral skin, look for low power. And again looked the really massively thick and a corneal layer, you can see this pale line here that's the stratum lucidum
again. Only place that's really present in the body normally is acral skin on the palms and soles. You also get if you scratch or rub your skin and even from this power, where this is magnified 20 times normal, so 20 times a normal eye view, and you can see those open spaces are blood vessels. Here, up here, you have your epidermis. You have your papillary dermis, the little pink stuff in between. This is the reticular dermis down here. And even from here you can see the difference in the collagen: the fine collagen of the papillary
dermis, and in the thick, chunky collagen, and the thick bundles of collagen in the reticular dermis. And you can see down here that they're at the bottom, we’re starting to get into fatty layer, the subcutis. Right. And then here between the dermis and the subcutis, we have all these little round structures those are all the eccrine glands that we talked about before that live at that level of the dermal subcutaneous junction. So even from very low power, you can begin to see all the structures once you know what you're looking for. So let's go in
a little closer because they're a couple unique structures in acral skin that are worth knowing about. I really like acral skin. It's very pretty under the microscope and it has a lot of cool little things to see. So let's look. Number one, if we can find the structures up here that I really like and of course, they probably won't be here now that I'm looking for them. That's disappointing. Well, we'll have to go down here instead said this structure right here look, it looks a blood vessel. It's got kind of a little muscular pink wall.
And in the middle, it's got a space that's called the lumen, and that lumen is lined by a single layer of little kind of flattened cells, those are endothelial cells. And there's little couple red blood cells in the middle. But look, this is kind of different from other blood vessels because look at the small round cells, very nicely and neatly organized around the outside of this vessel. So this is called a glomus apparatus, or glomus body. And these mostly exist at the tips of the fingers, near the nail beds, and they're arteriovenous anastomosis. And the
theory is that they play some role in temperature regulation and those little cells around called, they're kind of modified to muscle cells, pericytes, we talked about earlier, they're just very prominent here and they kind of have contractile properties that allow this vessel to kind of open and close, and allow for blood through. So that's a glomus apparatus. And then look over hear, there's another little tubular shape, but this is not vessel. It's got too layers of cuboidal cells, so this is actually an eccrine duct. Alright, so you can begin to tell these things apart once
you look at them. A lot. And the other thing we'll look at here, we have this structure which is a pink bundle, and remember we talked about pink bundles can be nerve, smooth muscle, or dense regular connective tissue like you'd see in the tendon or fascia. And this in this case, it's nerve. And in nerves it’s kind of a little bit wavy, it kind of undulates back and forth. And when you look closer, you can see right there, this little line in the middle, that's actually an axon, and those little bubbles around that are where
the myelin normally resides. Let’s see if we can get that in the better focus. So I only see it just very focally. So that little pink line there is the axon. And then there's little bubble, and in that little space is either this probably the node of Ranvier or there's also this thing called an incisure (of Schmidt-Lanterman), I can't repeat the name of the person, but someone named it so it must be important. So anyway, that little space of white is where myelin was that's now washed out. So only in like kind of larger, deeper
nerves, do you really see much myelin. Up near the surface of the skin, we don't usually see myelinated nerves, we only see unmyelinated most of the time microscopically. Alright, and then let's look at the adipocytes while we have them here. So this is what that the fat looks like in the subcutis. The fat cells are large and white large white circles and they have nuclei, you just don't get to see them all the time because it depends what cut you’re at. Each of these big huge fat cells only has one nucleus. So the nuclei are
these little dark guys at the very edge of the fat call, and they're actually kind of disk shaped, but they look like little spindle stretched out cells because they're squished out by all this fat. And so it's kind of hard to see what their nuclei look like in a normal fat. But when you get them cut at an angle, you can kind of see their nuclear features, where they have a little bubble of little fat droplets in their nucleus. And we'll see if we can find that here. I don't… Oh there this. So here this
little adipocyte nucleus is kind of folded over, so we can see it, we can see it cuts across. And that little hole in the center is called a “lockhern”, that means “nuclear lake”, it's a little lake of lipid/fat in the middle of the nucleus. And it's always there in adipocytes nuclei, you just can't usually see it. So when the fat is kind of atrophic or damaged, you can kind of see it. We cut through the adipocyte nucleus at an angle and then you can see this little bubble. It's always there, but people sometimes get confused
about that because they're not used to seeing it. And there's another little tiny glomus apparatus. See the little vessel in the middle, and the little clump of cells around it. Alright. Now let's look at the different part of the body. Oops, we'll turn it over. Now this is beautiful. This is the scalp. And here we are even at the lowest possible power on my scope, try to get the focus there, you can't even see all of it in one field and that's because these giant hairs that go all the way down. So these are called
