Chronic Myeloid Leukemia (CML)
127.64k views8548 WordsCopy TextShare

Ninja Nerd
Official Ninja Nerd Website: https://ninjanerd.org
You can find the NOTES and ILLUSTRATIONS for this...
Video Transcript:
foreign what's up Ninja nerds in this video today we're going to be talking about chronic myeloid leukemia also known as CML if you guys like this video it makes sense it helps you please support us and one of the best and easiest ways that you guys can go about supporting us to continue to keep making these free videos for you guys enjoyment is by hitting that like button comment down in the comment section and please subscribe also you guys want some awesome notes and illustrations that I really think will help you guys to follow along
with me during this lecture go down the description box below there's a link to our website where we have some amazing notes and illustrations on our website go check that out but let's start talking about CML so with CML very sad unfortunate but very interesting type of disease and at this point in the lecture really what I want you guys to understand is that when we talk about now going into the chronic leukemias you guys should have already at this point watched the videos on acute myeloid and acute lymphocytic leukemia or in this case we
actually call them acute myelogen so acute lymphoblastically leukemia you guys should have watched those by now and it's really important that you guys do because I think the pathophysiology at this point is really important to understand because if you guys remember we have the hematopoiesis pathway and CML is just an abnormality or alteration within the hematopoiesis pathway that's really what it is and it all starts with this beautiful cell a pluripotent stem cell or a hemocytoplast which is the main stem cell located in the bone marrow that produces all of this Downstream cell lines which
is pretty cool so this is called the hemocyto blast and the hemocytoplast is the stem cell for all blood cells so what it'll do is it'll differentiate and it'll differentiate what's called myeloid stem cells which you guys should already know by now and then the lymphoid stem cells and then what we talked about in AML and all is that really there was a disease process there was something abnormal which was occurring in the next component of the cell line because what happens is myeloid stem cells they'll further differentiate when they differentiate in the presence of
a hormone called EPO TPO which is erythropoietin thrombopoietin or what's called Colony stimulating factors these will then differentiate into special specific cell lines like red blood cells the erythropoiesis platelets via thrombopoiesis or making something called Milo low blasts and if you guys remember in AML the disease process occurred where we'll write it down AML occurred where the myeloblasts continued to proliferate and proliferate and you made tons of mild lasts because it would proliferate proliferate but it would not be able to differentiate into these further Downstream cell lines so would not make functional white blood cells
now in patients who have CML the disease processing occur as high up where it kind of gets stuck in being able to replicate replicate replicate but not differentiate and this is where it's really interesting so what happens is it's not here and the AML process what's really weird in this process is that the myeloid stem cell goes haywire and it just literally replicates like bunnies and it produces a ton of myoblasts a ton of the next Downstream effect so we go promile we go to myoblast into what's called a pro myelocyte then we go into
what's called a Milo site then we go into what's called a meta myelocyte and then these eventually go to What's called band cells but they completely differentiate into what's called functional white blood cells called neutrophils so you have your neutrophils you have your eosinophils and you have your basophils and these are your granulocytes the problem here is that the myeloid stem cell just over proliferates and if it over proliferates this this thing is going to start going haywire and if it goes Haywire it's going to increase its proliferation and produce more myoblasts more Pro myocytes
more myocytes more metamildcytes and you make massive amounts of neutrophils massive amounts of eosinophils and massive amounts of basophils that's really interesting isn't it so at each one of these what's happening in really CML or chronic myelody leukemia is this the myeloid stem cell that's just crazy proliferating but it's differentiating into each step do you understand the difference AML it was going Miley stem cell to myoblast proliferate proliferate proliferate proliferate never differentiated CML goes here proliferate proliferate proliferate differentiate differentiate differentiate differentiate into specific granulocytes so you'll get massive amounts of functional white blood cells which
is really interesting so that's where the pathophysiology occurs in this particular disease we're not going to focus on the lymphoid cells Sims align because we'll talk about that in CLL but you know the lymph lymphoid stem cells and the same concept they'll go to become lymphoblasts and then the lymphoblast will then kind of further differentiate into T cells and into B cells or B lymphocytes and T lymphocytes but in this particular process the disease is occurring right here the myeloid stem cell line and it's just happily over proliferating and producing multiple increased numbers of all
of the myelid stem cell line and if you want to even a little extra sometimes for some reason it may also increase the production of platelets but it has no effect on the red blood cell line for some odd reason but that is the big thing that I want you guys to remember so now the next question that has to come into your mind is is what's the reason that's that's the interesting component right so we know that CML is an A myeloproliferative type of disease it's that myeloid stem cell just replicating replicating and differentiating
and making tons of these white blood cells and even some degree platelets why is it over proliferating and that's the interesting question one unlikely cause but it's something to think about is ionizing radiation this may produce some type of mutation if you will but I would say that this is less common so the reason why ionizing radiation may do this is it may potentially produce something called a mutation and if you cause a DNA mutation it may stimulate what's called oncogenes or proto-onco genes and it may inhibit your tumor suppressor genes and allow for these
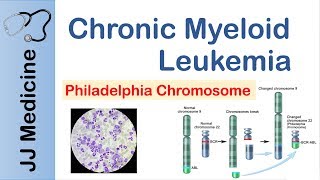
