Cholinergic Drugs | Pharmacology | Dr Najeeb
303.75k views19807 WordsCopy TextShare

Dr. Najeeb Lectures
#cholinergic #drugstoremakeup #pharmacology #pharmaceutical
Cholinergic Drugs | Pharmacology | Dr ...
Video Transcript:
so my friends today we are going to talk about at last cholinergic drugs right the drugs which produce in our body actions which are normally produced by acetylcholine right so we are going to talk about cholinergic drugs now cholinergic drugs are those drugs which increase the cholinergic activity in our body now cholinergic drugs are primarily classified as direct acting cholinergic drugs direct acting cholinergic drugs and in direct acting cholinergic drugs now what is the real difference between the direct acting and the indirect acting let's suppose this is a cholinergic neuron right and this neuron is
releasing from here acetyl choline that's very right and acetylcholine is going to work on this tissue this specific tissue and let's suppose here is cholinergic receptor of course cholinergic receptors may be ion channels or they may be yes seven pass G protein coupled receptors right now as you know when acetylcholine is released of course it can still it will stimulate post junctional cholinergic receptors as well as prejunctional cholinergic receptors but very rapidly it is catabolized and catabolizing function is done by the enzymes and these enzymes are called yes these enzymes which catabolize the acetylcholine right
these are called acetylcholinesterages these enzymes are called acetylcholine nestrasis is that right now these enzymes are very well concentrated at the synaptic membrane synaptic Junctions especially with the post synaptic membrane right as well as with pre-synaptic membrane acetylcholine stresses and Zions are present in very high concentration in association with post-junctional membrane and pre-junctional membrane is that right now as you know that as soon as I still choline starts its action very rapidly it is destroyed by acetylcholinesterase enzymes having this basic concepts now I will explain what is the meant by the direct acting cholinergic drugs
and indirect acting cholinergic drugs direct acting cholinergic drugs are those drugs direct acting cholinergic drugs are those drugs which can actually directly work at the receptors what are direct technical energy drugs direct technical energy drugs are those drugs right which are structurally or functionally similar to acetylcholine right and direct actin drugs or energy drugs are those drugs which can bind with cholinergic receptors some of them bind with the nicotinic receptors some other direct acting bind with the muscarinic receptor still there are some others which will bind with the nicotinic and muscarinic both receptors so what
are direct acting cholinergic drugs the drugs which directly activate the cholinergic receptors right then we talk about indirect acting cholinergic drugs now indirect acting cholinergic drugs must be increasing the cholinergic activity in our body but not directly not directly acting on The receptors indirect cholinergic drugs basically inhibit the action of yes the inhibit the action of what is this acetylcholinesterase let us Suppose there is a drug which can bind here and inactivate the function of what is this still cholinesterase and such drugs which can bind with the acetylcholinesterase right or even stresses at the Junctions
right and butioral choline stress is present in plasma right so most of the indirect acting cholinergic drugs are the drugs which bind with the what is this a style cholinestrages and inhibit them when the action is inhibited then what will happen whatever endogenous acetylcholine is released it is not destroyed and its life increases and it's still choline accumulate at the synapses and its action on The cholinergic receptors increases right in this way indirect acting cholinergic drugs by inhibiting acetylcholine stresses enhance the action of endogenous acetylcholine Amma clear no question now let's go in little detail
so what is the different types of direct technical Energies first I will discuss about the direct acting cholinergic drugs in the lecture and later on we will talk about indirect acting cholinergic drugs now direct acting cholinergic drugs they may be mainly muscarinic muscarinic drugs which are dominantly stimulating The muscarinic receptors and other group is nicotine drugs directing drugs which stimulate the nicotinic receptors preferably now in the musculinity drugs which you would bind with the muscarinical energy receptors and activate them it means these drugs has Affinity with the musculinity receptor as well as they have a
capability to intrinsically stimulate musculinity receptors because if a drug bind with the receptor but does not stimulate then it is antagonist but if a drug bind with the receptor and stimulate then it is Agonist so of course now we are going to talk about muscarinic cholinergic drugs it means these are muscarinic Agonist it means this group of drug can bind with the musculinity receptors and stimulate them am I clear right now in this case there are two types some of the drugs are cholines choline esters esters and others are derived from the plants that is
their alkaloids alkaloids now choline esters do you know us can you tell me a single cholinester drug it in which choline is present in esterified form please tell me acetylcholine acetylcholine is a Esther of choline right even though it is not used as a drug I will tell you later why but at least you should tell me acetylcholine which is a compound which is which can stimulate Mass Clinic of course but it can also stimulate nicotinic right acetylcholine is not you can say selective to muscarinic right now acetylcholine then there are some other molecules which