anagen hairs, they’re the normal hair that make up most the hairs on your scalp. And you can see that these blue kind of nodules that here they almost look like little flames in the end of a candle, if you have a good imagination. Those little purple things, those are the roots of the hair. That's what's giving rise to the hair. It's growing the hair from that place there. And those in the scalp and near the scalp, the hair roots are situated down here in the subcutaneous fat. So most other places on the body, your hair
follicles kind of arise in the dermis, but here on the scalp, particularly you have lots of these really large anagen hairs. And they have their roots down in the subcutaneous fat. And you can see we can't, you know, unless we get really lucky with the way we slice the tissue, usually don't get to see the whole hair all the way up. So you have to see it kind of has multiple sections that hair connects to the surface. We just can't see it because it's not on the plane there were sectioned through tissue. So and then
up here, you can see where the hair shafts come out or where the follicles open to the surface and the hair shaft would come out through there. You can see these white sebaceous glands. Right. And those make the sebaceous secretion we talked about that earlier. So let's look a little closer. I think that hair follicle anatomy is one of the more confusing aspects of histology, I think there’s a lot of different structures in there. So here, we’ll go down the higher power. And I'm sorry for the line across the screen, that's a scratch on the
surface of the slide. And it's at the diagonal line, it's not real it's just on the surface of the glass. So here we are. This is hair root or the hair bulb, and it's made up that these dark blue cells. This is called the germinative epithelium. These cells are actively dividing, you can see mitosis right there. And their job is to grow quickly and that's why our hair grows because of these cells way down here at the very root. And then this little pink, this little pink papilla invagination into the bulb of the hair roots,
or the hair bulb, this is called the hair papilla. And it's made a kind of specialized mesenchymal spindle cells, like modified fibroblasts. There's little blood vessels in there and that's what gives the support and nourishment to the developing a hair bulb. Okay and as you go up, you can see that these germinative or also we call the blue cells matrical cells, these matrical cells are germinitive cells. So they begin to change and they begin to look less blue or purple and a little bit more pink, and that's because they're developing more keratin in their cytoplasm.
And what's going to happen is that these cells will eventually die, the nuclei will go away, and what you'll be left with is this compact like kind of cable made out of dead keratin compacted together, and that's what the hair shaft is made of. It's made all these cells that are dead and compact together. But we can also see that around the outside of these matrical cells that are developing in the hair, we have this bright red beautiful layer here. And this is called the inner root sheath, and it's got a couple layers generally I
don’t think are really important to know that that eventually will develop a cuticle, a Henle layer, and Huxley layer. I don't think that those are really that important for most medical students to know at least and honestly probably not that important for most pathologists to know. And then here on the outside, you can see this outer layer looks very very different. It's very clear. It kind of has these very columnar, like tall cells that almost look, some people imagine they look like piano keys, and sometimes when we have a better cut they do. So that's
called outer root sheath, and it's clear because the cells are filled with glycogen and that glycogen washes away during tissue processing and leaves these clear spaces. And then as we travel up, these layers continue to change and look different. So here, this is a different hair follicle, but a little bit further up, and you can see this is very different now. And we’re cutting kind of an angle, that's why it looks like a little oval rather than a tube. This is the outer root sheath, and you could see those nice piano keys along the basal
layer. You can see this clear cytoplasm. The inner root sheath now doesn't have those bright red granules, those are called, and that we looked at, those are called trichohyaline granules by the way. Those bright red granules, those are trichohyaline granules. Oh and look, this is nice. This is a different hair shaft, but you can see that the cells, those blue matrical cells we talked about earlier, they've now like gotten to be very pink, and they have docked their nuclei. They are on their way toward towards dying, and so this central structure here is eventually going
to become the whole hair shaft. So again that's outer root sheath. These three layers here are the inner root sheath. And then this is the developing hair shaft. And so as we go further up, now you can see it's kind of fragmented but let's look closer. The inner root sheath is now just a single pink dense layer. The hair shaft is kind of broken here but that it has no nuclei retained anymore. That's the hair shaft in the middle. This is the inner root sheath right here. This is the outer sheath that's like glycogenated and
has those little piano keys. And then there's this little pink layer on the outside that we call the adventitia, it’s kind of modified fibroblasts that are surrounding the hair shafts. Let's go up a little further on the hair. So here's a nice long cut. The hairs actually missing, it's fallen out of the center during processing. Hair is a little bit fragile, so sometimes it does that. But as you go up, you can see that the outer root sheath doesn't look quite so clear anymore. Now it's looking much more like the kind of epidermis does. It's