particular cellular replication to occur excessively without causing the cell to like stop dying so it'll have increased cell proliferation then they'll be decreased apoptosis so the cell won't die and then it'll just continue to keep dividing so that may be one reason the more likely reason and the thing that I need you I need you to remember in this lecture is likely genetic and that's one of the unfortunate problems with this disease is it's usually a genetic Association so the particular type of genetic association with this is It's seen and they called a chromosomal translocation
I'm actually going to remind you guys of this because you've seen it before so chromosomal trans location is a really interesting type of process it's where you're kind of like swapping genetic material between two chromosomes and the two chromosomes that this is occurring in is called chromosome 9. and chromosome 22. so here's 9 here's 22 and you're going to have a translocation between these in other words there's a gene let's make it red actually Rob who loves to film these videos he loves purple so we'll do purple for him this is going to be our
Gene right here so there's one gene okay we're going to call this one our able Gene and then over here we'll put this one we'll say that this is like our BCR Gene what I'm going to do is I'm going to swap some genetic material and when I swapped the genetic material between these two so let's show like a little swapping of genetic material between these two what I should get is I should get something called the Philadelphia chromosome and it really should be a combination of these two genes together I fuse these two uh
kind of genes right together and make them really abnormal so look now I have my Fusion Gene so my able Gene and my BCR Gene are right next to one another and actually fuse together so this is the result of the 922 translocation so the question that you have to ask is is why is this bad the BCR able Gene causes excessive replication and inhibits apoptosis the cell can divide divide divide and never die that's crazy those like vampire cells so now from this you'll have two particular effects here one is you'll have excessive cell
proliferation as we talked about above with the ionizing radiation and the other thing is that you will decrease apoptosis the way that the BCR able Gene does this is it activates as very specific enzyme that's involved in cellular peripheral proliferation and I actually do want you to remember this and the enzyme that it actually is kind of associated with was called a tyrosine kinase receptor so it's usually associated with What's called the tyrosine kinase receptor which is a very special enzyme so I need you pleased for the love of goodness don't forget that 922 translocation
causes the formation of the BCR able Gene which leads to increased cellular proliferation decrease apoptosis so the cell can divide and never die and the main reason it has the ability to do this is it stimulates the tyrosine kinase receptor this is 90 percent of the time associated with CML that's pretty high so the other disease just to quickly test your knowledge we said that this was seen with two diseases one CML what's the other one all so it's 90 of the time associated with CML 20 of the time associated with Alo I know the
math right doesn't make sense but that's the high the association relationship between these two now question then comes okay is it's getting stuck where again just so we can remind ourselves because what's interesting about CMLS is weird in comparison to AML and all and CLL in that it has three it's a triphasic type of appearance so we said here we have What's called the myeloid stem cell coming from the hemocytoplast goes into what's called a myeloblast a pro myelocyte a myelocyte a metamilocyte and then it goes and makes all of our granulocytes we said that
really what's happening is you're starting from this puppy here and you're just shunting these into this pathway making lots of these making lots of these lots of these in the initial stages what we call the three there's a three phase response there's a chronic phase an accelerated phase and a blast phase in The Chronic phase which is where 80 to 85 percent of patients usually live you're actually accelerating this pathway and making tons of neutrophils tons of eosinophils and tons of basophils but what happens is this only lasts for a certain amount of time and
as you continue to keep proliferating what ends up happening and this is what's weird in the beginning it's due to the 922. over time over time as you continue to keep replicating and replicating and replicating with every replication cycle becomes more mutations with more mutations comes more abnormalities so what I need you to remember is as you continue this pathway you'll have increased replication right but lots of replication that's occurring during this phase but the thing that I need you to associate this with lots of replication comes increasing mutations and with increasing mutations you decrease
differentiation you decrease the differentiation of the myelo stem cells so now what happens is is you start trying to push these into this pathway but because it goes mild blast Pro myocyte myocyte it may get stuck here stuck here or stuck here and that's over time so this is something that you see with time and as the patient starts transitioning into what's called The Accelerated phase or the blast phase they have less of these functional neutrophils eosinophils and basophils and more of the pro myocytes myocytes metamildcites less functional types of white blood cells and that's
important and that's what we have to talk about next all right so the next component here in this lecture is talking about okay we've we've made tons of leukocytes right we've made tons of neutrophils eosinophils baseballs and they're actually pretty functional we've just made a lot of them and what was the reason why we made a lot of them again is because there was a mutation it could have been due to ionizing radiation or it could have been a mutation due to a fusion protein the BCR able Gene that was formed which was the 922
translocation caused it to cause lots of tyrosine kinase receptor activity causing excessive cellulation causing the cells not to die because it's inhibiting apoptosis and because of that these cells can live forever and that's one of the downsides and that over time as you can continue to keep replicating replicating with each replication cycle you develop DNA mutations those mutations can then cause them to stop being able to differentiate and we'll go through this progression but one of the big things to realize is that an acute leukemia versus chronic leukemia acute leukemia a lot of these problems
