Prefrontal Cortex
53.56k views4830 WordsCopy TextShare

Sense of Mind
The prefrontal cortex (PFC) allows us to engage in what scientists call “cognitive control” (also kn...
Video Transcript:
the prefrontal cortex or pfc allows us to engage in cognitive control also called executive functions which includes following instructions inhibiting impulses and regulating emotions outside of cognitive control the prefrontal cortex is involved in our sense of self while we will explore this aspect as well prefrontal cortical function is most closely associated with cognitive control so that will be the main focus of this video now here's david better a neuroscientist who studies cognitive control on why the pfc is so crucial for this set of functions it's well suited in a number of ways one is it's
a major hub of information from other sensory and emotional and memory systems that can provide information that could be used for monitoring your behavior and for controlling what you're going to do but really in terms of its being at the center of a control network both its inputs and its outputs are very hub-like connected to a lot of other areas each executive function is made possible by different combinations of subregions within the prefrontal cortex along with areas of the parietal cortex and subcortical regions especially the basal ganglia it is these networks that actually carry out
cognitive control different researchers use different demarcations to say what is and isn't the pfc in this video i'll be following the definition of neurologist leslie fellowes she states in a review that the pfc is the region anterior that is in front of the pre-central sulcus by the way i'm andrew cooper sansone and this is sense of mind this channel is all about helping you to understand your brain by looking at the most up-to-date and reliable science please like this video and subscribe to this channel if you get anything out of it also consider signing up
for the free newsletter by going to senseofmindshow.com newsletter let's get back to the pfc starting with the dorsal prefrontal cortex the dorsal prefrontal cortex which is the top half is crucial for certain executive functions including your ability to hold and attend to information respond to stimuli correct errors made during a task and motivation to do anything at all as just noted the functional theme of the prefrontal cortex as a whole is executive function also known as cognitive control which is in the words of the neuroscientist david better who we met earlier quote an elaborate class
of mechanisms devoted to generating plans keeping track of them and influencing a cascade of brain states that can link our goals with the correct actions cognitive control processes live in the murky space between knowledge and action influencing the translation from the first to the second while not being either one with that definition we can very roughly divide cognitive control into two categories emotional also called hot cognitive control or non-emotional or cold cognitive control now as an approximation the dorsal pfc contributes more to the cold variety whereas the ventral pfc contributes to the hotter emotional variety
now why is that so the subcortical brain structures those that are ventral to the cortex include the amygdala hypothalamus hippocampus striatum and nucleus accumbens these are all involved in the visceral experience of emotional feelings and the production of raw pleasure and pain now closer to this underside of the brain is the ventral prefrontal cortex compared to the dorsal half so it makes direct or indirect connections with many of these subcortical structures and can modulate their activity now the dorsal prefrontal cortex on the other hand is embedded in networks on the really in the cortex that
are more involved in sort of the higher cognitions we'll start with the dorsal medial prefrontal cortex one component of cognitive control is motivation which we can define as the willingness to do some kind of task patients with dorsal pfc damage mainly those with damage to the medial regions those near the midline of the brain especially the anterior cingulate cortex or acc often develop deficits of motivation at the most extreme end is a kinetic mutism where patients barely move speak or do anything on their own volition it's not that they can't move they simply lack the
will even when they can be motivated to do something so for example if someone like a doctor strongly urges them to do it they're unlikely to spring into action and they also show dampened emotional reactions now a less extreme condition is a bullia or a lack of motivation combined with some degree of slow thinking and slow movement on the other hand the mildest motivation deficit is apathy people with clinical apathy tend to do fewer things and engage in fewer tasks than most people what causes motivation deficits in dmpfc patients motivation requires the coordination of multiple
brain regions only some of which are in the pfc like the anterior cingulate cortex and the dorsal medial prefrontal cortex it involves a cost-benefit analysis in which we weigh the effort the cost required for a task and compare that against the probable outcomes but the first part of that equation the weighing of the cost of effort required to complete the task may be accomplished by the anterior cingulate cortex or acc the acc is all about prediction error signaling which david better once again explains is anything that differs from what whether it's good or bad it's
just this is something different than expected whether it's the response you made or the outcome or anything that happened at that point in time so acc is monitoring effectively the mismatch between the outcomes and the expectations in contrast the valuation of benefits involves the subcortical dopamine system if you want to learn more about dopamine check out my videos about it the medial prefrontal cortex refers to the area of the pfc nearest to the midline of the brain which separates one hemisphere from the other this region is robustly activated whenever you think about yourself as scientists
have shown with fmri now taylor guthrie a neuroscience phd student and creator of the youtube channel the cellular republic told me in an interview it's actually one of the most robust and reliable signals uh in any mri experiment across all of these different domains across detention across memory research whatever you can find in one subject you put them in a scanner you tell them to think about themselves same part of the brain lights up every single time and it's this medial portion of the frontal cortex guthrie has a particularly enlightening lecture on the neuroscience of
the self where he details some of the experimental evidence indicating which brain regions are involved for example in experiments where subjects are asked to consider whether a certain word accurately describes themselves or if it's better describes a another person it's the medial prefrontal cortex that activates more vigorously when the word describes yourself rather than another person guthrie explains this medial prefrontal cortex was really heavily active for the self-condition and wasn't active for any of the other two and at the level of the activity of the medial prefrontal cortex so if frontal if that medial prefrontal
