Special Senses | Semicircular Canals | Cristae Ampullaris | BPPV
483.65k views6440 WordsCopy TextShare

Ninja Nerd
Official Ninja Nerd Website: https://ninjanerd.org
Ninja Nerds!
During this lecture Professor Zach ...
Video Transcript:
I ninja nerds in this video we're and talk about the semicircular canals so again if you haven't already please go watch the anatomy of the inner ear watch the video on the cochlea watch the video on the vestibule and then now we're gonna talk about the semicircular canals these are really really important structures alright so let's go ahead and dig right in so over here we have a little crude diagram if you remember we've used this for the cochlea and the vestibule and stuff like that so if you remember this part over here this little
coiling like part we call that the cochlea alright we talked about that its role within the sound right the sound transduction from the sound waves then we talked about the vestibule and its components right via the macula within the utricle and the saccule and their response to linear acceleration in the horizontal horizontal and vertical axis and head tilting now we're gonna talk about these guys here which is going to be these guys right here these little half little circles called the semi circular canals there's actually three of them okay three of them and this is
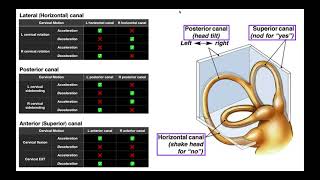
important to understand that because what's really cool about the semicircular canals is that they're oriented in such a way that they fulfill both the x axis the y axis and the z axis so any rotational acceleration they can pick it up in any angle which is I don't know I think that's so darn cool so what are the different semicircular canals so let's pretend that this is the right all right inner ear structure this guy is going to be pointing out towards your ear alright so it's in the inner ear and it's pointing out towards
the auricle this one right here is going to be called the horizontal or the lateral semicircular canal all right is the lateral semicircular canal then you're gonna have another one and this one is actually going to be coming up like this all right it's going to called the superior or the anterior semicircular canal so you have this one right here which is going to be the anterior semi circular canal they have one more which is going to be coming and the posterior part all right this is gonna be going backwards this way this is going
to be called the posterior semicircular canal all right now remember I told you that they're they're oriented in specific types of axes so let's take two different planes let's say I do a sagittal plane okay what does that mean I'm cutting right down here I'm cutting down the sagittal plane from the nose all the way to the occiput and I'm looking right here okay well let's imagine here that we have the left ear and the right ear okay what happens is is you have the anterior semicircular canal which we're gonna represent like this okay there's
the anterior and here's the anterior then over here in the back there's going to be another one called the posterior semicircular canal and then these one's going out to the side lateral alright these are going to be called your lateral semicircular canal and the significance of this is really cool in the sagittal plane you have different angles that these semicircular canals are oriented in so from the posterior semicircular canal to this actual sagittal plane is a total of 56 degrees so 56 degrees post here lis and laterally from the sagittal plane you'll have what's called
the posterior semicircular canal then from the anterior to the sagittal plane is approximately 41 degrees so then you're gonna have the anterior semicircular canal oriented 41 degrees and Theriault laterally and tarah laterally from the sagittal plane now here's the next thing if we look at a horizontal axis right so imagine here is going to be here's your nose your mouth right like this and then here is your eye right when you have this part here you're gonna have your other another canal the horizontal canal and imagine here we have from the nasal occipital line here
we have an angle in this actual lateral semicircular canal from the horizontal plane is approximately 25 degrees from the horizontal so the lateral semicircular canal is located within 25 degrees above the horizontal plane what why am I even mentioning these things the whole purpose is is that they're technically 90 degrees from one another and because of that that allows for them to be able to pick up rotations pick up the actual angular acceleration from any type of angle and direction that is what is so darn cool and interesting about this structures here ok so again
you have the lateral semicircular canal which is like 25 degrees above the horizontal then you're gonna have over here the posterior semicircular canal which is 56 degrees post here laterally from the sagittal plane the anterior semicircular canal which is 41 degrees and tear laterally from the sagittal plane and because of that they have 90 degree angles for one another that allows for them to be able to pick up information with respect to angular acceleration within three axes they can pick it up within the Y axis they can pick it up from the x axis and
they can pick up information from the z axis that is just I don't know why so darn cool that they can pick up angular acceleration and any type of axes all right so we talked enough about that that kind of stuff let's go to the next point the next thing that we need to do is is we have to kind of talk a little bit more about these semicircular canals remember how we did with the vestibule we had that like that little little kind of like flow here if we come down here again let's follow
