Can You Reverse Type 2 Diabetes? | Roy Taylor | The Proof Podcast EP #287
37.57k views16215 WordsCopy TextShare
The Proof with Simon Hill
We’ve examined the complexities of type 2 diabetes many times on The Proof, learning from experts fr...
Video Transcript:
when people who have say a body mass index of 45 lose substantial weight go down to say 41 they don't have diabetes so they're still obese but they don't have diabetes but of course that's the operation of a personal fat threshold again they've just come down and so it's not a matter of totally getting rid of the Obesity that would be ideal perhaps but no we're just talking about the metabolic side of things here and so people can remain obese but manage to get rid of the diabetes even within that freame glucose is a very
useful index it just as a general indicate index of how the diabetes is progressing but when we look under the surface in type 2 diabetes it's the fat that's driving the problem with glucose so yes using glucose as a measure of what's happening is fine but it has become a sort of mesmeric uh substance that's diverted scientists away from what's really happening welcome back in today's episode I sit down with Professor Roy Taylor to say this was an honor is an understatement Roy is one of the most esteemed scientists research SE in nutrition and type
2 diabetes his work with studies such as counterbalance Counterpoint direct and most recently the retune trial have fundamentally changed our understanding of what causes type 2 diabetes and what people living with diabetes can do to improve their metabolic health and quality of life in this exchange you will learn about Roy's twin cycle hypothesis why some people who are overweight developed type two diabetes and others don't what the personal fat threshold concept is why fat accumulation in the liver and pancreas is so damaging to metabolic Health how someone can get fat out of these organs and
in doing so normalize their blood glucose and blood lipids and much more with that let's hear from Professor Roy Taylor okay Professor Roy Taylor let's straight into the deep end here and then maybe if need be along the way I can ask you to clarify a few things what is the twin cycle hypothesis the twin cycle hypothesis was my attempt to put together all the observations on how the body actually worked how the body dealt with food and metabolism and what went wrong in type 2 diabetes so over the years we'd learned firstly that muscle
was very resistant to insulin and using MRI techniques Advanced MRI techniques we could measure the glycogen in muscle and in fact use this to show that people who had normal uh insulin sensitivity at muscle stored a lot of their food as muscle glycogen within the first five hours after eating onethird really quite a lot whereas people who had low sensitivity to insulin and muscle socalled insulin resistance those people stored almost none and from other work we knew that the only way that that glucose would be handled is not being stored properly the only way way
it could be handled would be for the body to turn it into fat now that sounds like magic but that's exactly what the liver does and so that excess glucose would be shunted into fat and people will be more likely to build up fat in the liver now we shown fat in the liver causes the liver not to respond to insulin now I put all this together and the twin cital hypothesis runs like this basically a little too much food over a long period of time will cause fat to start building up in the liver
and when the liver starts getting resistant to insulin it will start putting out too much glucose because insulin usually dampens down the constant production of the liver of glucose so there we have glucose Rising a bit but what happens next is that the pan pancreas kicks in and insulin levels rise a bit to just bring things under control now that's fine temporarily but unfortunately insulin speeds up the process of turning glucose into fat and so we've got a vicious cyle that started running that will run on and glucose levels will gradually Peg up but it's
not just the glucose that the liver puts out the liver also puts out fat for the rest of the body the liver really supplies you with the energy you need to live every day overnight it's the glucose coming out from the body that keeps your brain alive and the fat coming out from your liver that keeps the rest of the body alive that's what they use to burn for energy second by second it's an astonishing process but if there's too much fat in the liver then that one liver cyal will have a KnockOn effect because
it will leave too much fat in the blood the liver puts out too much fat it will be delivered to all tissues now any excess fat would usually be stored Under the Skin and metabolically that's safe it doesn't cause any metabolic damage however in the situation of excess and with a relatively full subcutaneous Under the Skin compartment then Fat's going to build up elsewhere and that's the problem and it's when fat starts building up inside the pancreas that really the action starts so we have a second vicious cyle in the pancreas the fat stops the
insulin producing cells from working properly lo and behold that means glucose levels are higher after every meal and lo and behold that means more glucose is going to be turned into fat and so we have these twin vicious cyles interacting the importance of this twin cight assignment was that it explained type 2 diabetes as a simple chain of events yes interacting cyles but a single cause now that is simple and what we see in populations is when they're overfed diabetes erupts if they're relatively starved diabetes goes away so all of a sudden we had a
handle on this and it was a complete Revelation and a move away from what all the experts were saying up to 2011 that type 2 diabetes was a complex heterogenous disorder caused by multiple different factors well that's nonsense basically you inherit your genes but in if you put on a bit too much weight heavier than you can bear then these twin vicious cyles will start turning and being a hypothesis it could be tested and shown to be right or wrong you said there that the twin cycle hypothesis provides an explanation for a single cause what
if someone is thinking well hang on how can excessive calories explain this if not everyone who becomes overweight or obese ends up with type two diabetes that's a very good question the first point to make is that there's a wide range of thresholds at which people will develop type 2 diabetes so in our most recent study we've demonstrated that those slim people who get type 2 diabetes have have got too much fat inside their organs they simply don't show the fat so there this matter of how much fat and this personal threshold for fat but
there's a further point which is really important about 70% of people of white European ethnicity will not never get diabetes no matter how much they eat how fat they become and in fact at the moment 73% of people with uh who have a body mass IM in sorry a body mass index over 40 do not have type 2 diabetes and show no signs of getting it in the near future so we can see that it's only a proportion of people who are susceptible and that is the stop go of getting type 2 diabetes so there
are really two stages one is the eating too much the other is the uh genetic Factor but why do I say that it's just one well it's because I'm talking to a group of individuals they are one person each and in my consultations with patients I only have one person in front of me and that person comes in with a readymade collection of genes they are themselves now doctors have to practice the art of the possible so I'm dealing with individuals if a person presents to me with type 2 diabetes they have insulin producing cells
that are susceptible to fat and that is the that is the whole point so this disease is simple to understand right so it's it's not necessarily fat or being overweight or obesity that is the single explanation but it is fat getting inside these organs the liver and the pancreas specifically fat I guess where we could say it shouldn't be in individuals that are more susceptible to this so certain individuals as they're gaining weight are more genetically predisposed to having fat stored within organs whereas other individuals have a greater capacity would that be the right terminology
to store more fat subcutaneously and not inside these organs yes that's absolutely right okay so let me throw back to you what I grasped from your explanation of the twin cycle hypothesis so it all kind of begins with this positive calorie balance so a very small calorie Surplus over a long period of time coupled with muscle insulin resistance this results in an increase in blood glucose or that extra glucose the body has to do something with it instead of forming glycogen in muscle tissue you get an increase in denovo lipogenesis which is the conversion of
glucose to Fat within the liver with the increase in liver fat you get insulin resistance in the liver insulin's job at the liver being to slow down or halt the FL of glucose from the liver into circulation so with that you get an increase in blood glucose the the response from the pancreas there is to increase insulin so insulin levels go up and Insulin then increases or drives more fat production in the liver eventually the body has to do something with that excess fat being produced in the liver packages it up in lipoproteins these vldl
very low density lipoproteins which are an APO containing lipoprotein and are therefore atherogenic and they go out into circulation if the subcutaneous fat storage has been exceeded that excess fat that is now in circulation it has to go somewhere and eventually can begin to build up in organs particularly the pancreas which then can begin to affect the beta cells in the pancreas that produce insulin such that there is reduced insulin in response to ingesting a carbohydrate containing meal and with that you get increase in plasma glucose and the liver begins to convert more glucose into
fat and so forth the cycle kind of self perpetuates did I grasp all of that correctly yes that's absolutely correct okay so I've I've done a 7-hour kind of Deep dive master class on apob with Dr Thomas dpring so we've sort of exhaustively covered why elevated apob increases risk for cardiovascular disease but something that we haven't covered much on this show is why elevated blood gluc ose is such a problem what is it about blood glucose going above a certain level that makes it so problematic well glucose will interact with the small blood vessels to
directly cause damage we know that glucose which is a very soluble compound just look at how rapidly people can stir it into a cup of tea well it is osmotically active it will suck water water from other compartments across a membrane and that tends to damage the very delicate cells that line all our capillaries so the capillaries the smallest blood vessels that are really in contact with our all our tissues are really exposed they're at the front line of damage and so what are the problems of high sugar well primarily disease where the capillaries are
most important in the eye and in the kidney and in nerves that's where they're delivering such a crucial job and they're most exposed and that's where the damage First shows but also the same process is happening inside the lining of the major blood vessels the arteries and that's where the heart disease bit comes in so we've got the glucose effect which is there but but also we've got the fact of the fat now it's the very fact that diabet type 2 diabetes is caused by high levels of uh fat essentially and atheroma and the process
of heart trouble is caused by high levels of fat that's where the two come together so you see the provision of fat as well as the damage caused by glucose leads to the problem in the arteries now cardiologists have tempted to focus upon the cholesterol level and that's absolutely fine as a clinical measure it's fairly useful but it's not a real thing in blood cholesterol only exists to provide an envelope for the delivery of neutral fat which we call triglyceride and that's really the fat I've been referring to through this discussion so that's the energy