kind of pink and has a basal layer, and then a more pink layer on the inside. It doesn't have that really prominent clearing anymore. Now the hair follicle keeps going up and eventually, even though see the white space here, this is kind of a chunk of tissue that was missing from when we cut that the tissue, but you can see that what happens is the sebaceous gland drains into the hair follicle. And so that's called the sebaceous duct. This little area here, where the sebaceous gland drains directly into the follicle. And the follicle opens up
on the surface. And on the surface you can see that this portion of the follicle is called the infundibulum, the portion where that the sebaceous duct drains in, that's called the isthmus, and in this portion appears the infundibulum. And the infundibular portion of the hair follicle looks just like the epidermis. And we talk a lot in pathology about epidermal inclusion cysts or epidermoid cysts. The surgeons call them sebaceous cyst even though they're not actually sebaceous. What they're lined with is this lining right here. So they’re really actually follicular cysts of the infundibulum. They're growing from
infundibular portion of the hair follicle, and they have a lining just like this, and that flaky loose keratin in the middle. So this basically at the very opening of the hair follicle looks just like the surface of the epidermis. And you can see this little detached fragment here, this is a hair shaft. It's kind of refractile, you can kind of, it kind of floats above the rest of the tissue. It's hard to see because it's fragmented. And it's got little bits of brown and that's melanin. And that's where hair has color because we have melanocytes
down in that root of the hair follicle. They give the hair its pigments. Let's see if we get another, a better look at a hair shaft. They're hard to find sometimes. The little one there, but maybe there's a bigger one somewhere. That's pretty good. See here's a hair shafts, so the follicle is that that outside epithelial layer here that kind of a surrounds the hair shaft. And the shaft is the hair itself that comes out atop your head. And again you can see these little streaks of pigment there, that's melanin. That's what would make your
hair brown or different colors. And then the rest of the pink of the hair shaft is keratin. It's from those dead matrical cells down the root that gave rise to this. And that's when you get a haircut, that's the stuff that's out on the surface that gets cut. Here's another picture of hair root cut a little bit differently. There’s the hair bulb, and look at the brown pigment in there, those are actually melanocytes. Try to get it in focus here. There's little brown pigmented cells, those are melanocytes and they have these are branching dendritic processes,
these little tiny branches and they're feeding melanin to all of the matrical cells. And that's why when the matrical cells go up towards the top and die and turned the hair shaft, the hair shaft has pigment included. And again that's why we have pigmented hair of different colors. So that's how hair works. It’s a little bit complicated, and I still think it's like one of the last great histologic mysteries for me. And I still hair pretty challenging. I think we have one other view, maybe of a hair follicle here. Let's take a look and see.
That's about the same as what we were showing before. You can see the bulb down there at the bottom, it may have matrical cells. You can see the developing inner root sheath of those bright red granules. And then moving up, you can see the outer sheath that's made of pale, glycogenated cells. And in the middle here, you can see the matrical cells are now turning more pink and elongated. And so that's actually that's called the cortex of the developing hair shaft and then that's the medulla. So that the bulb is turning into a cortex, an
outer layer and a medulla middle layer, and then eventually that will all squish together and die and turn into air shaft. And again we have nice adipose tissue out here. Oh and that's pretty good too. Here's a little bit thicker blood vessel. And you see the blood vessels have that inner layer of endothelial cells that are flat, and then on the outside as you get in the larger more muscular vessels, you actually have two layers of smooth muscle. You have kind of an inner layer and then an outer layer. And the outer layer is kind
of wrapping around in a circle, we're cutting across that's why the cells instead of being spindly they look like little tiny round dots, because we're cutting them in cross section. And if you get in here, just a little bit, you can see that if we cut it a little bit different angle, that they actually spindle cells, they are elongated. And this cell and this cell, those of the same cell, we're just cutting them 90 degrees to one another. So when you cut long thin spindled cells in half, kind of like if you imagined a hot
dog, you got a long ways versus a cross section half, it looks totally different. You have to think of cells in 3 dimensions just like that. And then right here we got a nerve. And there's those little pink dots are axons. The little purple dots are Schwann cell nuclei. And then on the outside this layer is called the perineurem. It wraps and supports the nerve. This is a section of adipose tissue, fatty tissue from near the hand of the wrist. And the reason I'm showing you this there's no actual epidermis on this piece but you
can see where near the dermal subcutaneous junction because look, in the fat we have these. Eccrine coils, eccrine glands. So you know we’re near the skin once you see those you know that the skin has got to be… Sorry. Skin has got to be nearby. There they are, the eccrine sweat glands. And then these structures over here are one of my favorite structures. One of my favorite normal structures in the human body. There they are. The onion skin beauty of the Pacinian corpuscle and so these structures are basically attached to a nerve. And they’re made