that again so you have what's called the outer bony labyrinth and this is the one that's made up of perilymph right which is again if we go over it again it's gonna be what rich in sodium low and potassium this consists of this is the one that's actually called a semicircular canals this is the semicircular canals okay the outer bony labyrinth contains a special structure inside of it what is that special structure inside of it they call that the inner membrane as' labyrinth and the inter membranous labyrinth if you remember is consisting of in two
live high in potassium low in sodium the special structure which is contained within the semicircular canals is called the semi circular ducts last point was this last part here where we said there's a special detector okay this last part here is the special detector or that sensory epithelium so what is that special detector or that sensory epithelium well there's a certain part and we're going to explain and show it here in a second but there's a special detector or the sensory epithelium it's actually located in a specific point in the semicircular ducts called the ampulla
of the semicircular ducts that structure is called the cristae ampule eris okay so the crista ampule Arras is the special detector or the sensory epithelium it's found within the ampulla of the semicircular ducts which are consisting of in the lymph which is found inside of the outer bony labyrinth which is filled with perilymph called a semi circular canals okay so we know the difference semicircular canals we know that they're actual specific orientation with inside of the actual skull we know actually what is contained within the semicircular canals one more thing so now when we talk
about we talked about the utricle and we talked about the saccule with the macula responded to linear acceleration and the vertical and horizontal axis and the utricle played a rolled in head tilts right well this guy the semicircular canals they respond to rotational acceleration or angular acceleration okay so these guys play a role within rotational or we can say angular acceleration this is extremely important ok these guys this whole semicircular canal system plays a role with being able to maintain a special type of equilibrium ok our balance and they call that type of equilibrium they
call it dynamic equilibrium so it helps to be able to play a role of maintaining our dynamic equilibrium maintaining our balance our posture when we're in actually a rotational or type of kinetic activity so that covers that so we understand that he plays roles and rotational angular acceleration helped me maintain our dynamic equilibrium alright so now we actually can go ahead and use this and talk about it in a scenario because that's kind of the best way to learn this so what we're gonna do is is I'm gonna say let's actually pretend for a second
that I am actually moving my head to the right like this ok so I'm moving my head to the right what's gonna happen that's the best way to learn it's okay so let's say that I'm moving my head and I'm gonna represent it like this I'm rotating my head to the right so this is gonna be the right eye this is going to be the left eye ok so I'm rotating my head to the right when I rotate my head to the right I'm taking right now to semicircular canals alright and we could say that
it could be lateral we could say the posterior where you could say the anterior doesn't matter I'm just saying for right now I'm zooming in on one of the semicircular canals and looking inside of it ok because if you remember we had this semicircular canals here there's this little dilated region right there that dilated region right there is called the ampulla of a semicircular ducts so this is called the ambulance' my circular ducts right what I'm doing is I'm zooming in on that ampulla and looking inside of it ok so this is a part of
the actual duct system where the endolymph is flowing I'm zooming in on the ampulla that semicircular dock so we can look and see what's happening and we're looking at right and left so this is gonna be the right semicircular canal and this is going to be the left semicircular canal all right so I rotate my head to the right when I rotate my head to the right remember what was that fluid that's actually kind of circulating in this area right here what is that fluid call that's called into lymph all right when I rotate my
head to the right the fluid stays stationary for a second because of inertia okay so when I rotate my head to the right the fluid the indolent fluid that's present within the actual right semicircular canal over here is gonna stay stationary due to the inertia but the semicircular duct will continue the semicircular canal will continue to move so as that happens as this actual there's the rotation the fluid stays stationary but the semicircular canal still rotating so what happens is is this endolymph is going to kind of create like a little movement here that pushes
on this structure this Christiane pilaris like structure so again whenever we're actually rotating our head to the right due to the inertia the fluid the endolymph actually is going to stay like a stationary position and as the semicircular canals rotating the fluid rushes over this actual specialized detector and bends the actual entire Christiane Polaris you know there's a couple different structures we should talk about here son-of-a-gun all right so what is the couple of these structures you see is big red goopy jelly gelatinous like structure here they call this the cupula the ampule Airy cupula
because it's in the ampulla right the ampule of the semicircular docks now underneath the cupola and this cupola is just basically a gelatinous mucopolysaccharides like structure underneath it you're gonna have these hair cells okay these are our hair cells and remember that the hair cells have those stereocilia with the one big one called the kind of psyllium we'll look at that mechanism again beat that guy's into your head did you guys really remember that and there's supporting cells around that too then on top of that right underneath these hair cells you have these little eighth