cortex was really active while they were considering that word they remembered that word later if you're interested in learning more about the role of the pfc in self identity and motivation check out the interviews i've done with taylor as well as david better now let's move up and out of the midline and fan out to the dorso lateral pfc the dorsal lateral prefrontal cortex or dlpfc located toward the left and right edges of the pfc is required for tests of fluid intelligence that is the ability to reason flexibly in order to solve problems patients with
damage to the dlpfc often have trouble stopping or switching between tasks because they're likely to perseverate now perseveration is when you keep doing something even though the situation no longer calls for it for example if you ask someone with dlpfc damage to draw a picture of a clock but you tell them to stop numbering when they get to eight o'clock they are likely to just keep numbering it's not that they're rebellious or don't understand your request it's just that dlpfc patients have difficulty exerting the cognitive control necessary to switch tasks interestingly the dorsolateral prefrontal cortex
of the left and right hemispheres appear to have slightly different roles in cognition so the left dlpfc is involved in verbal reasoning while the right dlpfc is more important for certain kinds of visual reasoning this makes sense because many of the structures involved in language processing are on the left side of the brain as gregory hickok a language neuroscientist noted in an interview with me the language equals left hemisphere dogma is old and entrenched one of the reasons why you know it's so popular is it's partly true so if you have left hemisphere damage like
from a stroke most people if you have damage in the right you know the correct part of the brain that where language is involved you're going to end up with something called aphasia which is a disorder of the speech and language with right hemisphere damage language problems are not particularly common so there is pretty strong evidence for a left dominance for language however it turns out that the ability to produce speech is much more left dominant than the ability to comprehend it um and so that the i what we've been promoting is the idea that
the asymmetry or left dominance of language is not it's not uniform across all language functions that it's more a production thing and less a comprehension thing particularly the early stages of perceiving speech sounds seems to be quite bilateral when patients with damage only to the left dlpfc are asked to think of as many words that fit into a given category as they can in a short period of time they produce fewer words overall and make more categorization errors compared to healthy controls or even to write dlpfc patients those patients on the other hand show a
similar pattern but with visually demanding tasks for example if they're asked to draw as many shapes as possible that all conform to a simple set of rules regarding how many lines the shapes can have and similar constraints the right dlpfc patients are often unable to follow those rules and end up drawing fewer shapes overall it's not entirely clear why the right side shows the visual deficit now why do dlpfc patients show these deficits one reason for these deficits may have to do with the dlpfc's role in working memory working memory as defined by rebir and
trinell 2019 is quote the ability to temporarily maintain and manipulate information of different modalities in other words we might colloquially refer to it as the front of your mind or the forefront of your mind patients with dlpfc damage perform really poorly on tests of working memory in monkeys individual neurons in the dlpfc have been shown to activate in response to a stimulus indicating that the monkey will need to perform a certain task now intriguingly those same cells remain active during a short delay in which the stimulus isn't shown perhaps indicating that some representation is still
active in the monkey's working memory another function of the dlpfc that helps explain the cognitive deficits resulting from damage is that of abstract rule representation a very important feature of the frontal cortex is that it houses the supplementary motor cortex as well as the pre-motor and motor cortices that essentially plan select and execute movements broadly the supplementary motor area or sma and the pre-motor cortex sends signals to the motor cortex which initiate actions and command the spinal cord to execute them as you can see these motor regions are the most caudal that is closest to
the tail of the animal in the frontal cortex many researchers consider the pre-motor cortex and sma to be just outside the border of the pfc okay so the opposite of caudal is rostral which means closer to the head or nose of the animal interestingly as described by david better in his book on task if you start at the pre-motor cortex and move rostrally toward the front the function of the cortex becomes increasingly abstract another way of saying this is that more rostral regions of prefrontal cortex represent deeper rule trees for example you probably have seen
a sign at a store that says no shirt no shoes no service which is a very concrete instruction a shallow rule tree now let's say that this particular store has a casual friday rule where you don't have to wear shoes and if you're a male you don't have to wear a shirt either so we've just made this rule tree corresponding to the store's dress code much deeper not only must you remember no shoes no shirt no service you must now remember that that rule only applies on saturday through thursday but also that on fridays an
alternative rule applies and depending on your gender an additional friday rule may also apply patients with damage to more rostral regions show difficulty with deep but not shallow rule trees those with caudal damage show difficulty with both since you can't build a deep tree without shallow ones as foundation now interestingly the region that houses the very deepest rule tree isn't the most rostral end but the mid dorso lateral prefrontal cortex and as david batter notes compared to all other animals that have prefrontal cortices the region that is most expanded in human brains is the mid
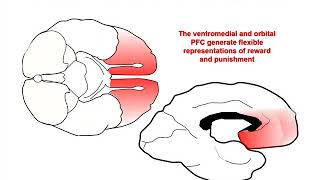
dorsal lateral prefrontal cortex so part of what makes our species unique is our ability to represent highly abstract rules the ventral medial prefrontal cortex or vmpfc is involved in social and emotional aspects of executive function as well as certain types of decision making and probabilistic reasoning this brain region is extremely important in ethical behavior medial means near the midline so ventral medial means the underside near the midline for our purposes the ventral medial prefrontal cortex includes areas of what this 3d model refers to as the orbital frontal cortex like the vm pfc the orbital frontal