of multiple swirled layers around the outside, and their deep down in the tissue. And their job is to receive deep touch or pressure. So that's why they're not near the surface, they’re down deep. I kind of think of them as having all these multiple rings so that they can be kind of spongy and they can squish down when someone pushes on your hand. And so you tend to have these most prominently near the acral surfaces, and they're down usually in the fat or the deep dermis. So I think they're just really pretty to look at
and I never get tired of seeing them, no matter how many times I've seen them. See, here's another one. A big huge kind of one, cut at kind of different angle. Looks like an onion, right? More than anything else, that's called onion skin, this looks like an onion. Pacinian corpuscles. Plus they have a cool name, so I really like the Pacinian corpuscles. All right. Here, let’s take a minute to look at a big nerve. And this is not actually from skin, this if from deep soft tissue, but just demonstrate what nerves look like. This is
a large nerve made of multiple nerve bundles. You can see each of these pink bundles is a nerve bundle all packed together. And they're made of these spindle cells that are running at together in parallel. And again those are Schwann cells. They're kind of protecting and wrapping around each individual nerve fiber. Nerves tend to get a little bit undulating and wavy, but be aware that that they're not the only thing that's wavy. Actually tendon and other fibrous tissue tends to be wavy as well. But that's a large, kind of thick nerve. We don't usually see
nerves like this in normal skin. This is from deeper and soft tissue. Alright. Think we already looked at this tissue actually. And then I think one last a structure to show. We didn't really cover this is fat, subcutaneous fat. And here in the fat is a very large tumor. This is sarcoma actually. We're not gonna talk about that in this video, but the reason I'm showing this is that down at the very bottom of the fat where the fat of the subcutis runs into the muscle underneath, you have this thick layer of pink stuff this
is dense regular connective tissue, dense collagen and this is called the fascia. Tendon, fascia, ligament all look more or less identical microscopically just depends on where exactly it's from. But what it's made of is really thick and dense compact bundles of collagen and those dark stripes there, that's artifact, that’s folding from when we cut the tissue. Sometimes the tissue cuts don't fold, don't lay out perfectly flat, and we get little folds in it so. I'm sorry, we try to avoid that but it's impossible sometimes on big specimens. And here if you look at higher power,
this is what dense, regular connective tissue looks like. If you cut cross sectionally, the fibroblasts look like they're little tiny round nuclei. But if you cut it like here, in longitudinal section, you can see that the fibroblasts actually stretch out and are kind of elongated. And there's dense pink stuff in between, and that's the collagen, collagen type one. So a lot of people confuse this with smooth muscle but I think that a key is that if you recognize, it's a little hard to get on video, but if you recognize that the pink bundles are actually
bundles of collagen outside of the cell. And under a microscope, you can kind of see they were refractile a little bit, they kind of move in and out of the tissue. If you kind of move your condenser up and down. Maybe we can try that and see if it works. Not really. Oh there. I guess there you can kind of see that they kind of move in and out of focus. And at these cracks in between them, so those are collagen in bundles and collagen is an extracellular matrix protein. So it's outside of the cell.
So these are fibroblast, they're making all this pink collagens and pushing them outside of the cell, as opposed to smooth muscle which looks pink because it's filled with contractile proteins. So those are intracytoplasmic proteins. Takes a little practice, but eventually you can kind of learn to tell them apart. But I think that's important. I find that even that at the resident, and sometimes higher levels, people still sometimes struggle with telling apart tendon or fascia from muscle. So if you struggle with that as a medical student, don't feel bad you're not alone. Alright. Now let's look
at a couple of immunostains before we finish up. And immune stains again are antibodies that are targeted at certain proteins. And they are then tagged with a colored molecule. And that lets us see what kind of proteins we are actually dealing with here. So let's start with cytokeratin. So we said cytokeratin is an intermediate filament. Oops, we will turn it around. It's intermediate filament that fills up epithelial cells of all sorts. All epithelial cells in the whole human body should have cytokeratin, and they sometimes have different types of keratin. But this is a marker, this
one right here, is a pancytokeratin. Those six stains multiple different types of keratin, so it will stain pretty much every type of keratin ideally that's out there. So if we see that positive, we know that what we're dealing with is an epithelial cell. So here, let’s get it in focus. So there's the normal epidermis, and you can see the epidermis is bright, this dark brown color because it's filled with keratin filaments. Where's the dermis, which is made of collagen, is totally negative for keratin. So keratin highlights the normal epidermis. And then when we looked down
at the structures in the epidermis, you can also see… I’m sorry, the structures down in the dermis, you can see that these things we talked about earlier. The hair follicle so made of epithelium, so it's keratin positive. The sweat glands also made of epithelium, so their keratin positive. So all these cells that are brown are some sort of epithelial cells. So here we have sweat glands, hair follicle, and then we already talked about that the surface in this skin, the epidermal surface is made of keratin as well. And so we can use, the reason we