fare and nerve terminals remember we have the ganglion there's a the vestibular ganglion here or another one we can call it the Scarpas gangly on Scarpas ganglion or the vestibular ganglion whatever you like the peripheral processes have these eighth faire nerve terminals that are actually going to be picking up information from these hair cells and then based upon that information it can get sent down the central process which goes to the central nervous system okay so looking at the ampulla within the semicircular ducts you have the cupola which is this big red gelatinous mucopolysaccharides structure
underneath that you have the hair cells with their stereocilia poking up into that cupola underneath the hair cells you have this types of affair and nerve terminals which is connected to Scarpas ganglion or the vestibular ganglion and the central process projecting to the central nervous system and then underneath the hair cells you might have some supporting cells so now whenever you go back to that thing we rotate our head to the right as we rotate our head to the right the semicircular canal will rotate because of the inertia the endolymph will flow will actually stay
still but as their semicircular canals rotating the endolymph will push on the cupula bending this structure so now it's going to bend this way if it bends this way okay there's different types of stereocilia within this area right so let's come let's go over here for a second and zoom back in on this so that we guys we get this down because I know we covered in stood in the vestibule I know we covered it with in the spiral organ of Corti but it's good to just do it again so let's say that whenever the
cupola bends right when the cupola bends let's see that the stereocilia beat towards the kind of psyllium okay so the stereocilia beat towards the kind of psyllium if this stereocilia be towards the kind of psyllium what does it do to the tip links stretches them as it stretches them what does it do to these actual channels opens the channels if the channels open who starts coming in calcium and potassium and again let's just keep it for the sake of it calcium and then we'll have here potassium as all of these cations start flooding into the
cell what happens to the inside of the cell it becomes extremely electro positive as it becomes electro positive what happens to the inside of the cell it starts becoming depolarized so then it'll produce what's called depolarization as that happens remember calcium ions are going to be accumulating over here and it's going to cause the synaptic proteins on these vesicles to fuse with the cell membrane as that happens and the vesicles fuse with the cell membrane what happens we can exocytosed these chemicals and when we exocytosed these chemicals guess what type of chemicals we release out
into this area when you release a special neurotransmitter called glutamate okay and glutamate will actually stimulate this actual affair nerve terminal and send action potentials down the peripheral process to the pseudo unipolar ganglion Scarpas ganglion again you can call the Scarpas ganglion or you can call the vestibular gang whatever you want then whenever it reaches the Bible this pseudo unipolar neuron it'll send information down the central processes to the central nervous system okay now this is whenever the stereocilia beat towards the kind of psyllium so the stereocilia is beating towards the kind of psyllium what
would happen if it was beating away from the kind of psyllium the tip links would relax the channels would close calcium potassium can't come in if calcium potassium can't come in it's not going to depolarize it'll actually hyperpolarize if it hyperpolarizes it won't stimulate the exocytosis of glutamate it won't stimulate action potentials okay so if we rotate to the right due to the inertia of the endolymph pushes the ampulla of cupula and let's say that it causes these actual stereocilia to beat towards the kind of psyllium if they beat towards the kind of psyllium what
is going to do these these nerve terminals here it's gonna stimulate it and it's gonna stimulate action potentials down the Scarpas gang like down the peripheral process to the pseudo unipolar neuron where the actual Scarpas ganglion is then it'll send these action potentials up through the central processes of this nerve into the central nervous system isn't that crazy okay so this one's gonna be stimulated alright this is gonna be stimulated let's come over here so now we're rotating to the right due to inertia the fluid stays kind of like stationary but the semicircular canals are
rotating so as the semicircular canals are rotating but the fluid has inertia what's gonna happen the endolymph is gonna flow in this direction now and if the endolymph flows away from this so here they call this ampulla fugal movement and they call this one over here ampule OH pedal movement so they call this ampule Oh fetal movement which is gonna be towards the cupula bending the cupula and then this one is going to be ampule oh fugle movement which is going to be moving away from the cupula so if it moves away from the cupula
let's say that it actually causes these guys to move like this so now it moves in the opposite direction okay if it does that what's gonna happen let's assume that we go back to this again we look at this but we take the opposite example here's another hairstyle here alright and we have this guy here this hair cell and what we're gonna do is we're gonna have the stereocilia beat away from the kind of sodium in this example as the stereocilia beat away from the kind of psyllium what's going to happen then is the calcium
or the potassium gonna start entering in no because those tip links are gonna be relaxed now and so now these can't get in if they can't get in what starts happening to the inside of a cell it doesn't become electro positive and actually kind of slightly hyperpolarizes if it hyperpolarizes what's that going to do then is there gonna be any release of the glutamate no there's gonna be no release of the glutamate if there's no release of the glutamate are you gonna be able to stimulate these efferent nerve terminals no so what's gonna happen to
