Approach to Upper Gastrointestinal Bleeding - causes, symptoms (melena) and treatment
136.79k views1427 WordsCopy TextShare

Armando Hasudungan
Patients with acute upper gastrointestinal (GI) bleeding commonly present with hematemesis (vomiting...
Video Transcript:
patients with acute upper gastrointestinal bleeding commonly presents with hematemesis which is vomiting of blood or coffee ground like material and or molina which is a black atari stool the initial evaluation of patients with an acute upper gastrointestinal bleed involves an assessment of hemodynamic stability and resuscitation if necessary diagnostic studies usually endoscopy and when possible treatment of the specific cause upper gastrointestinal bleeds or upper gi bleed can be differentiated from lower gastrointestinal bleeding based on clinical presentation we have molina and hematemesis for an upper gi bleed and hematokesia which is fresh blood in feces for a
lower gi bleed both may present with signs of anemia and blood loss depending on the amount upper gi bleeding can be differentiated from lower gi bleeding also based on anatomy upper gi bleeding occurs above the ligament of treats whereas lower gi occurs below the ligament of tree the ligament of traits is a muscular band that suspends the fourth part of the duodenum from the right crews of the diaphragm now we will talk about the causes of upper gi bleeding firstly the most common and this is in descending order and then we'll talk about the rare
causes so probably the most common cause is gastric and or duodenal ulcers essentially ulcers form when there's more gastric acid secretion than there is mucosal defense the risk factors common risk factors include helicobacter pylori infection which is a spiral bacterium that infects the superficial gastric mucosa and disrupts the mucosal layer non-steroidal anti-inflammatory drugs are also common cause physiological stress excess gastric acid and rarely you get hyper acidity alone and this can be due to a syndrome for example in patients with zollinger zollinger-ellison syndrome severe or erosive gastritis or duodenitis is another cause the term gastritis
and duodenitis are used to denote inflammation-associated mucosal injury the risk factors are also the same for peptic ulcer disease as mentioned earlier severe or erosive esophagitis as the name suggests is severe inflammation of the esophagus it's associated with gastroesophageal reflux disease gourd or gerd on endoscopy what you see is erosive damage to the esophageal mucosa other risk factors include medication use including non-steroidal anti-inflammatory drugs oral bisphosphonates tetracyclines and infections including candida and herpes simplex virus canada represents itself as white streaks in the esophagus usually associated with some immunodeficiency a very important cause of upper gi
bleeding is gastroesophageal varices and these usually develop as a consequence of portal hypertension in approximately 50 percent of patients with cirrhosis and varicel hemorrhage occurs at an annual rate of about 10 percent varices may be identified in the esophagus and or the stomach they may also be seen at sites other than the esophagus of the stomach such as the small bowel these are known as ectopic pharisees as with most other causes of upper gastrointestinal bleeding endoscopy is a diagnostic modality of choice for esophageal gastric viruses and here you can see dilated veins the management of
esophageal varices include band ligation which is a standard treatment you can also have sclerotherapy when band ligation is not technically feasible also there is early trans-jugular intra-hepatic port of systemic shunts or tips for short gastric viruses is usually managed with some sort of injection in the form of cyanoacrylate which is glue portal hypertensive gastropathy also known as congestive gastropathy is caused by portal hypertension the pathogenesis of portal hypertensive gastropathy may be related to both congestion and hyperemia in the stomach angiodysplasia also known as vascular ectasia is essentially ectatic dilated thinned walled vessels is essentially ectatic
dilated thinned walled vessels which can be seen as spider nevi in the stomach the vessels here are thin walled and are usually lined by endothelium alone not the muscle and so as a consequence it can easily rupture dulafoy's lesion is a dilated aberrant submucosal vessel that erodes the overlying epithelium in the absence of a primary ulcer the etiology of doula foy's lesion is unknown additionally events triggering bleeding are not well understood patients who bleed from doula forest lesions are typically men with comorbidities including cardiovascular disease hypertension chronic kidney disease diabetes and alcohol abuse malory white
syndrome is characterized by longitudinal mucosal lacerations intramural dissections they're called in the distal esophagus and the proximal stomach and these are usually associated with forceful wretching the lacerations often lead to bleeding from submucosal arteries these tears usually heal spontaneously very important cause of upper gastrointestinal bleeding although less common are mass lesions including polyps and cancers neoplasms of the upper gastrointestinal tract account for less than three percent of all cases with severe upper gastrointestinal bleeding the bleeding here is usually slow in a majority of cases actually no lesions are identified and so when patients present with
upper gr bleeding and get an endoscopy there's actually no lesions identified even with a pill cam now we'll talk about other rarer causes of upper gastrointestinal bleeding gastric antral vascular ectasia gave also known as watermelon stomach is an uncommon cause of upper gastrointestinal bleeding the term watermelon stomach is derived from the characteristic endoscopic appearance of longitudinal rows of flat reddish stripes radiating from the pylorus in the antrum that resemble the stripes on a watermelon the red stripes represent ectatic and sacculated mucosal vessels gabe is seen in patients with liver cirrhosis and or systemic sclerosis hemobilia
or bleeding from the hepatobiliary tract is a rare cause of acute upper gastrointestinal bleeding it should be considered in any patients with acute upper gi bleed and a recent history of hepatic parenchymal or biliary tract procedures of any sort hemocycus pancreaticus or bleeding from the pancreatic duct is another rare cause of upper gi bleeding it is most often found in patients with chronic pancreatitis or pancreatic tumors aorto-enteric fistulas as the name suggests is a connection between the aorta and the small intestine it is a very rare cause of acute gi bleeds and is most often
iatrogenic usually following an aortic graft procedure and you have a leak it is associated with high mortality rates and represents a true medical emergency the third or fourth portion of the duodenum is the most common site for aorto-enteric fistulas this disorder should be considered in all patients with massive or repetitive upper gi bleeding and a history of thoracic or abdominal aortic aneurysm prosthetic graft cameron lesions are erosions or ulcers occurring in the sack of a hiatal hernia they have been described in up to five percent of patients with hiatal hernia who undergo upper endoscopy another
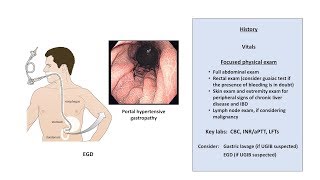
important cause to consider is iatrogenic bleeding after an endoscopic procedure for example maybe removing a polyps or having a biopsy of the upper gastrointestinal tract clinical presentation of an acute upper gi bleed include hematemesis molina signs of anemia so you have fatigue you have shortness of breath tachycardia orthostatic hypertension then you have the signs based on the actual underlying cause so upper abdominal pain for peptic ulcer disease odenophagia gastroesophageal reflux dysphagia for esophagitis or esophageal ulcers history or you know someone dry wretching or coughing indicates mallory weiss tear a history of dysphagia early satiety involuntary
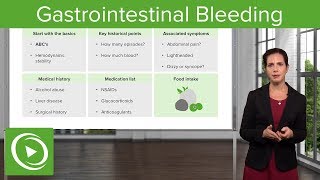
weight loss cachexia consider malignancy if you have ascites and jaundice consider varicil hemorrhage or portal hypertensive gastropathy the initial management for upper gi bleeding acute upper gi bleeding involve resuscitation insertion of two large iv cannulas performing baseline bloods including coagulation profile and group and hold and cross match administering crystalloids which will correct hemodynamics in majority also administering intravenous proton pump inhibitors and of course this can be followed by blood products and for blood transfusions there are certain indications but basically you want to transfuse everyone when there are hemoglobins less than 70. for people at higher
risk it's you transfuse less than 80. different protocols vary platelets are rarely indicated but you can consider if there are actively bleeding and their platelets are less than 50. importantly to correct coagulopathy if present with vitamin k fresh frozen plasma prothrombinex imaging the patient with a ct abdomen would be warranted but fundamentally an endoscopy should be performed within 24 hours as this reduces hospital lengths of stay and reduces blood transfusion requirements thank you for watching so in summary upper gi bleeding presents with hematemesis and molina with and without signs of anemia we learned about the
different causes the most common are ulcers of the gastric duodenum and you have other rare causes we talked about the management involves resuscitation [Music] [Music] you
Related Videos
24:49
GI Bleed | Clinical Medicine
Ninja Nerd
42,619 views
18:31
An Approach to GI Bleeding (Melena, Hemate...
Strong Medicine
181,432 views
14:43
Gastrointestinal Bleeding (GI Bleed) – Eme...
Lecturio Medical
236,248 views