use these immunostains is to help us when we have tumors if we're not sure what type of cell tumors coming from, we can use the immunostains to help us determine if the cell is epithelial or its muscle or nerve or melanocyte origin. And that makes a big difference because those tumors all have different properties that we pay attention to. So the next thing we’re look at is S-100 protein. And the reason I'm showing S-100 protein is that it does, it stains nerve and some other things. It stains melanocytes in the epidermis. So it will stain
melanocytes along the basal layer, so these little guys down at the bottom here. Let’s find them. These little cell sitting on the bottom basal layer that are dark brown, those are melanocytes. You can see they have these little branches, those that we call them dendrites. Those are the branches that feed melanin to the neighboring keratinocytes. So melanocytes are S-100 positive. Alright, but they're not the only cell in the epidermis that’s S-100 positive. You can see another branching little cell up here in the mid-layer of epidermis, those are Langerhans cell. The only reason I can tell
them apart is because of where they're located in this skin, which is actually a piece of normal epidermis. So you have S-100 positive melanocytes down at the basal layer, and then also Langerhans cells, which again, are antigen processing cells up there in the mid portion of the epidermis. And then also fat, adipocytes tend to stain with S-100 as well. So you can see S-100 staining these fat cells here in the subcutis. S-100 is not a very useful stain for fatty tumors, but it does stain normal fat. And it will stain nerves as well, but I
didn't have a good nerve to show in that piece. And then here is a stain for a muscle marker called desmin. Desmin is a muscle protein. And you can see actually that the epidermis is dead negative, right, completely negative for this marker. But down in the dermis, you can see these bundles that are dark brown, those of the smooth muscle bundles, the arrector pili muscles that we talked about earlier in the video. Those are the muscles that give you kind of goosebumps, right, and they hook up the hair follicles. And then also look at these
round little donut shaped rings around here. Those are blood vessels. Alright, so as opposed to desmin around vessels highlighting the wall, let's look at this immunostain. This is an immunostain called CD 31. And so you can see it's actually staining the central lining of the vessel, the lining of the lumen, which the endothelial cells, but the muscle wall on the outside is actually completely negative. So again, you can tell that the inner lining and the wall of the vessel are actually made of different components. You can see all these little vessels around here, the smaller
capillaries, they all have the lining cells, the endothelial cells, are staining with CD 31. And CD 34 is another marker that does the same thing. It stains the lining cells of the vessels and it will stain both lymphatics and arteries and veins. Endothelium of any kind will stain with this marker. So again, one more look. There that's the lumen being lined by endothelial cells which a positive on a CD 31 immunostain. Alright, and one other immunostain to show is a stain called Sox10, and it's a nuclear marker. It's a protein that's in the nucleus of
melanocytes. And you can see this is, I’m just showing this to highlight that melanocytes normally are present on the basal layer of the epidermis, and they're kind of spaced out. And this is a patient with a lot of sun damage, and so the number of melanocytes kinds of increases a little bit in sun damaged skin. But they're down there on the basal later for the most part. They're spread out with that kind of melanocyte for every 7 to 10 keratinocytes, depending on who you ask and where exactly you are on the body. And look a
little closer. You see this is highlighting the nucleus of a cell. So we should the S-100 earlier they showed both the cytoplasm and the nucleus. Sox10 mostly highlights just the nucleus. So it just helps you see very nicely how many cells are there. It will also stain other things too, like it stains Schwann cells and nerves. So it's not a perfectly specific marker but it stains both benign and malignant melanocytes, and it will also stain most nerves. I’m not sure if we have a nerve down here but we can look and see. If there's any
nerve in the dermis. I'm not seeing one. So anyway, that’s a Sox10 immunostain and that's just to highlight kind of the normal pattern of how melanocytes are situated in the basal layer of the epidermis. Alright. And now let's go. There’s a couple things I realize that I skipped over and did not show you. And I wanted to demonstrate those. So one is a structure that I was looking for in acral skin. And this is not the most perfect example, but it will have to work. For now. Right here beneath the epidermis, so in the papillary
dermis, is this round, or kind of oval shaped pink structure. And it has a kind of little layers, little lines that run across and little spindle cells inside when sometimes these are like perfectly oval, and they somehow remind me of a striped pink Easter egg. I'm probably the only person the world that's reminds me of but it that's what I think of when I see them. But these are called Meissner corpuscles. And Meissner corpuscles or Meissner bodies live right here in the superficial dermis, right the papillary dermis, so they're right next to the epidermis. And