develop rapidly so their cells actually do divide pretty rapidly in chronic it's more of a slow Progressive process so they do divide but the problem with them is that they divide and they don't die and so that's where the downside comes but it's Progressive over time over time over time and then it can potentially get worse so what's the effects of this let's talk about the triphasic response of CML there's three phases chronic phase accelerated phase and blast phase in The Chronic phase which is where to be honest with you 80 to 85 percent of
people usually present these oftentimes have no symptoms I'm not even kidding sometimes there's no specific symptoms but if they do have symptoms it's very very vague what are those symptoms okay we know one of the problems here is that that myeloid stem cell here is that myeloid stem cell it is just proliferating and producing tons of these neutrophils eosinophils and basophils right so one of the downstream effects that you'll see from this is if you were to get a CBC of the patient you would have a massive leukocytosis and the interesting thing is that this
would be of all cell lines and that's what's weird in this one and but it's actually very helpful is that you will have a lot of neutrophils which is relatively common but what you don't often see is a lot of basophils there's not many diseases that will pump your basophils up a lot and I really think that that's worth remembering so please don't forget that it will pump up your eosinophils as well now that's one thing is that you may find this and they may have strikingly like high uh white white cell counts on their
actual CBC so that's one thing that you could see but I think the base affiliate is really really critical but when you have these lots of leukocytes what they may do is two particular things one is that they can actually go and deposit into the spleen and when they deposit into the spleen the downstream effects of depositing into the spleen is that it caused the spleen to just get a little bit bigger and this can cause something called splenomegaly so you may see something called split Omega and to be honest with you this is actually
one of the more common things that you may see that cause these vague features is that if you have an enlarged spleen what's the spleen right next to your stomach and so the spleen gets bigger it's taking a lot of space and pushing on the stomach your stomach is supposed to get food in there if you can't get food in there because it's actually being compressed you end up with nauseous you end up maybe even vomiting you end up with not being I feel always full or you have a poor appetite so those are things
to consider so watch out for features of like nausea vomiting maybe anorexia or a poor appetite and a sense of like abdominal fullness these are really really kind of key features that you can see associated with splenomegaly and this actually tends to be one of the more common features that you see in the mild cases of this disease now two things can actually happen with this one now when you have this these white cells they can go to the actual spleen and it can cause the enlargement of the spleen but it's not just because of
them depositing into the spleen it can cause the enlargement of the spleen by two particular factors one of the reasons that the spleen enlarges is deposition so the deposition of the actual white blood cells but the second reason that the actual spleen enlarges is because some of these leukocytes cause the spleen to gain the capacity to start producing blood cells like wait that's that's hematopoiesis but it's not from the bone marrow so we call that extra medullary hematopoiesis so we call it extra medullary hamatopoiesis so that's what I really want you to remember is that
the reason why the spleen gets bigger is a two-fold reason one is because it deposits the leukocytes into the spleen causing it to get bigger but other is that the spleen gains the capacity to produce blood cells to help out the bone marrow and this is called extra medullary hematopoiesis okay the other thing that may potentially be there and it's very mild is that the leukocytes May release a lot of cytokines like interleukin-1 tumor necrotic Factor Alpha things to this effect that may trigger these low-grade fevers it may trigger some like fevers and some night
sweats but these are like mild constitutional symptoms okay fevers and night sweats so that may be something else that you can potentially see but I really think that splenomegaly is key the leukocytosis with the basophils are pretty key and you may see some fevers and night sweats the other thing is that it does affect the platelets it has no effect on the red blood cell line so what I want you to remember is that there's no for some arteries no effect on red blood cells in this phase because it doesn't actually cause them to over
you would think oh if the mileage stem cells are responsible for making all blood cells so red blood cells should go up it's weird there's no effect on them but there can be an increase in the number of platelets and so because of that you do want to watch out for something called thrombocytosis which may only be seen from getting a CBC you might not see any of the potential features of thrombocytosis so these are the big things that I really want you to remember about The Chronic phase in The Chronic phase the primary thing
that you have to remember is most people spend most of their life into this phase they usually present asymptomatic if they do present with symptoms most common It's associated with splenomegaly maybe some constitutional symptoms and if you don't see these constitutional symptoms or splenomegaly oftentimes it's just something that you pick up from routine blood work finding a markedly high white count on their CBC and a thrombocytosis and again to go back to the pathophys just to make a little note of this with that pathophiz what type of blast cells so you're producing a lot of
blast cells and I mean you're producing a lot of white blood cells one of the big things is that in this phase The Chronic phase the blast cells are low they are in the lower amount we say less than 10 percent whereas all the other ones all your granulocytes the relatively mature ones these are the ones that are in high amounts okay lots of granulocytes very little blast cells but now guess what we go to the next phase in this next phase we got the accelerated phase in the accelerated phase what has now happened is
you started this all off with the the trigger the trigger was likely a 9 22 translocation and that was secondary to What's called the BCR able Gene and what that did is that caused two effects one is it increased the cell proliferation and the second thing is that decreased apoptosis right we we know that now one of the things here is that because of this lots of cell proliferation and decreased apoptosis it really increased the number of granulocytes right it really increased the number of granulocytes but here's the thing if along the way I add