source if you like for the body but the liver packages it as triglyceride but you can't put a lump of butter into the circulation so you've got to wrap it in an envelope that will be okay with the watery blood and that envelope contains the lipoproteins including AOA and that's why it's called Uh a lipo protein the protein coat which includes cholesterol and so vldl which you mention yes that's raised about 50% in diabetes 50% what other component of the blood is so grossly abnormal even glucose is raised rather less than that in many people
who develop type 2 diabetes so here we have a gross abnormality and we've shown that with the weight loss and reversing type 2 diabetes it goes back to normal and moreover we've shown the composition of the fat which comes out of the denovo lipogenesis Turning glucose into fat reflects this and that too drops sharply to become normal so yes it's it's an absolutely beautiful process when you see the simplicity of nature working yes in a complicated environment but the processes are actually very simple that's how nature Works simple robust processes it's interesting to to think
about the fact that in this disease State often the focus is just on the changes to blood glucose but as you're speaking to here there are changes to to to blood lipids but I mean is that something that you pause and think about that you know people are are wearing cgms and are hyperfocused just on the glucose component but there is also this kind of I guess derangement occurring with blood lipids at the same time first of all glucose is a very useful index it's just as a general indic index of how the diabetes is
progressing but when we look under the surface in type 2 diabetes it's the fat that's driving the problem with glucose so yes using glucose as a measure of what's happening is fine but it has become a sort of uh mesmeric uh substance that's diverted scientists away from what's really happening now this isn't the first time that this has been suggested a long time ago a fabulous American scientist uh marari uh wrote a famous paper called what if minkowski had been a gusic now minkowski first uh reported this matter of the high sugar but the taste
uh was the thing he could taste it and what if he'd lack the sense of of taste that's ausia so what if he hadn't detected the sugar well he might have tumbled to the fat straight away that was a point mcari was making and ah because it's not been such uh an easy thing to conceptualize and put together in the way the twin Cal hypothesis puts it together it's escaped to tension over the last few decades so yes this is something that uh needs to be sorted out glucose a very useful indicator fat the hidden
driver so we come back to the twin cycle hypothesis at the beginning of it you mentioned there's a positive calorie balance and there is some pre-existing muscle insulin resistance so would it be fair to say that the insulin resistance coupled with positive energy balance that this is Ground Zero does the twin cycle sort of start if you are not insulin resistant in muscle tissue that's a very good question and for most people the answer would be well yes there was pre-existing M muscles non resistance but we know there's a wide range of what's casually referred
to as uh insulin resistance but that's entirely within the range that we see uh in the background population and indeed some people are quite reasonably sensitive to insulin but of course we've got an interplay here we've got the matter of the uh food excess and we've got the matter of the insulin resistance now with the insulin resistance the diabetes will come on earlier but sooner or later with food excess if the person is susceptible then the diabetes will develop so you can see it's really a sliding scale of possibility of developing it and also the
matter of time to uh have this type two diabetes pop out and become uh evident what's causing that insulin resistance in the muscle tissue though in the in the first place is is it the positive energy balance itself is it the sedentary Lifestyles that that people are living the enul resistance is largely a familial characteristic it tends to run in families so the most sedentary person in one family might have insulin resistance that's actually lower than the most active person in another family so we've got genetic factors and the reasons for them are buried in
evolution and it's guess work trying to sort out what was going on but they're there but on top of that we've got two major factors we've got the accumulation of fat because fat will make Muscle insulin resistance as well but also we've got physical activity and exercise and an active lifestyle will maximize the possible insulin sensitivity of muscle in other words reduce the insulin resistance and staying slim will also minimize that so yes as soon as we start talking about muscle ulum resistance we can identify several factors that's L seems a bit a bit complicated
but hey for the individual in front of the doctor they can modify their ulum resistance to some extent usefully by being Physically Active but that's not the the major stop go the major stop go is the constant food intake and just getting that right is there an evolutionary explanation Roy for for why some people are more susceptible to insulin resistance and others are are less susceptible others are better at storing fats subcutaneously and protected against this fat inside the liver and the pancreas well the the usual explanation uh that's offered is socalled the Thrifty phenotype
in other words people who have a body setup that tends to conserve food and take call opportunities to take on board food and the ones who are going to survive periods of famine and food shortage they will just about have enough to get by on other people will have less be susceptible to in um infections for instance die off before they have children and so the population becomes enriched with those people who are best suited to survive famine Now population that have been exposed to repeated cyles of famine such as in India uh particularly and
across parts of the Far East then these people have got a quite a high prevalence of type two diabetes if the whole population is overnourished so that has taken a support for the hypothesis so yes we can imagine uh reasons for this coming about but you know we can never be absolutely certain it's not something we can test in a rigorous way because we would need to conduct experiments over uh many scores of generations of humans and of course that's not with than our gift just to kind of double click on your concept the personal
fat threshold I guess I phrase that I believe that you coined that the personal fat thr hold speaks to how much fat you can store subcutaneously is that right yes that is the essence of it um although there is also a lever component so some people can be very large and obviously have fat Under the Skin excess fat Under the Skin but be metabolically normal relatively small percentage but this is entirely recognized at the other end of the scale there are some severe genetic conditions with absence of subcutaneous fat and guess what they have high
levels of liver fat high levels of fat delivered to the pancreas and a proportion of people get type 2 diabetes now a very high proportion compared to other thin people but even so it's not 100% because some people have the problem with storing fat and the good kind of beta cell that doesn't bother about fat being on their doorstep so yes the personal fat threshold uh is largely a matter of being able to hold fat in the tissues Under the Skin and remain metabolically safe if you exceed your personal fat threshold you're likely to have
diabetes if you're susceptible to it and so in our recent study the retune study we found that getting people in the normal or NE normal body mass index range to lose an average of 6.5% of the body weight they became non-diabetic 70% became non-diabetic so we need to set in context this unfortunate idea that doctors and nurses tend to cling to that if you have a body mass index you mustn't lose weight well that's absurd because the concept of normal is rooted in a population and the advice is being given to one person in the
consultation we're all individuals and I know for my patience that Everyone likes being treated as an individual that person there which I think is about one out of six people with type two diabetes is that right who have a normal BMI what you're saying is that despite the normal BMI and from the outside looking at this person you may believe that they don't have any weight to lose that person has exceeded their individual personal fat threshold and has excessive fat in the liver and pancreas to the point where things like fasting blood glucose and their
hba1c are putting them into pre-diabetes or type 2 Di diabetes kind of territory that's good okay and the Rune study that you just did recently that you just mentioned there that was if I if I'm if I uh have got this right that was the intent there was to see if type 2 diabetes in people of normal BMI shared the same etiology the same kind of cause as type 2 diabetes in people that had were overweight or obese So within this study you were able to actually measure that with the the reduction of fat in
the liver and in the pancreas in these people that have a normal BMI with that insulin resistance reduced and blood glucose normalized that's absolutely correct all the processes that we had shown underlay diabetes in people who were overweight or obese were exactly the same in people who had normal weight now we were able to chase the fat and show that the liver fat was high the vldl triglyceride that we've mentioned before that's high so the minute by minute second byc delivery of fat to the insulin producing cell the the level of fat in the pancreas
is just a marker for that but that delivery of fat continues and the relief of that when people lose weight is associated with recovery of ability to make insulin so yes the retune study looked under the Bonnet and saw the mechanisms of diabetes are exactly the same in these slim people as in heavier people again underlying the fact that tyght two diabetes is a condition of homogenous iology although in heterogenous individuals so if someone's listening and they're thinking gosh I'm I'm in the normal BMI category I'd love to know if I have exceeded my personal
fat threshold would I be right in assuming a a basic blood test that includes triglycerides and fasting blood glucose and perhaps apob or non HDL that those sorts of markers along along with you know waist circumference are going to be a a window into whether you've exceeded your personal fat threshold or not I can't say that we can be absolutely sure on the basis of measurements uh I can give a few guides yes a person who's exceeded the personal fat threshold is likely to have a moderately raised insulin level they likely to have a moderately
raised fat level triglyceride level um um and also they're likely to have gained weight in adult life so many people regard themselves as being normal weight but they're comparing themselves with their uh their friends of similar age all of whom have put on weight and when we ask the critical question can you wear the same trouser waistband as you wore when you were 21 then people get it they can't fit into the size say 32in trousers they wore at the age of 21 uh they're now 35 and they think that's okay well it might be
okay for most people but it might not be for them so you see it's a matter of likelihood and all I can say is that the personal fact fesal can only be defined as exactly if a person has Type 2 diabetes loses weight and discovers for themselves where that threshold lies for some people and we know this from our biggest study the direct study some people need to lose all 15 kilog in fact one person needed to go on to 20 kilg to get rid of the the fat sufficient to get rid of the uh
excess above the personal threshold but some people only needed to lose a small amount the majority needed to lose at least 10 kilg so you see that's how the personal fat threshold works but at the moment despite my best efforts we've tried to develop ways of measuring it I can't offer any concrete way of knowing for certain there's only a matter of degrees of risk at the present time and you said there the only way of knowing is to to lose weight and I mean assuming to to there you're mainly keeping an eye on blood