the reason is that unlike the Pacinian corpuscles, that big onion skin looking guys that are down deep, their job is to detect that kind of firm pressure or deep pressure or touch or vibration sensation, Meissner bodies, these little guys up here, are right next to the epidermis because their job is to detect fine touch. Basically, so they need to be right under the epidermis so that they can detect the most minute of movements and they're mostly located on acral skin, particularly near the fingers. And that's why we're able to have the most discreet fine touch
with our fingers because of all these little Meissner corpuscles. You don't see them much elsewhere except on acral skin. Even on acral skin, they usually really have a predilection towards the tips of the fingers, on the finger pads, where you have the most fine touch ability. So that's a Meissner corpuscle. We’ll look a little closer. And for a normal structure. And then a nerve kind of hooks up to this thing. You can't always see the nerve in there, but basically this is made a kind of a layered bundle of nerve like material and structures that
then connect up to a nerve and go back to the nervous system and give fine touch information to the brain eventually. So that's a Meissner corpuscle. And I also wanted to show a couple of interesting slide that we don't get to see very often. Now this unfortunately, this slide is too big to even entirely fit on one view, but this is acral skin. You can see that thick corneal layer. And there's dermis, subcutis, and this is bone. And that's the bone marrow space which is filled with fat and a little tiny bit of bone marrow.
And this is actually an amputation specimen from a, I can’t remember, I think this is from a toe. And the reason is because of this massive tumor here, this is a melanoma growing underneath the toenail. So this is a big huge melanoma, that's not really the point of the video, but the point is just to show that this is what a toe looks like. You've got the acral skin, and underneath it that you've got the dermis. You got sweat glands down here. There are large dilated blood vessels. I think underneath here we can see some
very nice glomus structures. Glomus apparatus. So you see this kind of tangled coil of vessels here, each of those central spaces is a lumen lined by endothelial cells. You even see some blood cells in there. And in those little perfectly round guys kind of organized around the outside, those as modified muscle cells, the pericytes, that help kind of constrict these little vascular channels. So that's a glomus apparatus or a canal of Sucquet and Hoyer if you want to be fancy and impress your friends, you can tell them that. And then down here is bone, this
is a cortical bone, lamellar bone, you can see that the lines laid down here in organized fashion. And in these central spaces, those are called lacunar spaces, and in there you have osteocytes that have become entrapped. As they started as osteoblasts and then as they built the bone around themselves, they made a little tiny space where the osteocytes are entrapped inside and so that's cortical bone. So this is the bone of the phalanx of the great toe. And let's go around to the other side here. The other thing that's kind of interesting here is that
you can see, coming right off of the bone, is dense pink layer. This is dense regular connective tissue, and again I told you earlier, that dense regular connective tissue is either fascia, tendon, or ligament. And here you can see that it's actually connecting this big band of it right here is connecting broadly to the bone. So if that on the other side, which we can't see here, if it hooks up to a muscle then this would be a tendon. If on the other side it hooks up to a bone, it would be a ligament. So
ligament and tendon and fascia look very similar at high power. And really it's kind of the context that you find them in that you can tell them apart. So that's a nice example of probably a tendon in this case. It's hooking up to one of the muscles that allow you to contract or extend your fingers, to flex or extend fingers. Oh and another nice structure that we have here, this is an artery and how we can tell it’s an artery is that we got this nice thick smooth muscle wall around the outside and then look
what's happening here right outside the lumen, there's the lumen. The lumen is lined by a layer of thin flat endothelial cells, and then out here, let's see if we can get it to show up. We’re going to flip the condenser. See that squiggly line there that comes in and out of focus? That's called the internal elastic lamina and it's this little band of squiggly elastic tissue that's right underneath the intima. And the intima is this inner layer and then the media is this outer layer that's made of muscle. And there's also a little tiny layer
outside called the adventitia. But when you see a presence of the internal elastic lamina, that means it's an artery actually rather than a vein. So veins can have thick muscular walls just like arteries can, but finding that elastic lamina that's a pretty good sign that you're dealing with an artery. So there's a nice example of a big artery. We don't see those in most skin biopsies, but when you have larger specimens like this, you can see them sometimes. So we've got artery, we've got some probably tendon, then we got nice bone down here, and then
we've also got a big melanoma arising under the nail. And I think somewhere I also saw... Over here. Oh yeah. It's kind of fragmented, but you can see part of that onion skin. So there it is again, the Pacinian corpuscle. It’s kind of broken in this case artifactually during processing, but that's a Pacinian corpuscle. Alright I think I've got another amputated toe here for a melanoma. So fortunately, these are rare melanomas on the toe, but they do happen. And actually famous musician Bob Marley died from a subungual melanoma of the great toe, unfortunately. So this
is when dark skinned patients get melanoma, this is the kind of melanoma they tend to get. You don't usually get melanoma if you're black or brown skinned, but if you do get melanoma, it's usually going to be under the toenail/fingernail or on the palms or soles. So the reason I'm showing this one is here, this is the top of the toe, and when we come out, this is what we call the nail fold going over the top of the nail. And this dense pink structure right here, this is nail, the nail plate. The nail plate