are produced by modification of acetylcholine or the molecules which are structurally similar to acetylcholine but there are some significant differences for example there is a drug called methylcholine there is a methyl group here methylcholine then there is carboxyl karba coal in this case in place of acetate there is carbamate you know Stell Colleen has acetate and choline this has carbamate and choline carboxyl is that right then there is another compound that is called bethenical the tenacol in Bethany call again actually with the choline there are carbamates not not acetate right now bethenicol also has a
methyl group addition if you don't want to remember there's no problem but you have to remember this thing that metha choline carbacol and methane coal they are basically molecules which are able to stimulate the muscarinic receptors right preferably especially about the tenacol it has a main action on muscarinic but it does have some little action on nicotinic also but others are mainly on the mask mainly on muscarinic sorry let's do a little correction but then equal is mainly muscarinic carboxyl is musculinity with little nicotinic foreign then there are alkaloids can you tell me alkaloids yes
can you tell me some alkaloids which are derived from the plant and which can stimulate the muscarinic receptors right at least tell me musculine my screen is why masculinity receptors are called muscarinic receptors because they can be stimulated by musculine and muscarinas derived from plants right or mushroom so mascreen mascarine any other drug which is derived from the plant and it can stimulate the musculinity receptor yes that drug is very very important one of my friend is again and again saying cocaine right of course we'll study cocaine but not in this lecture yes yes pilocarpine
have you heard of pilo carpin right so these are direct acting dominantly musculinity drugs in which methachary and carboxyl methane call they are choline Esters and muscarin and pilocarpine they are the alkaloids is that right we'll discuss them in detail now right and nicotinic drugs we will talk study them with the CNS stimulants an indirect acting cholinergic drugs we will discuss after discussing these drugs right so let us go into detail of these drugs foreign ergic system now this lecture is going to be dangerously easy too much easy let's start one by one first of
all we talk about a drug called acetylcholine now first of all what I want to say acetylcholine is usually not used pharmacologically why okay there there's a one answer someone is saying we don't use a style choline as a drug because we have already have it okay we have many other things but still we may take it as a drug also yes no it's not the right answer anyone can tell me that when we want to stimulate cholinergic system in our body for some therapeutic purpose usually we don't use acetylcholine why yes my friend question
is very simple that acetylcholine you know so well about it but when we need to increase cholinergic activity in our body usually we don't use acetylcholine why yes okay but the real real reason is that acetylcholine has a very very short half-life that's measured in seconds is that right why because when acetylcholine is injected it will be very very rapidly destroyed by but Royal Holiness phrases which are present in plasma and you know other names for butyl choline stresses non-specific cholinestrages pseudocolaneous phrases right so butylcholine stresses or the pseudo collinear stresses or non-specific coronary stresses
these are one and the same enzyme having three different name and they are abundantly present in your circulation of plasma and because they are present abundantly right and they destroy the pharmacologically introduced acetylcholine rapidly so acetylcholine cannot and of course not only acetylcholine is destroyed by pseudocolinestrages whatever acetylcholine you push in your body that will be also destroyed by the acetylcholine stresses right because of this Rhythm acetylcholine acetylcholine has a very very short life if you inject it it will last in your blood from 5 to 30 seconds only so this is one reason that
usually when we use we want to use a cholinergic drug therapeutically we want a longer longer action is that right so this is one reason that very short half-life right it's very rapidly destroyed in our body right number two acetylcholine has diffuse action Estelle choline if you really inject it in heavy doses if it reaches to its Target receptors it will produce multiple diffuse activities in the body and usually pharmacologically we require a drug which will hit a specific action in our body right so second reason is because the style choline work on all its
nicotinic and muscarinic receptors it activate the whole cholinergic system in our our body non-specifically diffusely and due to that reason it does not have an important pharmacological application this is diffuse because it produces diffuse activation of cholinergic system activation of nicotinic and muscarinic receptors so you can understand it can go to the central nervous system stimulate nicotinic and muscarinic receptors in central of a system but here I said something wrong it does not go to Central number system the reason being it is highly charged compound it is highly polar compound and it cannot cross yes
cannot cross biological membranes including the blood brain barrier right it cannot cross biological membranes you know biological membranes like bloodborne barrier or there is placental barrier or if drug is taken orally it has to absorb from git mucosa git mucosal barrier these barriers are made of cells and their membranes which are lipid by layers and drugs which are highly charged they cannot effectively cross the different biological barriers including the acetylcholine so still choline has these multiple problems due to that reason it cannot be used as pharmacological agent because it is destroyed very rapidly in our
body right it is a very short uh duration of action secondly if really you get it in the body in higher concentration it will produce diffuse activation of nicotinic and muscarinic receptor all over the body cholinergic activity will start it's not something to be very happy about that and it cannot cross biological membranes effectively right but just speaking hypothetically right let's do a little practice what we learned in previous lectures if I spell choline is given in heavy amount and transiently it activates a cholinergic system in all our body it stimulates the energy receptors all