more mutations into the mix so now what I'm going to do is I'm going to represent this with like a red arrow I add more mutations I'm going to put mutation here maybe from them having excessive amounts of replication they develop a mutation in the p53 gene or a rash Gene whatever it may be and now they gain the capacity to start increasing more blast cells so then they increase their granulocyte amount but they also start increasing their blast cells and it was less than 10 percent in The Chronic phase but now it goes up
from 10 to 19 percent and then we start having some problems because now when you have a lot of these blast cells you're starting to again you're still making a lot of these granulates but it's starting to decrease a little bit you're still getting a little bit less granular size but you still have them but now you're starting to occupy the bone marrow with a lot of blast cells and that started to become a problem so if I get up to 10 to 19 blast cells I start to decrease the space in the red bone
marrow and what happens when you decrease the space in the red bone marrow what do you do to your red blood cell line what do you do to your platelet line so you were proliferating them to try to make more platelets but now you're hogging up all the space with 10 to 19 of it being blast cells those are big cells now you're going to drop your platelets and you're going to drop your red blood cells in this phase The Accelerated phase where now there is more blast cells this is what I really can't please
don't forget this this is the big difference here between the accelerated and The Chronic phase now if I decrease my number of platelets and I decrease my number of red blood cells what is this called This is called anemia and features of anemia may be elevant but elephant relevant sorry or evident by what kind of features pallor dyspnea or fatigue fatigue whereas thrombocytopenia is not the other feature thrombo cytopenia in the early stages The Chronic stages it presents with thrombocytosis but in the accelerated phase now you have more blast cells this is decreasing due to
the decreasing space from the more blast cells and decreasing space due to the blast cells you're decreasing your number of platelets and decreasing your number of red blood cells and now you end up with bruising and bleeding so you can end up with a petite eye you can end up with a papira you can end up with ecchymosis you can end up with gingival bleeding epistaxis Etc and these are big things to be able to take away okay so you may see thrombocytopenia in the accelerated phase whereas you see thrombocytosis in The Chronic phase you
see no effect with red blood cells in The Chronic phase and now you see anemia in the accelerated phase the other component here is that you still are going to see I told you you're still going to have lots of granulocytes it might be tad bit less granulocytes that you had in The Chronic phase but you're still going to have them so you'll still see a refractory leukocytosis if you want to think about that you'll still see a lot of these white blood cells you'll see how it's called a refractory leukocytosis and I I really
don't want you guys to forget this again you're gonna have neutrophils eosinophils that are high but one of the interesting ones that stays high and that's what's not common in many other disease is the basophils when basophils are high they release lots of histamine and histamine causes agitation to the skin and they get really itchy and so one of the features that you can see is you can see something called puritis so watch out for that especially if the basophil count is high so look for a refractory leukocytosis what with the refractory leukocytosis the basophils
will be high that's not common in many diseases so refractory leukocytosis are still going to have leukocytosis in the accelerated and The Chronic phase you'll still have a basophilia in both of these phases Puritas might start to become a little bit more evident in the accelerated phase not in The Chronic phase the last effect here is that you still can have like fevers and night sweats and things like that associated with leukocytosis but the splenomegaly becomes much worse so these really start flocking to the spleen and they really cause lots of deposition tons of deposition
of more white blood cells more extra medullary hematopoiesis so I'm going to write this as extra hematopoiesis and this causes this puppy to get big man you get some splintomegaly like a son of a gun and then there's high risk of splenic rupture and that is really really key so the spinal megaly continues to get worse in this particular phase so splenomegaly gets worse with a high risk of now splenic rupture due to lots of deposition and lots of extra medullary hematopoiesis so you can see now that when you cross over from The Chronic phase
into the accelerated phase things start becoming a lot worse and the reason why is because yes you're producing lots of you're having a lot of these myeloid stem cells that are proliferating and making tons of these other cell lines like especially the granulocytes but the problem is is that now you're starting to occupy more of the bone marrow with 10 to 19 percent of blast cells where you didn't have that much in The Chronic phase and then if you start really kind of having a lot of these like cells here in the bone marrow you
start stretching out the bone marrow and when you stretch out the bone marrow and expand that puppy then you start causing something called bone pain so watch out for that and this should really be interesting because now you're starting to see features of something called acute leukemia am I right because in cute leukemia there was anemia thrombocytopenia bone pain there wasn't like the white count could be variable right but there was lots of blast cells we remember that so now we're going to start seeing lots more blast cells in the peripheral blood than we would
usually in the chronic phase but this is starting to look like acute leukemia that's we go into the last phase the blast phase the blast phase is high mortality my friend because at this phase when you start having a patient who is in this phase now they have transitioned from CML to AML they now have an acute leukemia you're like wait you can actually get that yes because how do we classify acute leukemia acute leukemia was seen because it's the same concept here you're going to have that 9 22 translocation that's going to cause increased