cortex is often considered a subdivision of the ventral pfc we noted earlier that the ventral medial pfc is involved in social and emotional aspects of executive function and the anatomy of this region gives us the first inkling as to why the vmpfc connects to a number of subcortical brain regions that are involved in emotions especially the visceral feelings associated with emotion for example the vmpfc makes important connections with the ventral striatum a key structure in the brain's dopamine system which is important for motivation and pleasure it also connects with the amygdala a brain region that
is thought to be the brain's alarm system of sorts because it triggers the fight-or-flight response to stress as we noted the vmpfc is important for the emotional or hot aspects of cognitive control still there's some wiggle room the ventral medial prefrontal cortex isn't exclusively about emotional executive function but it also includes some of the more cognitive aspects that is partly due to a fundamental fact about the brain the line between cognition and emotion between reason and passion is blurred and ill-conceived both involve cortical and subcortical structures yet we can still say with a rough approximation
that those subcortical regions residing below the cortex are maybe more crucial for emotion now the vm pfc is connected to many subcortical structures it is also part of functional networks that include other cortical regions involved in perception and higher thinking this means that if you were to injure your vmpfc there would not be just one effect but many also given that this region likely contains billions of neurons and other cells each participating in various functional circuits the effect of the injury would depend on precisely where it was located within your vmpfc what happens if your
ventral medial pfc is damaged the most famous case of this kind of injury is a man known in the medical literature as evr evr had a tumor removed from his ventral medial pfc which caused damage to nearby brain tissue in the words of one of evr's neurologists antonio de macio and his collaborators evr's social conduct was profoundly affected by his brain injury over a brief period of time he entered disastrous business ventures one of which led to predictable bankruptcy and was divorced twice the second marriage which was to a prostitute only lasted six months he
has been unable to hold any paying job since the time of surgery and his plans for future activity are defective he now lives in a sheltered environment unable to support himself and his family now this table from rieber and trinell's 2019 article shows the characteristic outcomes of vmpfc damage and compares those to two widely cited checklists of psychopathy as well as the symptoms of something called acquired sociopathy several of these items seem to relate to decision-making including the inability to organize future activity and hold gainful employment and diminished ability to respond to punishment let's look
at two types of decisions and how they're affected in vm pfc patients throughout the following discussion however remember that the vmpfc circuit seems if it's damage seems not to affect iq movement perception or communication vmpfc circuit damage can cause impairments in the ability to reason probabilistically this is evident in the iowa gambling task or igt so imagine you're sitting at a table and there are four decks of cards in front of you your goal is to win as much money as possible by picking a total of 100 cards each one at a time choosing from
any of the four decks every card has a positive or negative dollar amount written on its opposite side which you add to your cumulative score however unknown to you the experimenters have stacked the decks two say a and b are losers and two are winners say c and d specifically if you were to pull all 100 cards from a and b the losers you would have some rounds where you won a large amount say 100 but more rounds where you lose a greater sum say 250 on average then you would lose money on these high
risk decks yet if you drew exclusively from the winning decks c and d you would have some rounds where you get zero dollars but you'd have more rounds where you win a modest positive sum say 50 bucks on average you would win money if you picked only from these low risk decks now as you can see here healthy people start out choosing from the high risk loser decks probably because they initially win big but by about 30 cards in they've switched over to the low risk winner decks having learned their lesson from losing huge sums
with the high risk decks vmpfc patients however keep trying the high risk decks well like healthy participants they initially picked the high risk loser decks and by the 30th trial they do wise up and switch to the low risk winner decks yet by about trial 50 they have partially reverted and now pick from the winning and losing decks with equal frequency which is not an optimal strategy you can imagine how this might translate to difficulties with risk assessment and decision making where the stock market and casinos would appear to be especially dangerous for people with
vm pfc damage now the second domain of decision making affected by vmpfc damage specifically damage to the orbital frontal cortex is that involved in reversal learning tasks okay so say you're faced with a task where you have to learn one set of rules and then once you learn it the experimenter suddenly changes it to a different set of rules without telling you depending on how complex and different the new rule set is it would take you a little while but you would be able to figure it out through trial and error now a vmpfc patient
on the other hand would tend to stick with the original rule set and may never learn the new one even if he knows there's a new one at play again you can imagine how this would severely impair decision-making in a complex modern world whose rate of technological and cultural change seems to be accelerating all the time now what causes these decision-making deficits it may have to do with the vmpfc's role in emotion but before we get to that i just want to ask you really quick to please like subscribe and consider signing up for the
e-newsletter list okay sorry for that interruption let's get back to the ventral medial prefrontal cortex and emotion rieber and trinell note that when most of us do the igt we show unconscious signs that we are learning the probabilistic reward and punishment contingencies that is before we can consciously articulate which decks are high or low risk we actually sweat a little bit more as we reach for the high-risk decks this is a bodily response triggered by the autonomic branch of our nervous system or ans in other words the ans has picked up on the probabilities before