glucose and I say this with the definition of remission I guess in mind here you'd be looking at blood glucose returning to the normal range without any type of blood glucose lowering medications is that how you would know that you are below the personal fat threshold yes that's the that's the final orbitor and also we would expect the level of triglyceride to Fallen by 30% you know it's 50% raised at Baseline coming down to normal is a fall of uh I uh 30% you mentioned before that insulin levels could be elevated this gets me thinking
about kind of predicting your risk of developing type 2 diabetes and and I I've seen mixed views on this about how accurate measure you know insulin um lab sort of uh assays are but you know before we get to the the assay itself what you're speaking to here is that in that early stage where you have this increased fat in the the liver and with that you get um increase in in blood glucose and the pancreas responds by producing more insulin so at at a certain stage of this kind of Journey from metabolically healthy to
type 2 diabetes you might have normal blood glucose levels but have elevated insulin because the pancreas is kind of trying to compensate and producing a lot of insulin but you are able to keep blood glucose in a kind of quote unquote healthy range is is that a kind of early predictor an early kind of alarm Bell so to speak that you're on your way to type two diabetes that you your pancreas and those beta cells are kind of fighting for their life and you're just hanging in there at that moment unfortunately the range of normal
levels of insulin is such that it's very difficult to do a single test and say Ah that's raised so the usual quoted normal range for plasma insulin first thing in the morning is 2 to 11 uh Millo per L milliunits per liter but that gives it all away if a person who usually runs at 2 m per two milliunits per liter uh has risen considerably up to say five or seven they don't stand out at all it's only those people in the upper range who would move themselves outside the so-called normal range so it's it's
not precise unfortunately and precision is a matter of being certain that the outcome of a test uh indicates what you think it might indicate so the Precision for a fasting insulin is quite low and there are one or two other factors transporting insulin to the lab is a problem if it's left in contact with the the blood cells especially the white blood cells then the levels will go down steadily because the enzymes in the white blood cells will tend to be breaking it down and so it needs to be separated early it needs to be
chilled it's a difficult measure to make the there is one other substance that is measured alongside insulin often and that is thrown out at the same time as every molecule of insulin this bit of if you like garbage that helps in the manufacturer is thrown out and that's called C peptide and it's actually quite a useful measure of insulin secretion now in blood samples it is relatively unstable and again you need to handle the sample carefully but in fact in urine samples it is quite stable and although it hasn't entered any sort of routine uh
use at the present time the overnite um C peptide level in urine is a reasonable Guide to the amount of insulin that's actually being produced and that could well be a simple test of the future but you know I'm speculating here and looking forward uh to indicate what might be possible and that really underscores the fact that no don't rely on blood tests at the present time other than other than glucose to glucose and trios ride to detect the earliest risk of type two diabetes you mentioned there that uh another clue is just looking back
at the past decade or so and seeing if you your weight has crept up I've seen in the literature this kind of uh recommendation to keep your waist circumference to half of your height and I saw a few studies mentioning that that was a decent predictor of metabolic syndrome is that something that you've come across yes indeed and it would be a far better measure than the body mass index not perfect but better and indeed it's one thing that I have in mind to do where I have uh some uh uh spare time to go
back over the data from our studies and look at the weight height ratio and see how it just pans out how it is is a risk factor how it is um obviously it's a good um it's a good measure of the weight loss naturally because you've got weight over height um but as a risk factor yes it is actually uh a step forward and if only we could move away from relying upon BMI and imagining these fixed thresholds you're abusive your BMI is over 30 well no uh it doesn't work like that because of different
body types and so uh these amazing individuals who are playing in the Rugby World Cup at the present time they're not obese but many of them have bmis over 30 they're just uh heavily built guys with of course the additional training if we're thinking a little bit more here about preventing type 2 diabetes and someone kind of wanting to know what their metabolic health status above and beyond triglycerides looking at at your fasting glucose your hba1c making sure that all those things are in the normal range waste circumference the height Rao which we just spoke
about is there any extra predictive power or rationale for dexa scans for example that often have a visceral fat kind of measurement or liver ultrasound or using continuous glucose monitors what do you what do you think about these sorts of things for the general public or someone who's listening and just wants to understand a picture or get a kind of look into their current metabolic health I think I would advise such a person that the the waiter uh a happier life is to stop worrying about it but to ensure that the weight is approximately what
it was in early adult life or if there were actually too heavy then to bring it down a bit now one measure we haven't talked about so far is a percentage body fat that is something which again has a moderately wide range men you'd find having a total percentage of the uh the body as fat would be between about nine and about uh 20% in women it's higher of course that's just how uh biology setup and it goes from the low 20s up to say 32 so if you're above that normal range well you know
we really ought to be considering shedding some weight because that's a that's a measure a direct measure of the uh fat and this is something which is easily done with these uh fat monitors that you can find in gyms or uh even in chemist shops so yes percentage body fat is an indicator but really just adopting the Z loss we need to maintain our early early adult weight weight gain in adult life is 100% fat so that really would be my main message and embarking upon tests that have a low Precision has got a huge
problem and that is inducing in worry so I wouldn't advise people to seek out tests uh unless there's a high prior probability of issues for instance if people in your family have type 2 diabetes that changes the relative benefit and the Precision of all these tests and pushes it up it's a it's a funny phenomenon that we call prior predictability and so yes if there's reason to believe that you may be at risk of type 2 diabetes then embarking upon tests especially a simple fasting glucose test is a very reasonable action otherwise you open the
floodgates of worry leading to need for more tests more investigations and uh not necessarily improving your total happiness in life right no I think that's very sound advice and even even if you have that family history uh I guess it's still important to be using tests or getting tests that have been shown to be useful and predictive and um so that you can actually make meaningful decisions with the data that you get um versus some you know versus some of the things that you might come across online that seem very Cutting Edge but haven't necessarily
been put under the scientific method and um with that it may be that we don't know what to do with that data and that's where that anxiety and stress can can creep in because you've got a result that you know we really don't know what it means that's absolutely correct and I you've taken the words out of my mouth because we just going on to say that there are various offers online of doing marvelous tests and divining things that uh just wonderful and tell you about your your personal metabolic State and your personalized nutrition and
basically they're not reliable they're just completely money-making uh scams unfortunately often they're mixed in with good points and so yes many of them would Advocate weight loss not all of them point to sensible ways of losing weight but there is a problem if an author is dressed up in scientific terms say we do continuous monitoring and uh find out what sort of person you are and then we advise you what to do well that's Hy um and basically uh throughout throughout human history there have always been charlatans and the present age is no exception it's
just that the effect has been magnified um by the availability of information over the web so how do you feel about continuous glucose monitors I think I can guess but you know there probably is some listeners who are thinking surely that can't be a bad thing Roy I eat a meal I have this continuous glucose monitor on my arm I can see how my body responds to that meal is blood glucose elevated or I guess quote unquote spike is the term that's often used by many of these companies and in sort of laye on line
is there any utility to a continuous glucose monitor in a person that does not have pre-diabetes or type 2 diabetes as a way of determining if they're developing fat in the liver and in the pancreas and perhaps on their way to developing type 2 diabetes first of all the continuous glucose monitors fabulous devices for people with diabetes they especially with type one diabetes those people who need to take insulin they a complete Revolution and so this is an enormously exciting field but coming back to your specific question we don't yet have the information upon how
precise the uh application of continuous glucose monitoring can be it has the advantage that you can see whether uh first thing in the morning your average glucose is always absolutely unremarkable you can see whether your average after meals say after your evening meal when you been eating three meals a day hopefully no snacks in between well 2 hours after your meal how high is the glucose well you can easily take a an average of that it's possible that may give a clue it would certainly show up if a person was heading for pre-diabetes sorry it
was developing uh in the stage of pre-diabetes but we do not have the information about how precise it is how many times would it give the wrong answer and that is the information that we don't yet have this will come with time so it will be possible to answer your question but to my knowledge at the present time we can't be certain that the uh that the information that what would derive from a state of normal glucose tolerance would be sufficient to say Hey you know in a few years I'll be heading for pre-diabetes we
don't have that information okay so for now in order to know if we're above or below our personal fat threshold we're thinking about whether we've had weight gain in our adulthood looking at the Weist circumference the height ratio we're looking at our fasting blood glucose which you can get on a standard blood tests we're looking at Tri glycerides hba1c these kind of established uh biomarkers and percentage body fat and percentage body fat and you mentioned there are males sort of are in the ballpark of 9 to 20% and women from low 20s to 32% um
coming back to the personal fat threshold you you spoke before about the role of genetics and that genetics can kind of dictate how much body fat you can get away with before it starts to lead to this excess fat in the liver in the pancreas which results in this um elevation of of blood glucose is it just genetics I've seen various studies that have looked at at some interesting things like for example sleep deprivation I saw a study looked at sleep deprivation and granted following severe sleep deprivation people consumed more calories so I guess that
comes back to the start of the twin cycle the the excessive calorie component but not only do they consume more calories they seem to be storing fat more preferentially viscerally and then also um if we think about certain life stages there's quite a bit of data suggesting that as a woman enters menopause body fat distribution can change and there can be more of this kind of abdominal fat so is there you know other factors at play here like sleep and hormones that can dictate where you're storing fat certainly but these are all wrapped up in