over the body what will be the results ready number one which site will be activated what are the sides of the cholinergic receptors cholinergic receptors basically cholinergic receptors which one they are present in four four we can classify in so many way one ways they are present in central nervous system secondly they are present on ganglia it means and which ganglia sympathetic or parasympathetic both so it means if a style choline will go and stimulate all your parasympathetic Anglia and sympathetic ganglia there will be such a diffuse action and non-selective action right thirdly yes cholinergic
receptors especially muscarinic receptors they are present at neuro effector site of neuro effector yes sides of post ganglionic foreign Ty fibers parasympathetic fibers so all the tissues where parasympathetic poles King learning fibers are going they are having cholinergic receptors all those tissues will be stimulated do you think it's a limited action or very diffuse it's very diffuse and in the end you don't forget cholinergic receptors are also present and neuromuscular Junctions so do you think that if you give a drug like acetylcholine okay if it is given in general circulation it will not Cross Blood
wind barrier but at least it will stimulate the ganglia it will stimulate all the neural effector sites where parasympathetic posting learning fibers are giving cholinergic activation and also neuromuscular Junctions do you think you are getting some non-specific action on the body or specific non-specified due to all these reasons this is not a very good drug generally speaking what will happen to someone who has massive cholinergic stimulation you know already there will be heavy sweating there will be lacrimation pupil construction ciliaris spasticity yes nasal secretions Broncho construction and tracheobronchial secretions then a lot of salivatory action
yes all git secretions will be more git motility will increase defecation will occur and you come to the heart what will happen bradycardia and if Estelle choline goes to the blood it bind with the M3 receptors on the endothelial cell massive amount of nitric oxide is released excellent all of you know that massive wizard dilation and hypotension and then you don't forget along with the defecation there will be also urination because the trouser will be stimulated so do you think it's some very good action that you give someone really a good injection of a style
choline and he is sweating and he's electromating and he's elevating and he's urinating and he is defecating and he's dying with cardiovascular collapse with having uh pupils do you think it's something great so now you understand it why I style choline is not a great drug is that right now we go to some of its related compound as I told you there is botanical carboxyl methylcholine right let's talk about those drugs first of all I will talk about a style choline related drugs which are but then we call the tear knee call now Botanical has
relatively stronger action on muscarinic receptors right one of the best way to remember Bethany call is yes and its action is and its uses you can remember its actions and uses by a very simple thing yes but that that is a boy's name or girl name you are sure okay the other things are not good Beth activates Bubbles and bladder vowels and bladder even though girls like to activate other things but here the batch is activating bowel than bladder I mean um gastrointestinal system and urinary bladder is it a good news okay it's not good
news for Beth or the person who is going to have that but for Bethany call for the doctor it's a good drug it's called Energy drug we strongly stimulate musculinity receptors on the git and urinary bladder so if you want to activate in a patient gastrointestinal system or you want to activate his urinary bladder with any call is a very good drug is that right it does not have any significant nicotinic action right in pathanical the acetate with the choline there is acetate in acetylcholine but in Metheny call acetate has been replaced by carbamate but
then you call what happened that acetate is replaced by carbamate now you remember there was a drug called sorry enzyme which is called acetyl cholinesterase now this enzyme which is called acetylcholinesterase is that right now this enzyme very effectively destroy the style choline right but actually this cannot so effectively destroy the Botanical the reason being bethenical is a slightly different molecule where acetate has been replaced by carbamate and this acetyl is an enzyme which breaks down the Ester link between the acetate and choline this enzyme is not very effective in breaking down the Ester link
between choline and carbamate so this drug will be destroyed Slowly by acetylcholinestrages and butyl choline stresses so this drug will have short duration of action like acetylcholine or this will have a longer duration effect longer duration of action you understand it in bethenical you can say it's a modified acetylcholine in which acetate has been replaced by carbamate and this change in the molecule does not allow the choline stresses to destroy this molecule very effectively so due to that reason right this drug is destroyed relatively slowly so it has a longer duration of action as acetylcholine
has 5 to 10 or 20 seconds but this has duration of action usually more than 60 Minutes or one hour is that right it's a significant thing that something which is destroyed in 10 second now it can stay for 60 minutes or one hour is that right now because now the secondly not only here in this drug with any call not only acetate is replaced by carbamate but there is also addition of methyl group there is a addition of methyl group and when methyl group is added to this drug right and right this molecule this