cell proliferation that's going to cause decrease apoptosis with time and more replications you're going to get more mutations more mutations then lead to increasing number of blast cells you lose the ability to differentiate cells when you have more mutations you lose your differentiation capacity they divide divide divide but they don't differentiate that should sound very familiar that's acute leukemia and so now the blast cells pump up and they get up to greater than 20 percent that's AML that's AML my friends and that is what's disastrous about this potential disease okay so what I really want
you to remember is that the mutations they don't cause more blast cells directly they do it indirectly because the mutations that you get here in this particular Point here what they do is they lead to a decrease differentiation so now you can't convert the pro myelocytes and the myelocytes and the metamildocytes into eosinophils neutrophils and basophils they get stuck in the Pro myocytic stage or they get stuck in the metamilocytic Stagger they get stuck in the myelocytic stage and they don't become functional white blood cells and now you start seeing these blast cells in the
blood and that's the dangerous component of this disease so now we get everything that we already talked about everything in the accelerated phase gets worse everything now bone pain gets worse this increases anemia gets worse the thrombocytopenia gets worse so you're going to get an increase in your anemia increase in thrombocytopenia now you have less functional white blood cells and you have increasing blast cells and there's two effects here if you have less functional white blood cells and decreasing increasing blast cells and decrease functional white blood cells then you have a higher risk of infection
and then you can start seeing things like pneumonia UTI cellulitis and you know what else you can start seeing with lots of blast cells all the oncologic emergencies like what like leuko stasis like tumor lysis syndrome all those fearful things that we talked about acute leukemias so that's really what starts to happen is that what I really want you to understand just to quickly recap because this is why it's the toughest one to understand chronic myelody leukemia starts off with three phases of chronic phase it's very asymptomatic They Don't Really present much maybe just some
split omegaly and some leukocytosis with the basophilia so maybe constitutional symptoms you don't have many blast cells though so just making tons of like functional white blood cells so they're good they don't have infection risk then they develop more mutations over time they lose their differentiation capacity you start making less functional white blood cells infection risk does increase a little bit but not crazy but now you still have tons of white blood cells a lot of basophils which can cause this itchiness you still start depositing into the spleen get more splenomegaly risk of splenic rupture
but then you start dropping your other cell lines anemia thrombocytopenia you get bone pain due to expansion of bone marrow because now your blast cells just jacked up and then finally in the blast phase you turn most of those actual cells into blasts now you have so many mutations that have accrued that your blast cell component within the bone marrow has now increased to greater than 20 that's that's acute leukemia and now you drop all your cell lines you have less functional white blood cells thrombocytopenia anemia worsening bone pain and now you have more blast
cells than you did prior now you start seeing oncologic crises tumor license center of leucostasis skin cell infiltration and then because of having less function white blood cells and more blast cells you now have high risk of infections so this is really the high mortality component because now you have all the downstream negative consequences the next component is how do we diagnose this when we get a CBC with a peripheral blood smear it's a nice screening test because I told you most patients they live in The Chronic phase 80 to 85 of the time they're
in The Chronic phase so you're going to pick them up in that phase so when you get them in that phase what would their red blood cell line be pretty much normal right so generally we could say it'd be two points so let's say that it could actually be in two points here so if we were to say I'm going to abbreviate this let's say that we were what's called The Chronic phase of CML it would be normal but if we're on What's called the advanced phased or the blast phase of CML then it would
be a low red blood cell amount so you would see anemia okay so that's the important thing to be able to remember for the platelets if we were in The Chronic phase of CML we actually see high number of platelets so we see a thrombocytosis but as the disease continues to progress and you get more blast cells occupying the bone marrow taking up space in the accelerated phase or the blast phase of CML you start seeing a decreasing number of platelets so that's really really important I need you guys to remember that it's in the
chronic phase an accelerated phase there is a difference in the potential findings so in The Chronic phase of CML for the red blood cells it could be normal for the platelets it could be high in the accelerated phase and the blast phase for CML the red blood cells could be low and the playlist could be low the next thing is the leukocytes that's really the key you're going to see in All Phases usually a chronic phase accelerated phase even maybe to some degree the plus will put plus or minus plus or minus the blast phase
of CML you're going to see these crazy crazy high white blood cell counts and one of the big ones you'll see increasing neutrophils you may see increasing eosinophils but one of the ones that will be a Telltale sign and very helpful is you will see an increase in basophils and I think that is super super helpful and these white counts can be like scary high like when you first look at you're like oh my gosh this patient's dying uh and it's possibly you know that that could be the case because these things can be up
to like 50 to 200 000 white count so that's usually pretty alarmingly high white blood cell count the last thing here that I want you guys to remember is that you could see blast cells you could see blast cells on the peripheral blood smear but I think it's important to remember so when you look at the peripheral blood smear it really depends upon the stage so generally if you are in what's called The Chronic phase of CML versus The Accelerated phase or the blast phase of CML in The Chronic phase you may see actual true