the individual as it were although you mentioned some potentially uh uh temporary or modifiable things such as sleep deprivation yes the sleep deprivation uh The Chronic sleep deprivation will certainly raise levels of cortisol now cortisol is a is a hormone that has powerful effects throughout the body in clinical disease caused by excess C cortisol fat is stored centrally uh a so-called lemon on a stick appearance of people with this severe condition whereby the muscles are wasted but the tummy is expanded with fat so yes chronic sleep deprivation we can understand that with regards to the
menopause yes certainly there is uh a difference in distribution of fat and the difference between men and women in terms of illnesses caused by fat tends to narrow after the menopause because of because of that um so those are factors there one interesting area that uh is now coming into Focus for some time in animal experiments it's been demonstrated that if uh a rodent is uh overweight or made diabetic during pregnancy then there's a higher rate of diabetes in The Offspring of that Ro now for many years this was regarded as curious because human data
didn't seem to point to that but now it's been worked on for so long it does here that there is uh there are additional effects that we would call epigenetic effects in other words just modifications not in the genes themselves but in the proteins and carbohydrate molecules around the genes that cause different function so yes uh there is certainly epigenetic effects that will contribute to this um and so this may explain some part of the steady steady rise of diabetes under conditions of stress but if we set aside all of that when food deprivation kicks
in then we see everyone in the same boat and so take away the food you take away the diabetes so yes there are other factors but the Simplicity underlying it all shines through in the sense of what we know when push comes to shove and food is calling the shops so if you take away the food take away diabetes that's that's different to saying type two diabetes that's different to saying that there is no genetic component to type 2 diabetes what you're saying is that not everyone Who develops type 2 diabetes sorry not everyone that
is overweight or is obese will develop type 2 diabetes but most people five out of six who have type 2 diabetes if they were not overweight or obese they would not have type 2 diabetes would that be accurate that's correct yes when people who have say a body mass index of 45 lose substantial weight go down to say 41 they don't have diabetes so they's still obese but they don't have diabetes but of course that's the operation of a personal fat threshold again they've just come down and so it's not a matter of totally getting
rid of the Obesity that would be ideal perhaps but no we're just talking about the metabolic side of things here and so people can remain obese but manage to get rid of the diabetes even within that free quick one folks I get asked all the time about buying supplements and getting blood tests the good news is I've created comprehensive and completely free guides for both simply head over to my website the proof.com to download them that's the proof.com okay let's get back to the episode and coming back to the direct trial which you mentioned before
which I guess is one of the more prominent Trials of yours that's tested the twin cycle hypothesis um it was 15 kg I think you mentioned that seemed to be an important kind of number 15 kg of weight loss so that was the the typical weight loss that was required for people within that study to get enough fat out of the liver and pancreas to enter remission the uh average weight loss immediately after the low calorie phase which in direct was a 12we phase the average weight loss was just over 15 kilograms so yes that
was an average but uh some people needed all of that 15 kgam weight loss to get rid of their diabetes because putting on even a small amount of weight allowed the diabetes to come back when we tested subsequently other people could manage to put on quite a bit and still be free of the diabetes so that at 2 years down the line because direct was a 2year randomized control trial two years down the line in the weight loss group the average weight loss uh had uh dropped to 8 8.8 kg and even so onethird uh
of the entire group was still in remission from the diabetes so you see uh that's that's how it works I ex we need to aim for the 15 kg weight loss that will take most people into the range where the chances are they'll be free of diabetes that has the important effect of demonstrating to everyone concerned the possibilities so if at say 15 kgs a person is in remission but then life kicks in and they're distracted with other problems and the weight increases by say 3 Kg they're going into 12 kilg if there's still three
of diabetes Well life goes on but the chances are that they will just continue to put on a bit of weight especially if discovered they can uh put on weight without getting their diabetes back suddenly say at 10 a half kilog the doctor says well I'm sorry you've got your diabetes back again what do you want to do about it are you're going to lose more wait again or uh I can give you these drugs well you see the target of 15 kg is fairly secure and a good Target for most people and it's also
a wakeup call along the lines of get real you know how much extra fat do you think you're carrying around because most people in our Studies have put on more than 15 kg than they were when they were in early adult life so 15 kg is not a complete return to a state of Youth it's a return most of the way and will be sufficient to achieve the metabolic goal so in indirect you mentioned there was a 12we low calorie dietary intervention average weight loss was 15 kg so was that average weight loss Roy from
the 12we low calorie intervention and perhaps you can explain to someone what that kind of looked like if they haven't heard it heard uh that being explained before or was that 15 kgs achieved through the two years by doing this sort of low calorie cycle multiple times no and this is one of the really important points of uh our work that to lose weight it's much easier to do it in a short distinct period of time you've got a short Focus period of time you can plan when to start it avoiding birthdays and wedding anniversaries
maybe and uh you know that okay you're going to have to give up certain things per perhaps avoid some parties during that time so the Define nature of this low calorie period is quite important also the original reason why I design this this approach to weight loss to test the Counterpoint uh to test in the Counterpoint study this twin cital hypothesis the original reason was that the old literature pointed out that what they called very low calorie diets and they were very low were not associated with Hunger now that was a fascinating detail that has
stuck in my mind from the old literature and so that was one of the reasons I went for it and indeed we find that people are very hungry over the first 36 hours but you just got to tough it out if if you feel too hungry drink a bite of water have a list of things in advance to do fixing that door on the cupboard or uh going out and sorting out whatever in the garden so that first 36 hours is difficult but after that people suddenly find that they're not hungry all the time despite
only taking this diet which in direct was for 200 calorie liquid uh shakes that's a packet of Powder made up in a pint of water partly because it's high protein about 25% protein it's actually quite satisfying and it does actually fill you up uh that's the recipe for restricting yourself to 200 uh to 800 kilocalories just 200 per meal as I say inir we use four sashes a day in our early studies in Newcastle and continuing now we use what we believe is a a better accepted version which is just three shakes a day but
uh a large plateful of salad Foods or non-starchy vegetables that allows people to enjoy feeling crunch it eases the matter of this second phase which is moving from the low calorie diet back towards normal eating how do we do that after Counterpoint I was surprised when people came to me and said look doc it was actually much easier than I expected going on this low calorie diet but it was so difficult coming off it so we had to design a stepped food reintroduction so in counterbalance we introduced one meal and just kept on two shakes
per day and then we introduced a second meal a week later and Carri it on with one shake a day and then finally after a further couple of weeks we drop that final shake so people gradually got used to how much of normal food to eat what to eat and having a blank slate upon which to write new dietry habits is really rather good and so we can re-educate people and all of them are primed in advance that when they get back to eating normal food they can expect to eat only about 34 of the
amount they were habitually putting on their plate beforehand that's quite important they need to know that in advance those are all ways that we try and set up the most difficult phase the most difficult phase is keeping the weight off in the long term because if you look at it biologically you have the same person doing the same things in a same environment fast food environment an environment where it's become socially acceptable to eat when you're walking down the street even according to Hollywood to eat when you're talking where did that come from you see
the social change in the last 50 years has been astonishing around food but that's all part of the obesogenic environment it's not just the fast food and the availability of food constantly and uh the the lack of uh the lack of satisfying nature of fast food that's all part of it but avoiding that and keeping your weight constant that's a Class Act and that's something that we don't have easy answers to but uh people who are sufficiently motivated can certainly do it so that it 5 years from our direct study these are data that we've
presented at scientific meeting are not quite yet published but I can say at 5 years people were still very considerably below their starting weight the average weight was still 6.1 kg below Baseline now for a dietry study at 5 years that's never been achieved before now only those people who kept off an average of 9 kg were still in remission at 5 years but that says it all because it's a matter of yes getting the weight off but the human difficulty is one that I'm very alive to and we're constantly working to try and improve
this matter of preventing weight regain after this very successful m method of losing weight what percentage was that Roy of the the intervention subjects who were able to to uh stay in remission and Achieve that 9 kgam weight loss at 5 years of the people who are in remiss at 2 years it was 26% her in remission at 5 years but overall if we look at the line up on the starting line 149 people uh started off in the weight loss group then it was uh 11% of those 149 people we lost track of some
of them but we still count them in saying 11% if we stick to the information we know for definite then yes 13% we earning remission so in round figures around 12% you might say but that's that's not very good hey if we use a drug we talk about number needed to treat and a number needed to treat that's quite good would be about one in 10 one in 12 so if you use a drug then what in 10 people are going to actually benefit from it for the reason that it's prescribed to prevent a heart
attack for instance but here we have a simple dietry lifestyle information method that produces more than one in 10 of remission of uh a disease which causes terrible morbidity and early death so 12% has got to be set in perspective and it's good it's not good enough we can improve on this but of course that is a challenge for medicine and healthc Care Systems to use this information and to put it to good use yeah and that 11% or 13% is also not considering the potential benefits that people would have had who did enter remission
who are perhaps not in remission but surely there is some benefit to improved blood lipids and improved blood glucose for a period of years when you're considering your overall risk of cardiovascular disease for example yes and please you ask me about that because this is one of the most traumatic IC findings again uh as yet unpublished I hope it'll be published in a few weeks time but it has been made public uh at scientific meetings if we take that 149 people on the starting line for Direct in the weight loss group 149 in the control