molecule does not bind with nicotinic receptor so that's a good news or bad news it's a good news because now action of this drug become it's a little bit specific it become more selective are you getting it we really like the drugs which can act for longer duration in some situations and we like the drug which will hit exactly those receptor where we really want to have an action so acetylcholine and methane call how they are different than methane call acetate is replaced by carbamate and there is a addition of methyl group so duration of
action of this drug become longer and it's by its capability to bind with the nicotinic receptor is reduced so it's mainly having action on muscarinic receptors and specifically it loves to activate musculinity receptors on gastrointestinal system and restaurant system and urinary bladder so you can say that breath activates bubble and bladder how you remember B for bath B for Bobble B for bladder is that right there's no other popular drug in this group we start with B right so B for Beth the tenacol B for vowels B for bladder right so next time someone asked
you with any call what is function it activates vowel then bladder is that right any question up to this now what should be its uses very easy to understand it should be used this drug can be used when bladder is not Contracting properly or when gastrointestinal system is not Contracting properly that's so simple you don't need to be genius to answer this this drug will be used when there is hypoactive git and the hypoactive urinary bladder is that right but make it sure there should not be any obstruction before I tell you indication I should
tell you contraindication if someone has a urinary retention right look if there's a poor man having urinary retention because there is a Stone here Stone here or there is malignancy here or there is some structure here there is some obstruction to outflow do you think we should give a drug like Bethany call not at all if there is obstruction to uran outflow right don't give any call you know why bladder will strongly contract and patient will have severe pain but if there is a fixed stone or some tumor here right patient will only have very
severe pain and he will remember your face this was the Doctor Who did something and then I had my trouble was aggravated if someone has urinary attention to benign prostatic hyper profit PPH do you think you should give bethenical no we will give drugs like bethenical to activate the urinary bladder when the retention of urine is without any Outlet obstruction when retention of the urine is because bladder is not Contracting well right so we can say that this drug can be used to activate the urinary bladder in cases of non-obstructive urinary retention what kind of
urinary retention non-obstructive urinary retention is that right now what could be these conditions this may be postoperative urinary retention classical example not due to Stone this may be post operative urinary retention sometimes after the operation patient cannot pass Azure and endurance is retained probably is autonomic nervous system is not working well does the right of ganglia are not working well in the pelvic organs or in the abdominal and your patient is unable to pass the Assurance but due to retained urine he feels strong discomfort right so in case of post-operative urinary retention where there is
no outflow obstruction we can use this drug then any other condition post yes postpartum urinary retention what is postpartum when a woman has delivered a baby usually women deliver the baby and some of them they develop urinary retention after delivering the baby right in that case we call it postpartum urinary retention again there should not be any outflow obstruction and then you can push the activate the bladder by giving an injection subcutaneous injection of bethenical right so Betty moves the bowel and bladder that's so easy is that right urinary retention or postpartum urinary retention right
then in some other chronic hypotonic or myogenic or neurogenic bladders or some cases in which there is chronic hypo tonic in different diseases urinary bladder become hypotonic it does not contract well or myogenic that muscle is not the truth or is not Contracting or neurogenic right bladder so when there is hypotonic bladder or myogenic or neurogenic bladder right in these conditions urinary bladder does not contract well and usually urine is retained and retention of urine is dangerous it predisposes the person for urinary tract infections right so rather than keeping a catheter inside one of the
ways that you use Botanical to activate the urinary bladder am I clear to all of you yes right now let's talk about when we need to activate the vowels when we want to activate the git pharmacologically yes again when there is post operative a dynamic Alias you know what is alias post operative a dynamic alias aliasmine paralysis of git after abdominal operations many times git is not after the operation it is not mobile and if it takes very long time to recover its mortality we can activate the git by bethenical am I clear so or
those cases which we call it a tonic atonic yes stomach atonic stomach or we call this conditions gastroparesis when someone has a stomach which does not contract well or whatever he eats it is well rotained in the stomach and it does not push properly to the duodenum you can activate the stomach motor function or enhancer and potentiate the stomach motor function by bethenical is that right or there is Alias aliasmine paralysis of git Alias due to any toxic reason Alias due to any toxic reason toxic cause right we can activate the git but there are
a few things which are very important before activating the Git You must know that there is not any destruction in the jit because if there is some obstruction in the git for example interception and you give birth any call patient will be in trouble already there's a Blog in git and very strong parent Strauss has come maybe G80 perforate rupture right so make it sure as I told you when there's urinary retention you want to activate the bladder you should be sure there should be no obstruction in the same way when you activating the git