12:54
Understanding Pancreatitis
Zero To Finals
534,807 views

9:31
Peptic ulcer disease - causes, symptoms, d...
Osmosis from Elsevier
1,366,925 views

13:48
Epstein Barr Virus and Infectious Mononucl...
Armando Hasudungan
280,543 views

9:00
Patients with GI Bleed – Approach to Patie...
Lecturio Medical
51,920 views

10:44
Upper GI Bleeds for Medical/PA Finals | Me...
Dr Ollie Burton
8,021 views
49:43
Stomach Disorders | Clinical Medicine
Ninja Nerd
60,437 views

16:24
Gastrointestinal Bleeding by M. Manfredi, ...
OPENPediatrics
12,347 views

48:31
GASTROINTESTINAL BLEEDING | Causes | Appro...
Medi - Lectures
34,120 views

20:09
Liver Cirrhosis
Armando Hasudungan
949,394 views

3:48
Melena, Causes, Signs and Symptoms, Diagno...
Medical Centric
132,634 views

32:25
Pancreatitis | Acute and Chronic Pancreati...
RegisteredNurseRN
1,378,320 views

22:37
Peptic Ulcer Disease Nursing, Pathophysiol...
RegisteredNurseRN
1,020,520 views

19:23
Diabetes mellitus (type 1, type 2) & diabe...
Osmosis from Elsevier
2,763,354 views

15:20
Peptic Ulcer Disease (Gastric vs. Duodenal...
JJ Medicine
311,483 views

13:11
Bowel Obstruction - Causes and Pathophysio...
Armando Hasudungan
1,116,485 views

1:06:30
Inflammatory Bowel Disease (IBD) | Clinica...
Ninja Nerd
64,962 views

6:38
Crohn's disease (Crohn disease) - causes, ...
Osmosis from Elsevier
1,023,384 views