is the part of your nail that you clip when you clip your nails. And where the nail plate grows from deep down here underneath that little area at the top of your nail when you look down at it this is called the nail matrix. So these are the dividing cells. They look more or less like keratinocytes, they're basically modify keratinocytes. And these cells are growing and giving rise to the nail plate. The nail plate just like your hair is made of dead keratin. It's just a bunch of keratin stuck together. And you can see that
the keratin develops into this nice plate and that plate comes out and exits from underneath the fold and then goes along the top surface of the toe. And again here, it's unfortunately underlined by this huge massive melanoma, all of this purple stuff down here. This whole huge thing unfortunately is melanoma, which is very bad. But this is that’s a nice example, though aside from the melanoma, is an example of the matrix and the nail plate. And the little layer of epithelium underneath the nail plate, we call that the nail bed epithelium. And again, it's not
very normal here. It's kind of destroyed by the melanoma underneath it, but it is a good idea to get from low power to see that this is what your nail fold up there, the nail plate, the matrix of the nail. And then out here is the tip of the toe, lined by acral skin. It's kind of torn up from processing. Unfortunately to get the cuts of these sections with bone in them, we have to soak them in a type of acid to dissolve the calcium. And that kind of damages the quality of the histology, and
makes the tissue not look quite as good, but that otherwise we’re not able to cut through the bone. So and again you got your nice acral skin here. And what other structure to show while we’re on acral skin. Let’s see if we can find a good. A good one here. Ah, there it is. So right here, on acral skin, when the eccrine sweat duct, that’s the eccrine sweat duct, see the double cuboidal layer with the little lumen lined by pink cuticle, it eventually comes up and empties into the surface. And when it does, you can
see it kind of spirals, you get this, this is all one duct that's kind of spiraling, we're just cutting through part of the spiral. It spirals up and out through the surface and that still the space there, they're even going through the corneal layer that allows the sweat to come out to the surface. So when you get sweaty feet or sweaty palms, this is how it's happening. And so this structures called the acrosyringium. The acrosyringium is this little twirly outflow tract of eccrine sweat ducts that you see most prominently on acral skin. The eccrine ducts
exit out the surface, also in the skin too, but you really notice the slight kind of swirled, a spiral like pattern in the palms and the soles. There's another one, so you can see the eccrine duct. You can see it's kind of cut. There's another section of it, there comes up to the top. So again, this all connects together, we’re only just seeing one plane of section. So these are 3 dimensional structures we’re just cutting one slice through. So that's a nice example of an acrosyringium. And I think that about covers everything except for one
other abnormal thing, but it's so common that it's worth bringing up because we see it all the time. So I showed you before... Sorry. This guy showed you before, we said that there's epidermis and then there's the dermis which is composed of pink collagen bundles, but looking at this you can tell, even from here you can tell, this is not pink. This is actually blue or gray. This is made of tangled little wavy fibers that are made, that are blue or gray in color. And you can see a little tiny bit of pink collagen that
is left over in here. Let's move over a little bit. You can see there's more collagen over there, that's what the dermis should look like, right. But here, most of the dermis is being replaced by all of this pink. Sorry, all of this bluish gray stuff. And those are elastic fibers, and so this is called solar elastosis. And when you spend years and years out in the sun, getting sun damaged, this is what happens. This is not from one sunburn, this is from decades and decades of chronic daily sun exposure. And you can see that
when people that are older and had a lot of sun exposure, what happens is, it basically pushes down and replaces the whole dermis. And so now the whole dermis is now composed of a thick layer of elastic fiber. So we call this solar elastosis, and when you see that, it's a good sign that you're dealing with someone who's had a lot of sun exposure. And so you know you can keep an eye open for things that tend to occur in the setting of sun exposure, like in this case. This is actually an invasive squamous cell
carcinoma. All this pink stuff growing down here, this is squamous cell carcinoma. A type of skin cancer that occurs secondary to long term sun exposure. Alright, so that’s solar elastosis and in the part of the country where I practice, we see this so commonly, most cases actually probably end up having this when people are of a certain age because people just are out in the sun a lot, there's a lot of high intensity sunlight here. So it's so common that even though it's not normal, it's worth bringing up. And this is actually what causes wrinkles.
So when you get, when you see people that are very wrinkly skin from long term sun exposure, this is why. It’s the elastosis makes the skin kind of move into different shapes and doesn't let it go back to its normal shape over time. So not only does sun damage cause certain types of cancer, but also causes the skin to wrinkle and age more rapidly. So I think that wraps up normal skin histology and even a few abnormal things as well.
Related Videos

