What Is Rheumatoid Arthritis? | NEJM
54.9k vistas2245 PalabrasCopiar TextoCompartir

NEJM Group
In this Double Take video from the New England Journal of Medicine, Drs. Schubach,
Gravallese, and ...
Transcripción del Video:
[Music] rheumatoid arthritis or ra is a disease affecting Millions worldwide in this video we'll discuss what is currently known about the pathogenesis of RA and how it relates to the challenges clinicians face when choosing the appropriate therapeutic approaches for their patients rheumatoid arthritis is one of the most common immune mediated inflam diseases patients present typically with symmetrical polyarthritis of the hands and feet and seropositive patients will also present with auto antibodies but this is a systemic disease and so rheumatoid arthritis involves many other organs and systems as well morning stiffness is a common clinical sign
of almost all forms of inflammatory arthritis however morning stiffness lasting longer than 30 minutes is typically seen in patients with rheumatoid arthritis most people diagnosed with RA are between age 30 and 70 and women are 2 to three times more likely than males to develop the disease while it is not known exactly what causes rheumatoid arthritis genetic factors such as the presence of variant hladr alals and specific environmental exposures such as smoking are part of the equation early diagnosis and treatment of rheumatoid arthritis are critical to improving quality of life and preventing irreversible damage rheumatoid
arthritis is a clinical diagnos nois we need to see the patient and examine them and what we look for is the number and location of the joints that would be involved with arthritis uh we would look for the duration of the disease looking for a disease that's present for 6 weeks or longer we look for acute phase reactants and we may get an x-ray to look for bone erosions there are two different types of RA to determine which type a patient might have a physician will order serum laboratory tests ra is divided into CER positive
and serer negative and if we want to see if the patient is C positive we would look for the presence of Auto antibodies and these would include rheumatoid factor and anti- citrated protein antibodies or acas rheumatoid factor and AAS are not found in Ser negative individuals however other types of Auto antibodies may be present in general we view Ser negative and copositive as being really different diseases the copositive individuals have certain genes that they're associated with that are not found for example in ser negative ra and then disease severity is generally significantly worse in seropositive
disease they have more citis more joint destruction greater likelihood that they're going to require joint replacement Sur surgery on the other hand the way we treat them is actually quite similar the preclinical stages of copositive rheumatoid arthritis are characterized by disordered immunity with a breakdown of Tolerance and auto antibody production uction there is a genetic predisposition in patients with ra and people who have a first-degree relative with RA are at about a 2 to fivefold greater risk of getting the disease these patients who are genetically predisposed May develop Auto antibodies they may develop acas and
rheumatoid factors and this means that they are at risk for the disease but they don't actually have the disease at that point the mean duration of the preclinical phase of RA is typically about 4 years prior to the onset of disease but in some patients this may last 10 years or more patients may experience a second hit perhaps from a viral infection that will precipitate active disease environmental triggers such as infections and notably smoking can result in disordered immunity which may start at mucosal surfaces such as the airway spurred by these changes some proteins May
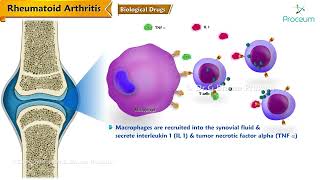
undergo a modification called citrol lination in which an amino acid arginine is converted to citruline within a predisposed individual antigen presenting cells see these proteins as foreign bind to them and migrate to the lymph nodes and mucosal lymphoid tissue there they activate CD4 positive t- helper cells which stimulate B cell proliferation and differentiation into plasma cells which produce acas and rheumatoid Factor many of these immune cells migrate through the blood to the synovium where they release pro-inflammatory cyto kindes like interferon gamma and Inter lucans this triggers neighboring cells such as macroasia monocytes and sovial fiberblast
to release cyto kindes notably tnf il6 and il1 as a result sovial fiberblast proliferate contributing to Joint inflammation as the disease progresses abnormally proliferating synovial cells and cause a tumorlike growth called panis to develop eroding cartilage and Bone other bone destructive Pathways also become activated made worse by the inhibition of bone repair Pathways as a result patients develop articular bone loss and systemic osteoporosis meanwhile acas and rheumatoid factor form immune complexes that activate the complement system promoting chronic inflammation chronic inflammation is accompanied by angiogenesis which allows additional trafficking of immune cells to the joints and
produces additional pro-inflammatory factors exacerbating existing processes in ra patients may experience unpredictable symptoms exacerbations called flares rheumatoid arthritis is a disease that can wax and weigh there are times when the symptoms are are either not apparent or patients are in remission or have low disease activity then there are other circumstances where often times for reasons that nobody exactly understands uh um the disease will suddenly flare either generally or only in a few distinct joints the the actual mechanisms for how one goes from say remission or low disease activity to a flare are not certain a
2020 study showed that in the weeks leading up to a flare circulating B cells become activated followed by the appearance in peripheral blood of pre-inflammatory mesenchimal cells or prime cells Prime cells appear about a week before a flare and are hypothesized to migrate into the synovium to trigger inflammation therapies have improved dramatically in the last three decades with the Advent of targeted approaches however choosing the most effective therapeutic strategy for each patient can be challenging individual patients with ra appear to have different pathogenic mechanisms and we base this on the fact that patients will respond
either for example to an anti-tnf and not to an anti-il 6 or they may respond to a t- cell Co stimulatory inhibitor and not to an anti-tnf and so it does seem that patients have very unique uh pathogenic mechanisms and the important thing is to find the right drug for the right patient we don't always have biomarkers or predictors of what pathway will be driving disease in a given patient and so the trick is to get to the point where you have a patient on a medication that addresses their own particular pathogenic mechanism and gets