functional granulocytes so you may see a lot of granulocytes and really no blast cells right so you'll see very little blast cells but when you get into the accelerated phase or the blast phase then what happens is your blast cells start going up and that's something that you want to be interested in is if on the blood smear you find a lot of blast cells that should make you think that you were more of the accelerated phase or blast phase of CML if you see less blast cells that should make you think that you're in
The Chronic phase of CML that's an important thing to be able to remember so it takes us into our next component here so we've done the CBC who peripheral blood smear it helps us to kind of have an idea of what they would look like in The Chronic phase versus The Accelerated in the blast phase right we go to the bone marrow biopsy because at this point let's say that we see a strikingly high white blood cell count with a basophilia a thrombocytosis a normal red blood cell count and then let's say mature let's say
mature appearing granulocytes with very little blast cells then I'm thinking that this could be CML especially in The Chronic phase which is where 80 to 85 percent of them live I go to the bone marrow biopsy you can do this and it would help with your definitive diagnosis but it's not absolutely crucial but you can do this and so you're going to take a piece of the bone marrow zoom in on and when you zoom in on it what you could potentially find is what we've already talked about so let's say that here we look
at blast cells and here we look at them being a little bit more mature like functional appearing so if you see blast cells you want to be able to quantify the number of blast cells that you see if it's less than 10 percent if it's 10 to 19 percent or if it's greater than 20 percent if it's less than 10 it's chronic phase CML if it's 10 to 19 it's accelerated phase CML if it's greater than 20 it's blast phase CML right that's how we could easily go about this then what we want to know
is is there granulocytes and what I would like to see is I would like to see a mixture because in patients who have AML AML they wouldn't really have a lot of like functionally appearing granulocytes they wouldn't really have many of these at all it could be variable if you get because remember what I said you could have low amounts you could have high amounts in AML but in CML that's what's really interesting is you can see some actual true functional ones like you may see some true functional like esnfls neutrophils basophils you may see
some that are like looking like myelocytes you may see some that look like meta myelocytes and so these are very interesting you wouldn't really see any of these in AML so if you see these this is more suggestive of CML and way less suggestive of AML and so that's why this is really important if you see this granulocytes and you see a mixture of like functionally appearing mature ones myocytes metamildcyte it's way more likely to be CML than AML okay but remember once you start getting into the blast phase and you see greater than 20
blast cells and on top of that you start seeing maybe less of these functional myocytes metamyocytes you may have converted over into AML so it's very important to remember okay but the big thing I think the bone marrow biopsy is really helpful for is looking for blast cells and quantifying that to determine the stage but also really helping to determine is there a lot of granulocytes that appear like they're further down the differentiation process if they're further if they are more differentiated that's more suggestive of CML than it is of AML I need you to
remember that okay once we've done this we've found that the have any of these findings and again I would really like you to remember more The Chronic phase normal red blood cells thrombocytosis and a crazy leukocytosis with basophilia likely mature appearing granulocytes or at least some myocyte metamyocyte on the peripheral blood smear do the actual bone marrow biopsy to find how many blast cells they have to determine which phase they're in and then do they have some mature appearing highly differentiated white blood cells that's likely CML then we go to the next step at this
point if I have an idea that they have CML then I just need to know is it the type of CML that has the 922 translocation 95 90 of the time yes but we need to confirm that because it determines what kind of treatment I will give them so what I need to do is I need to take their DNA put it into like a chromosomal analysis and find do they have the 922 translocation that form that BCR able Gene if they do that is important because if this is the case and I find this
922 translocation this is going to give me the treatment which I will utilize I will treat these patients with what's called tyrosine kinase Inhibitors which I'll talk about in a second so that'd be the cytogenetic component then what I would do is I would take the chromosome and I would find where that bcr-abled Fusion Gene is so this was the nine this was the 22 this is the translocation effect that we see here right from these again what you're looking for is really this this is called the Philadelphia chromosome Okay Chrome ozone you want to
be able to see this okay if that's present and they have that 922 translocation then go to PCR and quantify is this Gene present the fusion Gene the BCR able Gene is it positive if it is guess what we treat these patients with tyrosine kinase Inhibitors and again it's likely going to be the reason why because 90 of the time that's what it usually is but you need to do this so that you can prognosticate and determine their degree of treatment because if it is in this you need to find out which other type of
mutation they have because they may offer a different treatment process okay so at this point we've confirmed the diagnosis of CML we've found the specific type of chromosomal abnormality that's led to CML then what we need to do is we can add some additional tests because sometimes let's say that you only got a CBC with peripheral blood smear and you found that they had crazy high white cell count and I have an infection going on there's two different things that can happen here one is you can see CML and the other one is you can
have something called a leuko moid reaction this is usually seen secondary to infection or it can be secondary to stress so like an actual like stress in the body maybe they had surgery maybe they had some type of like procedure done of some sort maybe they had a they had a seizure so it could be one of these particular things but it's caused their white cell counts to go up so their white blood cell counts go up but they usually never break over 50 000. so they usually are less than 50 000. that's one particular