the action potentials being sent down this actual neuron here it's gonna be yeah it's gonna be decreasing or pretty much no action potentials so we'll show it like this we'll do like a arrow here like a little positive here positive here showing that this is very little action potentials and with all of these significantly large amounts of action potentials so high action potentials here down a vestibular branch of the vestibular cochlear nerve and then very little action potentials coming down to this tip of the branch of the vestibulocochlear nerve on the left side okay do
you guys know what actual hole in the skull this moves through okay as these because you know this part here the Scarpas ganglion these processes will come out and become a part of the vestibular branch of the vestibular cochlear nerve cranial nerve 8 it'll actually run through a hole in the skull called B internal acoustic meatus IAC right it'll move through internal acoustic meatus or internal acoustic canal whatever you like I'm gonna put IAC internal acoustic canal alright so I can move through the internal acoustic meatus or the internal acoustic canal and then into the
central nervous system where it'll actually go to a specific point within the medulla okay so now this has been stimulated due to the rotation to the right what happened to other artists and then this will be inhibited okay now as that happens lots of action potentials coming from the right side very little action potentials coming from the left side once it does that it goes to a special area in the brain in the brain there's the special nuclei here let's kind of draw them like this there's a superior vestibular nuclei in inferior vestibular nuclei a
medial vestibular nuclei and a lateral vestibular nucleus so this whole thing is the vestibular nuclear complex so again up here you're gonna have the superior vestibular nucleus medial vestibular nucleus lateral vestibular nucleus and inferior precipitant nucleus we'll talk about this a little bit more than the vestibular pathway for right now the most important one is mainly the medial okay it's mainly the medial one so when these action potentials are coming down through these actual vestibular cochlear nerve it'll go to the vestibular nucleus but primarily the medial vestibular nucleus when it does that it'll stimulate this
one whereas this one is it actually gonna have any action potentials very little pretty much none right so this is actually going to be inhibited so this is gonna have a lot of action potential stimulating the medial vestibular nucleus this is going to have very little or pretty much no action potentials inhibiting the medial visibility nucleus what happens is is these medial vestibular nuclei cross this is crazy right so they're gonna cross when they do that they go to the contralateral sixth nerve nucleus what is the sixth nerve nucleus this is actually going to be
the abducens nerve nucleus right so that's the sixth cranial nerve nucleus now what's really cool about this is whenever this guy he stimulated right he's stimulated he's going to send these lots of action potentials lots of action potentials down this structure to the six there of nucleus so what do you think's gonna happen to the six star of nucleus they're gonna stimulate or inhibit it we have a lot of action potentials you should stimulate it if you stimulate this guy he's going to send these action potentials to the left eye what structure right here here's
your nose in the middle right here's your nose so this is the medial rectus and this is going to be the lateral rectus remember L six lateral rectus is supplied by the six cranial nerve so this guy is gonna send these actual efferent axons going to the lateral rectus if he does that what will he do to the lateral rectus on the left eye he'll stimulated okay so he's gonna stimulate the lateral rectus of the left eye now another thing that he'll do he also is very interesting he kind of acts as not only just
this point here we can go and stimulate hit the lateral rectus of that side but he can kind of act like an interneuron and come up here to the contralateral side and stimulate this nucleus this is crazy right what is this nucleus here called this is called the oculomotor nerve nucleus or the third nerve nucleus so again this is the right side this is the left side again think about this if there is simulation to the six nerve nucleus activating these action potentials to the left lateral rectus then it should also stimulate this pathway if
you stimulate this pathway there should be lots of action potentials to the third nerve nucleus on the right side where does the actor oculomotor nerve go what goes to many different muscles but the main one that we're focused on in this example is the medial rectus so now we're gonna stimulate the medial rectus why am I telling you guys this there's a really important reason whenever we rotate right in order to be when we wrote it we want to be able to keep our vision we want to be able to keep our gaze set on
whatever we're looking at so whenever we're rotating our head our eyes naturally deviate very fast to the opposite side so if I rotate my head to the right my left eye is gonna want to abduct my right eye is going to want to add docked so that I can keep my eyes fixed on whatever I was looking at even when I'm turning that's the important part of this actual vestibulo-ocular reflex so the semicircular canals are really really important for being able to maintain our dynamic equilibrium but also they're really important that whenever we're rotating we
want to be able to fix our gaze on to whatever we're looking at because think about this if your running is your image jumping up and down while you're running no it's kind of pretty much held stable be thankful that for your semicircular canals and your your actual macula within the utricle in the Sakura because they help us to be able to keep our gaze fixed on whatever we're looking at even when we're jumping up and down over rotating so that's one of the beautiful things about this so now rotated our head to the right