37:41
Basal Cell Carcinoma (BCC) 101 - Dermpath ...
Jerad Gardner, MD
113,785 views

17:34
Integumentary System | Skin Model Anatomy
Ninja Nerd
381,486 views

1:15:56
Melanocytic Dermpath Basics: Melanoma
Jerad Gardner, MD
87,867 views

59:39
DERMATOPATHOLOGY: Blistering Diseases
Maxwell Fung, MD
3,887 views

1:32:38
Squamous Cell Carcinoma & Actinic Keratosi...
Jerad Gardner, MD
110,297 views

21:01
Watch Trudeau speak directly to Trump duri...
CNN
12,614,546 views

27:12
Authorities reveal cause of death for acto...
ABC 33/40
1,443,106 views

7:46
Elon Musk Cold Open - SNL
Saturday Night Live
14,950,658 views

14:33
The Integumentary System
Professor Dave Explains
708,337 views

7:04
Bolton has theory on why Trump threatened ...
CNN
1,379,140 views

57:56
Inflammatory Dermpath 101 (A Beginner's Gu...
Jerad Gardner, MD
42,991 views
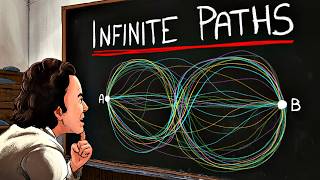
33:37
Something Strange Happens When You Trust Q...
Veritasium
4,805,377 views

7:31
This Was DESTROYING My Life
Dr. Eric Berg DC
242,280 views

26:21
Exactly Where I Get Injections and Why | B...
Dr. Sam Ellis
449,141 views

5:42
Musk demoted! Go inside Trump's EXPLOSIVE,...
MSNBC
1,976,703 views

31:12
Singapore's Top Diplomat Reveals TRUTH Abo...
Cyrus Janssen
121,993 views

59:59
Basic Dermpath Cases - Explained by a Der...
Jerad Gardner, MD
106,078 views
9:47
Integumentary System
Amoeba Sisters
788,096 views

13:33
Republicans begin to turn on Trump over Uk...
Times Radio
336,604 views

28:12
From Extreme Fatigue To STAGE 4 CANCER! - ...
The Patient Story
2,636,667 views