their disease under control rapidly there is now a large armamentarium of treatments for this disease and these drugs have been revolutionary deards are diseas modifying anti-rheumatic drugs and they control inflammation prevent or slow joint destruction and potentially reduce the risk of death if started early there are three classes of deards conventional biologic and targeted synthetic the conventional dear methotraxate a folate antagonist is usually the first line course of treatment typically rheumatoid arthritis will be treated with methotraxate and about a third of the patients will respond to Methotrexate alone Methotrexate was first introduced for the treatment
of RA in the mid 1980s and it was a huge breakthrough medication and actually targets a number of pro-inflammatory Pathways uh probably one of the most important things it does is upregulates adenosine which is an anti-inflammatory molecule in the local inflammatory environment what happens then is that there's suppression of multiple immune Pathways uh there's a decrease in the production of cyto kindes including is 1 Isle 6 Isle 8 uh there's a suppression of maccrage activation uh decrease in nutrifil Recruitment and other pro-inflammatory Pathways will be suppressed as well uh by methodi biologic agents introduced in
the 1990s may be used alone or in combination with methat trexy or other conventional Demars currently available biologics Target t- cell co- stimulation specific cyto or Surface markers on B cells to interrupt the cycle of inflammation biologics are proteins that require systemic Administration either by intravenous or subcutaneous Roots so there are many biologic agents that are now being used in rheumatoid arthritis we have biologic agents that will Target cyto mines for example we have five biologic agents that Target tnf and block its functions in the immune system we have two agents that block the is
6 receptor and therefore block the effects of is 6 in this disease we have agents that can deplete B cells rmab is the example there uh and we have agents that can block co- stimulation of tea cells so that te- cells don't become activated and these are all very effective depending on the patient and their pathway of disease a highly effective class of medications are the Jack Inhibitors a type of targeted synthetic Dart these drugs are small molecules that can enter the cell and interrupt cyto networks by blocking signal transduction so depending on how you
design these Inhibitors you can interfere various patterns of cyto kind signaling and they it turns out that they're actually quite effective um in blocking that communication system from the surface of the cell uh into the interior the cell and work as well as blocking the cyto themselves so in that way you're actually able to um block the effects not just of one side cyto but of multiple cyto simultaneously treating flares depends on multiple factors including duration and localization during rheumatoid arthritis flares we have to make a decision um one is whether or not we think
the flare is going to be persistent and if there's a persistent flare it may mean that we either have to advance therapy with the agents that they're currently on uh or whether we need to change therapy for example if someone has a flare and they're on Methotrexate if they're not in the optimal dose of Methotrexate and there's room to go in terms of the dosing it's not difficult to increase that dosing on the other hand if everything is maxed out and there's no room to go then you may have to switch Therapeutics other really important
change uh over the last 30 years is a concept which is called treat to Target and this is a concept that tells clinicians we need to get inflammation under control as quickly as possible and as effectively as possible so we now have measurements for uh identifying the level of inflammation in a patient and these are called dis disease activity scores and these disease activity scores will cover things like number of swollen joints number of tender joints maybe pH physician Global patient Global assessment um maybe acute phase reactants and they give us a number and with
that number we can actually follow the level of inflammation in a patient and we can treat so that that inflammation is as low as possible now that we are able to control inflammation better we are really looking for remission and if we can't get remission we want low disease activity and we will modify our medications so that we get to that point although tremendous progress has been made in the last 30 years there are several unmet needs in the treatment of arthritis there are still patients who don't respond adequately to any of the medications available
patients may go into remission but could have a recurrence of their disease perhaps from a discontinuation of their medications this means that rheumatoid arthritis requires lifelong treatment despite this clinicians remain optimistic there have been huge advances in the treatment of rheumatoid arthritis over the last 30 years we have so many medications now to choose from that are really effective in getting infl under control but what I'm most excited about is the possibility of disease prevention we know that we can identify a patient at risk for ra this may be a patient who has a first-degree
relative with ra who is at genetic risk for the disease these patients we can follow and we can potentially intervene to prevent the disease and there have been a number of studies of prevention that have not yet actually gotten to the point of prevention but we have been able to delay the onset of disease which I think is very promising and the possibility of intervening so early that we actually prevent arthritis from occurring at all is a real possibility now and I think that's what I'm most excited about I'm optimistic that we will be able
to ultimately individualize therapy there is something different about every patient with ra and and they all have their own form of the disease I do think that we'll be able to stratify people and I think we'll be able to do it with a blood test we want um and I think we will achieve a situation where clinicians can set up a blood test and within the next few days get an answer back and they'll say this person need an aisle six in hinder for example as researchers increase their understanding of the underlying pathogenic mechanisms of
rheumatoid arthritis new opportunities for individualized interventions that treat or prevent disease should emerge so for those with ra a timely diagnosis by an RA specialist along with Rapid Control of inflammation through early and aggressive treatment are the key to managing this [Music] disease
Videos Relacionados