group the risk of any serious illness was hared in those people that undertook the weight loss so me really starting off on the weight loss even though some people dropped out quite early small number but they did the overall adverse event rate was half now what was driving that well there were a few less Strokes the numbers weren't large enough to show a difference in heart attacks we had very few of those but the main difference was in infections of all kinds including leading to Serious foot infection and in new cancers now in the people
in the weight loss group uh the number of cancers that they deliv developed in in five years was one and that was in someone who dropped out early and probably didn't lose weight the number in the control group that were treated according to Conventional best practice was eight now these numbers are small but hey a ratio of 8 to one of new cancers cancers that we know are related to overweight and obesity that is a fabulous outcome of the direct study so yes health benefits of weight loss are very considerable and can I just make
a jump forward to knock on the head a silly idea that's been around for a long time yo-yo dieting is bad for your health that's nonsense there's no uh consistent information that losing weight and putting it on is bad for overall health in the weight range we're talking about so we can be sure that people who lose weight and keep it off for a while and over a period of time have reduced their average weight they will gain hugely and they will be not only healthier but also also happier people to kind of double click
on that concept of yo-yo dieting and coming back to this intervention so just to be clear when you looked at the the 5-year data and I think you said there was 26% of of people that were were in remission or 26% of people in remission from 2 years were still in remission at 5 years is this still a a group of people who only did that that low calorie intervention that 12we intervention that was 800 kilocalories a day and they only did that once they weren't repeating that over the the years to come if they
put on weight they were offered the possibility of using the low calorie products again because what we discovered in direct was that people of course put on weight during times of uh stress due to family illness due to financial reasons all these factors uh kick in and when someone is busy dealing with this the the matter of concentrating on food intake and keeping it down goes out of the window so we feel the commonest reason for weight regain was a sudden event which of course passes and so when that event had passed we offered people
the chance to regain the uh the previous Advantage so that was a process that was running in the background and in direct half of all the participants needed at least one of what we called a rescue package so yes this is part of the business of avoiding long-term weight regain and so if people put on weight it's not a failure it's just something to be dealt with so yes some people did have short periods of low calorie intervention to get the weight back down again but by and large they were just living entirely ordinary lives
eating ordinary Foods trying to avoid fast foods um and keeping an eye on their weight I think you said 36% of of the subjects in the intervention group in in direct achieved remission at 2 years which is remarkable that's that's an incredible result to see but if you if we flip that statistic just for a moment and and let's let's think about the individuals so let's think about the two out of three individuals who who come back and and are not in remission so that's 64% what are the main reasons that you believe would explain
why they didn't achieve remission well there really a we regain that's sticks out uh a mile so uh the people who were in remission uh maintained the weight loss far better than the ones who relapsed and so that was very obvious for instance at the fiveyear Mark when the average for the whole group was a weight loss of 6 Kilograms but that was uh swayed as it were by the small group who were in remission who were still at uh just under 9 kg 8.9 kg weight loss so uh if we'd look at the people
who'd lost remission my uh rough calculation would be probably about 5 half kg below Baseline compared with nine to stay in remission over 5 years so that's how it Stacks up so that's the main reason and of course you could look for reasons underlying that and life stresses are a big uh a big matter uh changes to social circumstances Etc so these are these are things that affect real people and as doctors we just need to advise how best to navigate those but I think having demonstrated the biology of type 2 diabetes having it shown
what a simple condition it is uh in to managing concept it helps doctors deal with all these complexities because life is complex and I wouldn't believe wouldn't uh suggest for a moment that this was a simple matter for an individual to deal with but we can see the main factors and deal with them that's really the exciting uh the exciting consequence how important is how long someone has had type 2 diabetes IES I think I've I've read in your work that this strategy of weight loss and getting below your personal fat threshold is more effective
in the person who still has some beta cell function and can can with with weight loss can start to get a normal kind of insulin response can you kind of speak to that and I guess the the importance of once if if you are diagnosed with pre-diabetes or type 2 diabetes the importance of trying to lose that weight and get below the personal fat threshold as quickly as possible yes so there's two questions really there one is achieving remission in the first place the others keep how long you can keep it off so achieving remission
in the first place uh this is strongly influenced by the duration of Prior uh diabetes now in their the famous Counterpoint study that proved the twin Cal hypothesis I opted to study people only in the first four years a completely arbitrary decision but we had to start somewhere but in counterbalance we tattle the question okay will we see the same information the same results if we study people with long duration type two diabetes as well so in counterbalance we had people with duration of just a few months of diabetes up to 24 years and we
showed very clearly that the longer the duration the less likely uh the chance of permission was perhaps down to maybe a few percent chance 5% at 20 23 years which is the uh the longest I've observed personally um but in reality we know that the short of the duration that's the most important factor for remission assuming the weight loss and so taking up your pre-diabetes Point yes pre-diabetes that's the time to act because you will almost certainly be able to achieve remission of diabetes assuming it's true type 2 diabetes but how long can you keep
it away well provided weight is kept down from all my observations it suggests that diabetes will remain away as long as the body avoids weight regain my longest duration personal patient is uh uh coming up for 19 years and so yes duration is uh a real factor and if people keep the weight loss off remission is going to be at least prolonged what is it about the duration Roy is it is it that the longer you are above your personal fat threshold the more damage there is to these beta cells and they just eventually lose
the the ability to secrete insulin yes the most dramatic piece of information from the counterbalance study was that people who went into remission had an insulin response at Baseline when we first tested them in the diabetic state that was pretty poor it was about half normal the group that didn't go in remission had an insulin responsive Baseline that was almost nonone so you see there was that flicker of Life still in the people who went on to be able to get remission so yes it is a matter of how long the insulin producing cells the
beta cells have been exposed to fat and of course glucose because the fat assault on the beta cell is joined by a glucose assault on the beta cell and that's why in diabetes the beta cell continues to go downhill so there's a lot of different I guess dietry strategies out there to to to help create a a calory deficit and and promote weight loss and there's a lot of debate and fighting between low fat and high fat and you know different styles of of kind of dietary restriction I'm assuming that your view here is that
the best option for at least some people we can go into who that might be or might not be is to utilize a sort of one of these very low calorie diet intensive you know short duration it's not a lifetime thing you kind of rob the bank or I think you say in your book seven days to slay the monster um is is that where you're at that if if you had pre-diabetes or you had type 2 diabetes that you think that's the most effective strategy for someone to adopt from a dietary point of view
yes on average although individuals may have individual preferences circumstances may vary so that other other ways May suit but there are some really important points to make about achieving weight loss the most important thing is that you achieve it and so setting this goal of 15 kg weight loss for most people in the overweight or obese range is important you realize how much you've got to lose now just fiddling with the components of food raising or lowering this or that is not going to achieve that you need to have a very substantial cut back in
say uh the fat content of food which would make it unpalatable for many people the carbohydrate content of food well certainly in the UK very low calorie di very low carbohydrate diets are quite unpopular they're not sustainable as people actually feel they need some modest amount of carbohydrate so changing the composition is not terribly good in general however there are as many successful diets as there are different individ s and some people really don't mind a low fat diet some people don't mind missing out all carbohydrate foods but they're few and far between and that's
why landeron studies randomize people to a group of this diet compared with that diet but of course in this group just imagine you've got half of people that suit the one and not the other and in the other group you got half the people that suit uh the other are not the one and so they end up having results at are 49 51% and so it's very understandable that there's confusion in this area so how to approach it well for the individual you've got to suck it and see I would advise going for the low
calorie diet getting rid of the type 2 diabetes that's the go-getting aim but if for some reason that's unre ible or found to be absolutely impossible then why not try one of the other methods the Mediterranean style eating with low carb is probably the best uh researched and intermittent fasting is probably uh the second best researched and used in practice other forms of dieting entirely possible let's move to the Other Extreme for the moment and take the celebrity diets a celebrity says well you know what I did was to only eat kiwi fruits and absolutely
nothing else well it somehow suited them maybe they are not being quite straight in reporting the total amount of weight they lost due to that alone uh maybe there was assistance from other uh other means so any diet can work if it suits the individual and we have to mention at this point there all other ways of losing weight in extremists if people have tried all the methods and they find the appetite Drive still uh produces failure well those parad surgery which is very successful although does have a higher complication rate than surgeons admit to
and then we've got the new magic drugs well no drug is Magic these come along with side effects and they've got to be used carefully and properly but if you use carefully and properly then they can achieve weight loss and they too would do the bit so we've got a range of measures my work has established what can be done within the constraints of the NHS as that is a very severely cach limited service cash restricted service you might say and uh I had to demonstrate for a thing to be useful it had to be