so far what do we know we activate the right semicircular canal send action potentials to the vestibular nucleus on the right side the medial of vestibular nucleus sends action potentials to the left six nerve nucleus stimulating him to stimulate the lateral rectus of the left side after he stimulates that guy he the six nerve nucleus also kind of acts as an inter neuron and since action potentials to the contralateral third nerve nucleus who goes and stimulates the right what medial rectus so if you think about it what's this I gonna be doing then this guy
he's gonna contract he's gonna cause medial rotation this guy's gonna contract he's gonna cause lateral rotation so even though my head is rotating to the right my eyes are deviating to the left very fast okay so I'm deviating to the right very fast now to look at this again what about this side what's happening over here why aren't the other ones contracting well look very little action potentials you're inhibiting the medial vestibular nucleus is there gonna be many action but that's what's going to the six nerve nucleus no not very many at all so is
he gonna be having a lot of action potentials going to the lateral rectus of the right I know so what would happen here he's gonna be inhibited if that's the case then is he gonna have a lot of action potentials crossing over to the contralateral side to go to the third nerve nucleus so if he's not gonna be sending very many action potentials up to the third nerve nucleus then he's not going to be sending a lot of action potentials out to the medial rectus so the medial rectus of the left eye will be inhibited
which will allow for our eyes to move in that way so I think that's just so darn cool but now what is this connection what is this connection between the six nerve I said it's kind of like an inter neuron it's kind of acting like but what is this connection here between the six nerve and the third nucleus special name for it so since this is on the right side they're gonna call this the medial longitudinal fasciculus but this is the right medial longitudinal fasciculus this right here this one right here is the medial longitudinal
fasciculus but for the left side okay this is an important structure it's helping us to be able to fix our gaze on whatever we're looking at keep our phobia fixed on whatever the image is even when we're rotating around but if you notice something really interesting whenever you're doing that whenever you're rotating your eyes be to the left very fast but then guess what they do afterwards they look that way well why do they look that way well our cerebral cortex is really good at being able to keep us oriented and protect us right so
what happens is we have a specific area in the brain it's called the frontal eyelid I promise you it's actually it's an actual structure it's called the frontal eyelid it's actually on the frontal lobe in front of the premotor cortex so it's called the frontal eyelid and this is gonna be that part of the cerebral cortex over here we'll have another part of the cerebral cortex and again this over here is going to be the frontal eyelid of the right side so this is a frontal eyelid and again this is the right one this is
the laughs one what happens is is once we move our head to the right like I said our eyes be to the left really fast but then afterwards they compensate and go back to the right again as we're rotating so what causes that okay the frontal eyelids send action potentials down whenever this happens to a spatial spatial nucleus within the pons okay there's a special special nucleus in the pons this little brown nucleus what is this nucleus here called this one this one right here is called B this one's got a heck of a name
the para median pontine reticular formation holy frak that's a lot but this is the name of these nuclei okay so right here these guys right here is called the para median pontine reticular formation whenever we rotate our head to the right our eyes be to the left but then the cerebral cortex from the frontal eyelid sends these action potentials down when they do that guess what these guys do they come over here and tell the six nerve nucleus that so before this guy was contracting right he was contracting well now we don't want him to
be contracting we want the eyes to be able to go back in the normal direction so what do you think it's gonna do this guy track it's going to inhibit this guy between inhibit the six nerve nucleus if it inhibits the six nerve nucleus what's going to happen to the action potentials going to the actual lateral rectus it's going to decrease as it decreases is it going to cause stimulation here anymore no it's actually going to inhibit it if that's the case well our eyes actually abductor on the left side no okay at the same
time if we inhibit this guy and we named the sixth nerve nucleus right here then what's gonna happen to the action potentials via the medial longitudinal fasciculus the right one that's going to decrease that means am I really gonna stimulate the third or of nucleus ten on the right side no I'm actually gonna inhibit it now and now very little action potentials will go to the medial rectus on the right side what does that mean that means it's not gonna be stimulated anymore it's gonna be inhibited if that's the case then what are the eyes
actually what gonna be to the left anymore no now they're gonna start beating to the right so now when that happens and this the opposite will occur over here so right it's going to come over here and hit this nerve nucleus but then what will it do to the other side it'll actually cause those guys to be stimulated right so now it'll stimulate this side and you get the point it'll cause what let's look rotate my head to the right one of my eyes do first they beat to the left right and what muscles contract