the rest of the brain or at least before the conscious parts of the brain so patients with damage to bmpfc circuits tend to sweat less not only on the igt but in response to pornographic or violent images that would elicit a pretty strong response in most people rieber and tranel note that the vmpfc patients often show a dampening of emotional experience still it appears that not all emotions are dampened after vmpfc damage the mpfc patients may have a lower threshold for anger and frustration for example some researchers argue that parts of the vm pfc may
represent subjective value leslie k fellows notes that vmpfc activity increases as subjects consider more valuable stimuli and the strength of that activity predicts which options they will choose interestingly in addition to the decision-making deficits just noted vm pfc patients are also likely to show choices inconsistent with their own revealed preferences that implies that their ability to calculate or maintain a hierarchy of subjective value is somehow impaired another emotion relevant feature of the bmpfc is its relation to empathy as robert sapolsky explains in behave as children's bmpfc matures and begins to resemble that of an adult
their subjective experience of other people's pain changes so if you see someone you care about gets slapped in the face you'll probably have a subtle vicarious experience where you imagine what that slap felt like and importantly you will also consider how that slap made that person feel emotionally but children who still have developing vm pfcs are more likely to focus on the physical pain and think less about the emotions that the slap must have evoked in the victim sapolsky also explains that the vmpfc is important for reducing our reaction to emotional stimuli so if you
look at an angry or fearful face your amygdala probably activates but your vmpfc will turn down that amygdala activity so you don't freak out in a situation where that would be completely inappropriate but children with still developing bmpfcs on the other hand tend to have stronger emotional reactions to angry or fearful faces and as noted the vmpfc patients tend to have lower thresholds for anger now let's turn to how the vmpfc's role in emotion explains an unsettling result of bmpfc damage regarding ethical decision making according to rieber and trinell both vmpfc circuit patients and psychopaths
show an unusual adherence to strict cold calculating utilitarianism this may be because the hyper-rational dorsal prefrontal cortex takes more control over decision making in the absence of input from the vmpfc now the dictionary defines utilitarianism as quote the doctrine that an action is right insofar as it promotes happiness and the greatest happiness of the greatest number should be the guiding principle of conduct if that's a compelling moral principle to you you like most people may nevertheless get squeamish when it comes to following through on its logical implications for example imagine you're a civilian in a
war zone you're with a group of people hiding out from a nearby enemy soldiers who will kill everyone in your group if they find you if anyone makes so much as a peep it all ends tragically now picture that one in your group is a mother with a baby and it starts crying your choice is horrific you have to either smother and murder this baby to silence it or watch as an innocent group of fellow humans is murdered partly due to your inaction what do you do in that circumstance many people's utilitarianism goes out the
window we simply feel too much sympathy for the baby and the mother to end that innocent infant's life yet utilitarian logic would probably say that doing so is justified like psychopaths but unlike the rest of us bmpfc patients are likely to follow through with the calculus they would be more likely to smother the infant to save a greater number of innocent lives or at least they say they would now before you get too judgmental imagine that if the number of lives to be saved was say a hundred million rather than a few you might have
to be a moral monster not to take such an action because at least some maybe tens of millions of that hundred million would be innocent infants still that decision would haunt most of us because of the ruthless violence and horrible suffering we inflicted but vmpfc patients are often less sensitive to guilt than the rest of us and this can help explain that pattern because of their reduced autonomic responses they may not feel the pits in their stomachs corresponding to guilt quite as acutely as the rest of us limited evidence suggests that they may also be
less sensitive to feelings of regret and as a side note i've explained elsewhere that sensitivity to guilt helps predict a person's trustworthiness okay let's summarize on this tour of the prefrontal cortex we've seen that this region is extremely important for both hot and cold cognitive control as well as our sense of self cold cognitive control appears to be mainly the domain of the dorsal prefrontal cortex for example the dorsomedial region and the anterior cingulate cortex appear to play an important role in motivation by way of their role in analyzing the cost of effort of carrying
out a task the dorsolateral pfc on the other hand appears extremely important in following instructions rule trees and working memory and there may be some lateralization with the right side more important for visual reasoning and the left for verbal reasoning on the other hand the sense of self depends on the regions of the medial pfc including the dorsal and ventral areas in contrast pod cognitive control and cold cognitive control as well as cognitive control in social settings may be more a function of the ventral pfc especially the ventral medial prefrontal cortex lastly i want to
emphasize that while i have divided the prefrontal cortex into ventral dorsal rostral caudal lateral and medial this is just a convenience in reality the pfc is continuous there are no separating lines from one sub-region to another and these sub-regions co-activate during many tasks also just to hammer this point a little more remember that the pfc does none of these things on its own without its associated networks in in general in the brain and the basal ganglia and parietal lobe in particular there would be no cognitive control if you're interested in learning more about pfc networks
in cognitive control check out the 2022 paper by vinod menon and marc despacito in the references in the caption as well as david better's 2020 book on task or the interview i did with david better about his book now thank you so much for watching this video if you got anything out of it please give it a like and maybe drop a comment and subscribe and also consider signing up for our weekly free video newsletter you can find that link in the captions or go to senseofmindshow.com newsletter now as always this channel is brought to
you by the diamond mind foundation this video was written and produced by me andrew cooper sansone thank you so much for watching i'll catch you next time [Music] you
Related Videos
18:48
Igniting Positive Emotions: The Prefrontal...
Sense of Mind
7,195 views