low cost and this is a highly coste effective way of going about weight loss which makes it suitable for Health Care Systems just to clarify the the kind of magic drugs you're talking about there are drugs like glp1 Agonist like OIC which I'm sure a lot of people have have heard of and to kind of I guess underscore a point that there that you made about diet studies and how they may have certain people randomized to a group who do well on a certain macronutrient ratio some that do poorly and then in the opposite arm
the same thing I previously had Professor Christopher Gardner on the show and he spoke EXA to exactly that point about diet fits and one of the interesting things that they looked at um and that was a 12mth low carve versus lowfat trial and know that you'll be aware of it um but the average weight loss was not significantly different but when you went in and looked at the waterfall plots you did C on each arm some people did poorly on low fat some did well and same thing with low carb um so to your point
at this stage without being able to predict who's going to do best on low carb or low fat then the individual can kind of play around with it and see what feels easiest um for for them I do Wonder though in one context Roy whether there is an advantage to a low carb diet so if we come back to the person that's had type 2 diabetes for quite a while and their pancreas is just completely beat out they can't produce insulin even if they're they're losing weight they're one of those people that are not entering
remission do you think that is a context where a reduced carbohydrate diet might have an advantage sure but it depends what level you're starting from and that's the whole point the matter of low carb the whole debate has been uh made Complicated by the fact that people were talking about different things now in the UK we're talking about perhaps 55% carbohydrate consumption on average that means some people are taking 65 70 for them it will make a huge difference to uh the diabetes as you describe it to drop down to say 45 which is a
very sane uh level if someone was toling along at 45% carb intake dropping it further probably won't make a huge amount further difference because uh there the body is coping and it needs a certain amount of carbohydrate uh to function optim and so we've got this difficult matter of what is excess certainly uh having sugar sweeten beverages is an obvious excess that can be cut out adding sugar to tea and coffee don't do it taking desserts well perhaps uh in limited quantities how about the big sources of carbohydrate that is potato rice pasta bread well
that needs to be looked at and it's certainly sane to have a moderately carbohydrate reduced diet probably the ideal is a Mediterranean style diet and though with lots of salad uh non-starchy veg products and moderate uh carbohydrate reduction hey friends if you'd like to stay connected and reinforce the valuable insights from this show let's connect on Instagram you can find me Simon Hill that's at Simon Hill I look forward to seeing you there all right let's dive back into the episode how important is overall diet quality because we've spoken a lot about energy and I
guess at at the beginning when outlining the twin cycle hypothesis you kind of underscored this uh very small but longlasting calorie Surplus kind of being at the base of the development of type 2 diabetes but I've seen quite a few studies that have looked at uh for example comparing different types of fats in the diet so comparing foods that are rich in saturated fats versus foods rich in polyunsaturated fats and and seeming to show that when you swap calories from saturated fat for polyunsaturated fats that there is an improvement in insulin sensitivity and a reduction
in liver fat are these things important for people to also consider sort of above and beyond calories and weight loss the kind of makeup of that dietary pattern and you know the types of macronutrients that they're consuming you'll get much more bang for your buck by reducing the total amount of food eat than by changing the composition of food the reason is the body sees relatively little of the food you eat it goes through the liver the liver will change the fat it will take carbohydrate and turn it into fat excess carbohydrate as we've mentioned
gets turned to do 100% saturated fat that is really quite a worry and by excess we're looking at people taking you know 60 70% carbohydrate uh in their diet which unfortunately is entirely uh unremarkable in terms of the population so yes the only sane approach is to uh avoid obvious sources of saturated fat without decreasing your enjoyment of what you eat and so using uh olive oil using uh monounsaturated or polyunsaturated oils for cooking yes that seems to be a no-brainer uh not using excess that also is straightforward not eating excess fat I think perhaps
that uh thick layer of fat around your pork chop is best left on the plate so there are certain obvious steps that you can do to achieve moderation that word that's so often used but rarely defined in this dietary composition so yes dietory composition matters but if you were to ask me what's the number one uh uh consideration what's the number one characteristic of a healthy diet it's to take in the amount of energy that your body needs from day to day and not to have excess year on year so avoiding energy toxicity really yes
and I know this might take us into the weeds a little bit but I'm interested why is it that saturated fats have a a differing effect on the liver on hepatic fat or insulin sensitivity at the liver compared to polyunsaturated fats is that a mechanism that you have come across I don't think it's completely unraveled but at the level of the molecules operating in the cell if you have saturated fat it's a it's uh a carbon chain which is very bendy if you have a Monon saturated fat it's got an angle in it it is
a different substance for the the cell apparatus to handle and so the geometry of the molecules May well be an important part of what we see as to what comes out at the other end so that's the best answer I can give uh Bridging the epidemiology just reports a phenomena to the absolute molecular level and so that's the state-ofthe-art as far as I'm aware perhaps uh switched on by a chemist might be able to give a more precise answer but as I understand it it's the handle of the molecule that is produced because these fat
molecules are long this saturated fat produced by the liver is 16 carbons and most of the fat molecules in human blood are 16 to 18 carbons and they're usually long and flexible change that and you change the behavior of the fat I think that's really the overall answer at the present time you've mentioned a few times that the body can convert excess carbohydrates into fat in the liver I just want to clarify something here I think that there's this you know pervasive view out there that carbohydrates they're driving the weight gain and and diabetes and
you know you and I know that not all sources of carbohydrates are are are equal you know a jelly bean I often say for example probably doesn't have the same effect on our health as a black bean but what would you say to someone who's been led to believe that all carbohydrates are bad and because blood sugar is elevated in people with type 2 diabetes carbohydrates must be the cause of type 2 diabetes well I point them to the simple way that uh the Body Works and allowed them to wake up this morning because they
only woke up this morning because their brain was supplied with glucose second by second throughout the night now where did that come from well it came from the blood but hang on there's a funny business here because the blood glucas level didn't drop overnight it was constant yes so where's it coming from it's coming from the liver the liver puts out enormous amounts of glucose overnight uh you'll put out 10 G every hour that's for an average siiz man uh in average Health but in diabetes you're putting out about 15 G an hour so it's
not to do with the food you're looking at metabolism determining the blood glucose level certainly the food eaten won't help and so avoiding excess carbohydrate is absolutely um a sensible move trying to go to very low levels of carbohydrate well if that's the only way a person can lose weight and therefore change the internal workings of their body then yeah you could do that but going from moderate carbohydrate downwards doesn't make much difference to the liver which is busy functioning away setting the blood mucose level the third macronutrient is protein and you mentioned before that
your low calorie me placements they were high protein I've come across some interesting uh data recently that um to my understanding sort of suggested that certain amino acids May trigger insulin release uh in people with type 2 diabetes whose beta cells kind of no longer respond well to to glucose and and what I've read is that the the kind of nutrient sensing Pathways may be different so there can be this dysfunctional glucose response but the protein response within the pancreas is kind of preserved what do you think about that and this idea of maybe using
protein perhaps at the beginning of a meal to kind of trigger the release of insulin and and perhaps better handle them you with carbohydrates well we did actually report that could be used to limit the biggest rise in blood glucose in people with type two diabetes which happens after breakfast so taking a high protein snack we used soy beans uh and yogurt as a recall to achieve this uh 2 hours before a standard breakfast resulted in half the rise in PL glucose levels now all that work came out of investigating What's called the second meal
effect if you look at the blood glucose rise after lunch it's much smaller than the blood glucose rise after breakfast even if you eat the same Foods at the same meal time in the same quantities and I was busy investigating that because I thought that it was a matter of the uh protein mode and we use protein not to try and stimulate the beta cell but to suppress the levels of fat production because it would cause a very slight increase in insulin but that would suppress fat and I thought that would make the body more
insulin sensitive and indeed it does so the bottom line is what you say has got some degree of Truth in it but when we come to looking at studies of trying to reach stake to minimize um the effects of diabetes that doesn't quite work all the way through so I can't say that having a high protein diet would make a significant difference over and above the factors that we've mentioned in your interventions there didn't seem to be a focus on exercise and I guess given the importance of sceletal muscle in glucose homeostasis I wondered if
you'd ever considered um the inevitable kind of muscle loss that that comes with losing a significant amount of body weight particularly if you're not doing resistance training concurrently sure focusing for a moment on the the loss of muscle mass uh this is something we measured it was uh uh a 4% decrease in uh uh fat free mass of the body in the Counterpoint study so we measured everything in that first study now if I persuaded you to walk around every day wearing a weights vest that contain 15 kg of weight guess what your muscle mass
would increase by a few percent over 8 weeks if people lose 15 kg the muscle mass has to decrease because every day they're carting around less body and the muscles we're talking about are the muscles you never think about very much that the huge muscles maintaining the posture of the lower back and keeping the hips in the right position those are the real energy consumers uh during moving ourselves around our curious race of bads we rely on those muscles and a lot of uh energy there so when people are 15 kg lighter there's a physiological
reason for them to have less muscle mass this has being completely misinterpreted as OD DEA the weight loss causes loss of useful muscle well no it's what useful muscle the body decides how much muscle is useful by how much work it has to do every day you can prevent this using resistance exercise and that's absolutely right and I would add that in the Newcastle magnetic resonance Center we've not just been researching uh food and diabetes we also do exercise studies on Ordinary People couch potatoes and athletes so this is an area that we're really very