on the right eye the medial rectus will contract on the right eye the lateral rectus will contract on the left eye but then what happens cerebral cortex notices that compensates for it within the frontal eyelids the frontal frontal lobe sends action potentials down to the para median pontine reticular formation who then does what to the lateral rectus now the lateral rectus over here is going to be inhibited okay so now the lateral rectus over here will be inhibited so it won't be pulling this eye out any more then on top of that the medial rectus
on the other eye is going to be inhibited so it's not going to be ad ducting anymore but then the exact opposite will happen then the medial rectus on the left eye will contract and the lateral rectus on the right eye will contract and what will happen our eyes will go in the direction of where it was okay when with the direction that we were rotating that is called that actual beating in the opposite direction then it's actually called saccadic movement so beating in the opposite direction is called saccadic movement okay that right there that
beating of the left and then beating to the right they call this a vestibular nystagmus so they call this vestibular nystagmus and this is a normal thing this happens normally okay so the stimuli nag nystagmus occurs naturally whenever you rotate your head to the right activates the right semicircular duct inhibits the left semicircular duct goes up through the pathways that have severed the nucleus medial longitudinal fasciculus cause your eyes to be 2d left-right but then the cerebral cortex compensates and causes them to be to the right that is called the vestibular nystagmus don't get that
confused with other types of nystagmus what happens is there's one of the most common causes of vertigo vertigo is basically the the feeling or the sensation that you think that you're rotating and moving around right even so it's basically kind of like a perception of something without an actual stimulus how does this happen remember back in the video where we talked about the macula they have those ODA Konya those OD Konya those crystals sometimes they can actually get dislodged and when you dislodged they can actually get stuck in the semicircular canals most common out of
all three of these semicircular canals is the posterior semicircular canal that's the most common one but you can get some that are dislodged and get stuck within the lateral semicircular canals or the anterior semicircular canals why is it important whenever you have these Auto Konya within there sometimes due to certain types of situations these ODA Konya can agitate the ampulla or they of the actual semicircular ducts if it does that and undesirably stimulates the ampulla of the semicircular ducts what is it going to do it's gonna send action potentials to your central nervous system telling
you that you're rotating when you're really or not so why would we not want that because that can cause vertigo and vertigo if you know what happens with vertigo sometimes it can even initiate nausea and vomiting because of it's so severe what can we actually do about this because they'll produce a nystagmus so if someone has let's let's say for a second that someone has an OD Konya that gets stuck with inside of the post here semicircular canal they call this posterior semicircular canal B P P V now you're probably like what heck does BPPV
stands for it stands for benign paroxysmal positional vertigo this again is one of the most common causes of vertigo now how would you diagnose this you can actually do what's called a Dick's Hall Pike maneuver and we're not going to demonstrate it but basically what it does it helps to determine if someone has benign paroxysmal positional vertigo specifically though if they have post here canal prolonged benign paroxysmal positional vertigo what happens is when they do the Dix Hall Pike maneuver their eyes will actually do what's called a rotational nystagmus so they'll have their eyes while
I bounce around like this it's called a rotational nystagmus okay that would be telling someone oh they have them they have paroxysmal posterior semicircular canal benign paroxysmal positional vertigo okay you know what you can do about it you can do a special maneuver they call it the Epley maneuver and it basically helps to be able to move the o de koning out of the semicircular canals and back into the utricle all right what about over here what if some has it's stuck in the anterior semicircular canal that's called anterior semicircular canal benign paroxysmal positional vertigo
well if you do the Dix Hall Pike maneuver what will happen to their eyes in this case it'll actually go up and down what is that called it's called a vertical nystagmus so if their eyes be up-and-down that's called a vertical nystagmus and you can do another maneuver there's different types of maneuvers for this one you can use what's called the limpert the limb the limpert actual maneuver and that can help to be able to move the ODA Konya back into the utricle and there's one more one more this is actually gonna be lateral semicircular
canal benign paroxysmal positional vertigo and if you do the Dix Hall Pike maneuver what will happen to their eyes it'll actually beat side-to-side that's called horizontal nystagmus and you can do a type of test called the deep head hanging maneuver which I'll help to be able to move those ODA Konya back into the utricle iron engineers so we pretty much covered the semicircular canals and we covered the vestibulo-ocular reflex as well as benign paroxysmal positional vertigo I hope all of this made sense I truly do I hope you guys enjoyed it if you guys did
please I'm begging you hit that like button comment down in the comment section and you better subscribe alright alright engineers please go check out our Facebook Instagram and our patreon account alright engineers until next time [Music] you [Music]
Related Videos