16:29
The Evolution of the Brain
Sense of Mind
135,775 views
2:32:38
Dr. Mark D'Esposito: How to Optimize Cogni...
Andrew Huberman
448,873 views
25:47
Prefrontal Cortex and ADHD
Dr. John Kruse
2,626 views

17:34
ADHD Is a Curse… Until You Learn This
ADHDVision
999,106 views

20:04
Neuroscientist Answers Emotion Questions |...
WIRED
2,087,011 views

16:08
How the Amygdala Works
Sense of Mind
42,508 views

25:16
Time, Music, and The Brain (The Social Bra...
Sense of Mind
725 views
25:21
The Neuroscience of Exhaustion: How to Sta...
Sense of Mind
24,301 views

14:09
Prefrontal Cortex (Matt Botvinick) | Lex F...
Lex Clips
10,246 views

17:54
Hippocampus and Memories
Psych Explained
116,324 views

11:58
The Evolution of the Cerebral Cortex: How ...
Sense of Mind
24,539 views

39:25
What Makes ADHD in Women Different
HealthyGamerGG
701,479 views

23:30
Addiction Neuroscience 101
The Science of Addiction
657,895 views
1:00:35
The Nuts and Bolts of Better Brains: Harne...
World Science Festival
1,599,255 views
32:16
The Neurobiology of Prefrontal Cortex and ...
Yale School Of Medicine
91,611 views
1:10:41
Decoding the Brain
World Science Festival
875,786 views
13:39
Why Teenagers Are Reckless...
Institute of Human Anatomy
251,062 views

24:42
The Limbic System - Motivation, Emotions, ...
Psych Explained
96,541 views
1:07:38
The Human Brain’s Greatest Invention: The ...
Sense of Mind
3,665 views