22:47
How I REVERSED my ARTHRITIS NATURALLY as a...
MYAutoimmuneMD
1,134,703 views

14:31
How 2025 Could END Rheumatoid Arthritis Fo...
Dr. Diana Girnita - Rheumatologist OnCall
41,673 views

14:46
Medical Mystery Solved – A Diagnostic Sequ...
NEJM Group
36,501 views
![Rheumatoid Arthritis [Symptoms, Early Signs, Stages & BEST Treatment]](https://img.youtube.com/vi/CTtIMGqTwXQ/mqdefault.jpg)
22:30
Rheumatoid Arthritis [Symptoms, Early Sign...
Michigan Foot Doctors
171,367 views

15:34
Rheumatoid Arthritis Pathophysiology (sign...
Armando Hasudungan
967,833 views

35:20
Rheumatoid Arthritis (RA): More Than a Dis...
Specialty Pharmacy Times
195,053 views

28:25
Use These 5 Food Hacks To Heal The Body & ...
Dr. William Li
427,426 views
16:48
Rheumatoid Arthritis Pharmacology - DMARDs...
Dr.G Bhanu Prakash Animated Medical Videos
4,209 views

11:57
Medical Mystery Solved — A Swell Diagnosis...
NEJM Group
16,791 views

18:55
10 TOXIC Foods for Rheumatoid Arthritis
Dr. Diana Girnita - Rheumatologist OnCall
73,823 views

1:24:24
Inflammatory Arthritis: Types and Treatments
Arthritis Society Canada
1,028,237 views

8:58
Psoriatic Arthritis
Zero To Finals
647,682 views

12:49
#066 Anti inflammatory food diet for chron...
Dr. Andrea Furlan
3,690,775 views

10:31
Early Warning Signs Of Rheumatoid Arthriti...
Dr. Diana Girnita - Rheumatologist OnCall
396,434 views

19:51
Managing Rheumatoid Arthritis and all aspe...
TEDx Talks
165,649 views

14:51
Osteoarthritis and Rheumatoid Arthritis - ...
Level Up RN
226,900 views
12:28
Rheumatoid arthritis - causes, symptoms, d...
Osmosis from Elsevier
2,069,119 views

45:38
Living with Rheumatoid Arthritis - Dr Carm...
Arthritis Ireland
17,462 views

9:48
The Scary Link Between Rheumatoid Arthriti...
Dr. Diana Girnita - Rheumatologist OnCall
37,501 views

13:54
How to cure Rheumatoid Arthritis | Symptom...
The Yoga Institute
983,533 views