tuned into so our studies of resistance exercise show very precisely that uh that is a very good way of building muscle why didn't we use it in Counterpoint well the reason relates to one of our excise studies which took a group of inactive people and got them to train up and made measurements on them throughout this period so that they could do a half marathon they all completed the great North run I have to say they didn't all run it uh there was a lot of walking but they all did it and moving from their
totally sedentary uh Behavior to doing this was remarkable what happened to the level of Fitness it went up remarkably what happened to their weight it did not change now they had urance huge amounts of energy in the training in during the race why hadn't it changed after every research project we invite back our participants to uh hear the results we explain the results for them what they've gone through all these trolls of measurements for as well as finding out how it was for them because that's how we learn how people can perhaps have studies done
in a more tolerable fashion we learn how for instance a diet was affecting people but in this case I wanted to hear how it was from these people uh after all their training and I said one of the funny things is the average weight stayed exactly the same even though you were burning so much energy and I expected it to drop and this lady put up a hand and said you don't understand when you're coming back from your half hour walk you've only got one thought in your mind I deserve that pie and suddenly I
had a completely different perspective on ordinary people doing much more exercise than usual and the thoughts and behavior that elucidated so I went to the literature and found out if there was any basis for this yes compensatory J eating uh after starting an exercise program is well recognized this explain why your friends might say to you hey I joined that gym I've SW my guts out for three months my weight hasn't changed it's just not working I don't know what's going on compensatory eating and so this is why we asked people not to undertake additional
exercise during the Counterpoint study and that's gone all the way through and so in the NHS National remission program people are not asked to undertake more exercise during the weight loss phase but let me emphasize a really important point during the weight maintenance phase we actively encourage people to increase what they do if people want to uh make their neck a bit broader because they might have lost weight there well they can do upper body weights that's very popular with men so the exercise message is not that you mustn't do it it's that we must
separate in time a matter of weight loss from increased physical activity that's a very important practical point and it's one that is so often missed out by exercise enthusiasts who are quite rightly enthusiastic about exercise but these young trainers think that everybody would respond to exercise exercises they do as a ritual activity and not actually look at literature and realize that people haven't who haven't done it before will increase what they eat when they start an exercise program there's a lot in that I guess one of the things that my head keeps going back to
is the ideology of type 2 diabetes and the the insulin resistance in muscle tissue and uh I appreciate that you said there that there wasn't a lot of muscle mass lost during the the um weight loss intervention but just to kind of maybe push back a tiny bit I'm not sure if if the average person in the general public with poor metabolic Health has a lot of a lot of muscle mass in the first place at Baseline so you know they're probably already under muscled and I guess my my point here is um not to
question what you're saying about appetite I hear that I wonder if over the 2E and 5 years even if it's outside of the weight loss intervention I wonder if people have very specific resistance training in place that they might have there might be a a higher rate of remission um by by improving someone's ability to to kind of manage blood glucose by having this this greater glucose sink so to speak yes absolutely I'm completely on on board with that um and indeed exercise and specifically walking was actively encouraged was measured was mentioned at every follow-up
visit but there's a further ASP we haven't touched on and this is illustrated by what happened when we measured the effect of this exercise device so we used accelerometers accurate triaxial accelerometers fitted on the upper arm uh to measure uh physical activity um during the whole of the direct randomized trial and what we found was our well- meaning advice to increase more was met with reports of doing more exercise the objective measurement from the accelerometer showed absolutely no change now you might be very disappointed in that and you think well maybe they weren't to be
good at giving the advice but in fact the further factor I mentioned was that people who develop type 2 diabetes tend to do less physical activity than the rest of the population they tend to like activity less whether this is a biological feature or it's merely an additional factor that makes the diabetes more lightly we don't know but J I agree entirely with uh the point you made but it has to be set in perspective and with regard to these people who don't have enormous amounts of muscle well in fact large people have very large
muscles um and the muscle that a person has reflects their everyday activity it's whatever they need to do what they do and these people need need less to move around in exactly the same way as it did before you might say the final Arbiter is well how do they feel the quality of life improved in direct and that remains so in fact throughout uh the five years of the study so the biggest barrier to to curbing type 2 diabetes and getting more people into remission would seemingly be adherence to dietary restriction and you've mentioned a
few times that losing weight and keeping it off it's a hard business particularly in the environment that we're we're in now this obesogenic environment that in many ways is kind of set up for people to fail so if we Zoom right out here Roy what needs to be addressed at a society level to help more people stay below their personal fat threshold and really squeeze type 2 diabetes out of our communities we need a rational approach to a matter of food provision now this question becomes political because inevitably uh this involves legislation we don't bring
about societal change without legislation by large so smoking business would not have happened where not to be outlawed in uh indoor communal places that actually produces a sea change the matter of wearing seat belts we knew that it saved lives but it was hardly done until the seat law seat belt law was introduced same with motorbike helmets dramatic reduction in mortality but no one notices that their motorcycling brother or son is not killed they were wearing a helmet so it it passes under the radar with food here we got a highly toxic substance in excess
that is one of the few toxic substances that's not regulated talk about any other toxin yes we have sensible legislation mention food and I'm afraid politicians are swayed by arguments of oh we don't want a nanny State we can't legislate about food everybody needs it well that might be true but uh we can put reasonable limits on so what are those reasonable limits well the first thing was a small step in the right direction of putting attacks on sugar sweet and beverages that forced a reformulation it caused Horror in the soft drinks industry who said
well we're going to have redundancies and our profits are going to go down and shareholders will suffer it was done what happened to employment no change what happened to the profits and we can see now the published profits continue to rise in a straight line so that argument was in true and exactly the same arguments are being made about restrictions upon two things the amount of added sugar in uh prepared foods fast foods and ready meals and total quantity served now that's a more difficult uh item to deal with but those are changes that can
be made to legislation along with the Restriction of fast food outlets near schools certainly in the UK we have a terrible problem with childhood obesity so there are sensible moves that can be made but it requires the general population to be demanding of politicians so we get above the silly part of political business and arguments about many states to actually achieve a safe envir enironment for our children and for the future of mankind are there still questions that remain unanswered that you have from a scientific point of view or do we understand enough now about
type 2 diabetes that you could retire you could maybe move into politics Roy um it's not a case of of of not knowing enough it's just a case of not doing what we know um is is that where we are right now or do we need more studies on on type two diabetes to get a better kind of handle on it a great question uh I think we're in possession of all the knowledge we need to make sensible changes to our environment legislative changes included but do we know everything no we don't and we would
benefit by learning more uh exactly what is it that causes the insulin producing cell to start curling up its toes and not performing well we don't really understand that and it's still a relatively under researched area because the scientists investigating the beta Cel had been focused on glucose because that's so easy to use in the lab to produce stressed beta cell but there been relatively few studies apart from the ones that informed the twin cital hypothesis uh researching the effect of fat on the beta cell those very early studies Illustrated the point I made about
some people not being sensitive to Fat well their beta cells just don't care if there's fat around whereas a beta cells from sensitive people they go under we don't understand the processes we don't understand why so yes there are scientific questions that remain open but that's no excuse for not acting now with regards to the wider population health and for individuals to be advised by doctors for their best metabolic health is it still a hypothesis the the twin cycle hypothesis or would you say that it's been proven and I guess is a model it's one
of these curious things the term hypothesis always sticks uh you you might say uh it could almost be described as a theor but we don't we don't use that terminology so it's a hypothesis that's been proven now we know from neonian mechanics and Einstein's Revelations and then Revelations about subatomic particles that proven hypotheses can be adjusted into the future but hey each of them is largely right and so yes the major advances were made will remain true so yes the twin cital hypothesis I think will remain TCH uh the personal fat threshold will remain um
PFT uh these are hypotheses the second one is more of a concept um the terminology is quaint perhaps but at least it illustrates progress well Roy this has been incredible um your work is offering a lot of Hope to to a lot of people I think you've you know answered a lot of questions that no doubt May many of the the listeners have and I have a quote here from one of your reviews um it's actually the the opening kind of couple of sentences type 2 diabetes was once thought to be irreversible and Progressive but
a series of clinical studies over the past 12 years most of which if not all have been your studies have clarified the mechanisms that cause the disease we now know that processes that cause type 2 diabetes can be returned to normal functioning by restriction of food energy to achieve weight loss of around 15 kg so um I just wanted to emphasize you know how grateful we are for for all of the work that you're doing and have done and and everything that you've Unearthed about type 2 diabetes it really does offer a lot of Hope
for a lot of people thank you so much for joining us today and hopefully we can connect again some point in the future and uh perhaps continue the conversation in a part two thank you for the opportunity of communicating this exciting science s there you have it friends I hope you enjoyed this episode if you did and want to stay up to date with future episodes be sure to hit that subscribe button on YouTube and follow on Apple or Spotify finally thank you for showing up and the effort that you're making to take control of
your health I look forward to hanging out with you again in the next episode
Related Videos