thing with CML it's not secondary to infection it's not secondary to stress it's usually secondary to a 9 22 translocation that's causing a malignancy to occur and their white blood cell counts are very high but oftentimes they're greater than 50 000. so that's one helpful thing what we also use is we use the presence of a specific molecule that can be found inside of these leukocytes I'm going to represent it here in blue and this is called leukocyte alkaline phosphatase and what the leukocyte alkaline phosphatase is indicative of is it tells us is this leukemoid
or is it CML that's all it does and so when you look at comparing these two that's really what you're using this for and this can sometimes be utilized in exams so in CML there's not a lot of lap or leukocyte alkaline phosphatase so the lap levels will be low whereas in the locomoid reactions which are due to stress or infection this is usually where their leukocyte alkaline phosphatase is very high and that might be one way of being able to differentiate these two which may come up on your exam so make sure that you
understand that the last thing that you'd also want to do here is again if you have a patient who maybe is presenting with some vague symptoms nausea vomiting abdominal fullness anorexia poor appetite maybe some left upper quadrant pain get an ultrasound or a CT of the abdomen and if you do that what you may find is this big enlarged spleen what was one of the most common features that I told you on the chronic phase which is really the only thing you can point out splenomegaly this is an important thing because you may be able
to feel a little bit on exam but get the Imaging to confirm that so then what I would do is I would get some type of splenic ultrasound or a CT of the abdomen and find that actual spirometry this is what it would look like all right my friend so now let's move on to the next step here which is the treatment of CML all right my friends so now we're going to talk about the treatment thank goodness it's actually not that bad so when we talk about the treatment of CML it's really remembering that
what was the most common cause the 922 translocation that produced the BCR able fusion protein well that was the real reason because if you actually take a look so let's say that here we take a look because what I want you guys to understand is that the treatment primary treatment for any stage whether it be a chronic phase whether it be a accelerated phase or whether it be blast phase the treatment for All Phases of CML is what's called tyrosine kinase Inhibitors the tkis and if you guys forget these there's two particular so when we
talk about these the most commonly utilized one so if we were to talk about these the agents the most commonly utilized one is going to be a matte nib but if you forget just look for tanib that's really the key way of being able to remember what was the tkis so really what do these things do well if you guys remember let's say that we take here and we zoom in on one of these actual kind of like neutrophils or one of these actual like myeloid stem cell kind of tissues what happens here is that
here is your genetic material right here is your genetic material inside we're just kind of zooming in on the cell membrane and the nucleus component here and what's happening is we said that there's two particular effects that's occurring from the actual kind of DNA component is that we are activating specific genes that will increase cell proliferation and we're also activating genes that will decrease apoptosis and so this will cause the cell to replicate and never die right which is crazy and really the primary reason is that we formed a fusion Gene and that Fusion Gene
was called the BCR able Gene and so let's say here I represent this here's going to be this receptor here's this receptor here this is called your tyrosine kinase receptor and the tyrosine kinase receptor when it actually has this BCR able so here I'm going to draw on like this blue color here this is going to be the BCR able fusion protein so this is called your B CR able protein what this does is is it goes and it actually fuses on to this tyrosine kinase receptor and when it fuses on to the tyrosine kinase
receptor it hyper activates the tyrosine kinase receptor so in any kind of stimulus hits this puppy it causes a hyperactivation which goes and stimulates these genes to increase cellular peripheralation and decrease apoptosis and so then the cells continue to replicate replicate and don't die so what if I came up with a way that I gave a tyrosine kinase inhibitor and what I really did is actually bound a drug to that BCR able protein and I inhibited it that's what these tyrosine kinase Inhibitors do so really what these are going to do is is these drugs
are actually going to inhibit they're going to bind to the BC ariable fusion protein and inhibit it from actually hyper activating this receptor then you inhibit the signaling pathway you inhibit the genes that are responsible for cell proliferation so you shut this down and then you shut down the genes that are responsible for trying to prevent apoptosis and you actually induce apoptosis and this is one of the ways that we can treat CML pretty interesting right that's the main way now if patients fail tyrosine kinase Inhibitors then you can move on to something called a
bone marrow transplant so the other option that exists for these potential patients is you could do something called a bone marrow transplant and this option is usually because they it's secondary too failure of tkis the last potential thing that I want to talk about here is we can do something called cyto reduction so we can do something called cyto reduction so obviously this would be one way which would be the tkis but sometimes when patients have like these crazy crazy high leukocyte counts and crazy like high thrombocyte counts the problem is it doesn't cause symptoms
and so when they start actually experiencing symptomatic problems so symptomatic high white blood cell counts or symptomatic high platelet counts then you should do cytal reduction and we don't necessarily use tkis we actually use a very specific agent here and this agent would be something called hydroxy urea and this is helpful in really kind of knocking down your white cell count especially when they are strikingly and alarmingly high so this is another potential option so I want you guys to remember hydroxyurea if they have symptomatic high white blood cell counts and high platelets you can
consider hydroxyurea really drop down their white cell count but the main stay of treatment is tires and kinase Inhibitors my friends in this video we talk about CML I hope it made sense I hope that you guys enjoyed it and as always until next time [Music]
Related Videos