28:20
Special Senses | Vestibule | Maculae: Utri...
Ninja Nerd
450,708 views

18:01
Vertigo (Different Types, Dix-Hallpike Man...
Dirty Medicine
332,555 views

6:14
Boost Your ENERGY with this 5-Minute Holid...
Sana Animam Fitness with Diane Bollen
1 view

16:43
Vestibulo-ocular reflex neuroanatomy
Sam Webster
6,256 views

17:18
Boost Your Bone Density with These 6 Life-...
Talking With Docs
481,257 views

41:08
Special Senses | Cochlea | Spiral Organ of...
Ninja Nerd
567,361 views

27:11
You're Probably Wrong About Rainbows
Veritasium
1,470,771 views
14:22
Semicircular Canals EXPLAINED | Structures...
Catalyst University
26,145 views

42:40
Special Senses | The Phototransduction Cas...
Ninja Nerd
747,036 views

1:37:34
The Groundbreaking Cancer Expert: (New Res...
The Diary Of A CEO
5,513,696 views

21:50
Special Senses | Inner Ear Anatomy
Ninja Nerd
615,523 views
9:07
Understanding the Causes of Vertigo
Zero To Finals
4,233,991 views

6:17
Home Eye Test! If you fail, see an EYE DOC...
Michael Chua, MD
3,841,371 views

1:30:56
The Exercise Neuroscientist: NEW RESEARCH,...
The Diary Of A CEO
7,941,565 views

28:24
Neurology | Vestibulocochlear Nerve | Cran...
Ninja Nerd
262,036 views

1:44:24
Temporal Bone Imaging (3): Inner Ear Malfo...
The Neuroradiologist
1,332 views

13:48
Vestibular Neuritis Recovery Story
Lindsey “Moonshine”
33,676 views

27:01
Special Senses | Photoreceptors | Rods and...
Ninja Nerd
261,350 views

18:41
Spinal Cord Regions + What Each Region Con...
Siebert Science
63,249 views

24:28
Vestibular apparatus (inner ear anatomy)
Sam Webster
53,954 views