1:49:54
Is Canola Oil Bad for You | Gil Carvalho |...
The Proof with Simon Hill
9,503 views
2:16:03
Longevity & Health: Exploring Seventh-day ...
The Proof with Simon Hill
32,203 views

2:26:38
Assessing Your Risk of Cardiovascular Dise...
The Proof with Simon Hill
62,310 views

1:05:57
A1C, INSULIN & the Damn RANDLE CYCLE with ...
KenDBerryMD
140,472 views

44:43
Dietary Fats: What You Need to Know for Be...
The Proof with Simon Hill
20,890 views

20:13
Professor Roy Taylor - What predicts drug-...
Public Health Collaboration
13,674 views
2:06:01
Is Fructose Driving Metabolic Disease? | D...
The Proof with Simon Hill
52,874 views
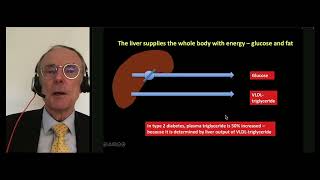
59:15
Long-Term Remission of Type 2 Diabetes Is ...
Ogden Surgical-Medical Society
33,386 views

1:36:56
Saturated fats, Sugar and Metabolic Health...
The Proof with Simon Hill
45,000 views

2:48:54
Maximizing Muscle Gain and Fat Loss: Evide...
The Proof with Simon Hill
58,748 views

1:39:38
Saturated Fat Misconceptions: Separating F...
The Proof with Simon Hill
46,130 views

1:49:16
Diet Trends & How It Affects Your Health (...
The Proof with Simon Hill
16,287 views

55:32
Why Anti-Diabetic Drugs Usually Make Thing...
Insulin IQ
133,383 views

1:56:58
Protein Amount, Quality and Timing - with ...
The Proof with Simon Hill
205,752 views

44:43
Reversing Type 2 Diabetes | Jason Fung
Jason Fung
1,056,000 views

3:35:33
Eating for Cardiovascular, Metabolic, and ...
The Proof with Simon Hill
47,652 views

1:17:18
How to Avoid Insulin Resistance and Why it...
Levels
499,513 views

1:11:11
The SUGAR Expert: Everything You Need To K...
Jay Shetty Podcast
3,149,964 views

14:51
EASD2021 Can you reverse type 2 diabetes?
European Association for the Study of Diabetes
14,827 views

1:12:45
Ben Bikman, PhD | Reversing Insulin Resist...
Metabolic Health Summit
253,797 views