1:19:53
Non-Hodgkin's Lymphoma
Ninja Nerd
141,996 views

48:45
Acute Lymphoblastic Leukemia (ALL)
Ninja Nerd
222,633 views

43:13
Hematology | Hemostasis: Coagulation Cascade
Ninja Nerd
2,174,695 views

9:50
What is chronic myelogenous leukemia? | He...
khanacademymedicine
215,806 views

1:02:10
Diarrhea | Clinical Medicine
Ninja Nerd
61,297 views

45:46
Acute Myelogenous Leukemia (AML)
Ninja Nerd
179,531 views

17:59
Chronic Myeloid Leukemia (CML) - Myeloprol...
Medicosis Perfectionalis
439,152 views

14:07
The Banality of Evil
Dr. John Campbell
211,514 views

34:10
Chronic Lymphocytic Leukemia (CLL)
Ninja Nerd
123,391 views

26:14
How to Treat Chronic Myeloid Leukemia (CML...
OncBrothers: Practice-Changing Cancer Discussions
2,126 views

1:00:50
Hodgkin's Lymphoma
Ninja Nerd
177,009 views

46:22
Chronic Obstructive Pulmonary Disease (COP...
Ninja Nerd
188,532 views

1:17:18
Acute Myeloid Leukemia - Diagnosis and Tre...
The Leukemia & Lymphoma Society of Canada
90,470 views

1:27:14
Nephrolithiasis | Kidney Stones
Ninja Nerd
250,141 views

20:12
Hematopoiesis | Erythropoiesis
Dr Matt & Dr Mike
73,535 views

1:04:26
Parathyroid Disorders | Clinical Medicine
Ninja Nerd
47,115 views

13:10
Acute Leukemia - ALL and AML - Hematology ...
Medicosis Perfectionalis
394,354 views

1:29:49
Nephritic Syndrome
Ninja Nerd
189,563 views
10:22
Chronic Myeloid Leukemia (CML) | Pathogene...
JJ Medicine
151,902 views
26:54
"I Had Every Symptom of Leukemia & I Expla...
The Patient Story
79,507 views