you have to be careful that git is not having any instruction right am I clear there should not be any obstruction then another condition in which this drug can be used that is called congenital Mega colon congenital Mega colon what is congenital Mega colon now what's the underlying problem yes who is going to tell me what is congenital Mega colon what really happens Mega colon look this is colon of course this is cecum and here is your ilium coming and your friend appendix okay now you know that this part of the colon that is supplied
by Vegas and last part of the colon this is supplied by origins or pelvic parasympathetic nerves now sometimes it happen that ganglia are absent from A short segment of cologne This Is A congenital defect that neuronal ganglia you know or back plexus and mesnar's plexus these ganglion do not develop in small segment of the colon maybe the neurological ganglion system from this side and this side where it was supposed to fuse they remain short short of fusion so there is a ganglionic segment in the git there is a ganglionic segment a segment in the colon
without any ganglion so what really happens that this part of the colon contract but when it brings the material here can it push forward no so in a way this will become a a dynamic part of cologne it does not Propel and have motility properly right so in a way the proximal part of the colon become Mega enlarged right because this is there is an obstruction at this point this is not a physical abstract obstruction this is problem that cologne is unable to create motility in a short segment so whatever uh you can say content
of git are coming they are retained proximal to that point and we say that cologne is becoming very large Mega colon and this problem may be present congenitally we call it congenital Mega colon some of these cases with congenital Mega colon can also be managed by administration of botanical is that right no problem here okay having said all these things now let's talk about what could be the side effects of bethenical who will tell me again let's repeat Bethany call is having longer Half-Life as compared to acetylcholine because it is replaced its acetate with carbamates
and it does not bind and stimulate the nicotinic receptors because it is methylated also activate Bubbles and blood are very messy business right so all those conditions where we want we need to activate the urinary bladder or gastrointestinal musculature we can use with any call but we should make it sure there is no obstruction to forward movement then I was talking about what could be the side effects I think by this time you must be able to tell me side effects will be all the side effects which are produced by generalized cholinergic stimulation generalized EK
stimulation right so what about this it's so easy to understand sweating will be there salivation will be there lacrimation can be there abdominal secretions and peristalsis and abdominal cramps may be there yes urgency or you can say ah rush to urinate has it right then there may be flushing and hypertension flushing is what the cutaneous blood vessels dilate don't confuse it with blushing blushing is a different thing when you blush you know that some part of the skin under emotional state it blush on right but these days when girls don't blush what they do they
put the blush on right but don't confuse the blushing with flushing flushing is generalized cutaneous Vaso dilation so what will be the actions again generalization of cholinergic that this drug is given little more there will be sweating let's start from the top there will be sweating meiosis meiosis with uh spasticity of ciliaris and difficulty to focus the eyes so blood VN then with that there can be Fletching then there can be yes salivation lacrimation salivation come down bronchoconstriction and tightness in the chest and then bradycardia and hypertension related complications can come and gastrointestinal secretions are
increased along with modality and cramps Domino cramps and then in various may be defecation and urinary right now these are the side of course these are the generalized side effects produced by generalized cholinergic stimulation then there are some specific contraindication to the use of botanical there are some conditions we should not use with any call because it is called Energy external and for example in peptic ulcer patient why because muscarinic stimulation can increase the secretion of a gastric acid right so it is contraindicated in peptic peptic ulcer disease okay it is also contraindicated in copds
chronic obstructive pulmonary diseases why because it produces bronchoconstriction so already they are having problem that people who have chronic obstructive pulmonary diseases at the top you give this drug okay you will move the bowel but you will stop the oxygen is that right so it's contraindicated then patient with the ischemic heart disease with coronary problem if someone has coronary atherosclerosis a part of myocardium is getting less blood flow at the top you give this drug and hypotension less pressure and less blood going into coronary further drop in the ischemic area blood flow and that may
precipitate myocardial infarction is that right even call Energy action uh in the patient with the in the editory itemias right because it reduces the what is that effective refractory period in the atrium and it can precipitate then this is also contraindicated in hyperthyroidism the answer is simple and hyper thyroid thyroidism why it is contraindicated in hyperthyroidism because patients with hyperthyroidism many of them do have eritreal tachycardia or atrial flutter already and when you give muscarinic stimulant right they may go to atrial fibrillation am I clear again the causes because muscrenic drugs can reduce the refractory
period effective refractive period in atrial tissue right okay the last contraindication which I'm going to tell you is Parkinson's Disease Parkinson's disease why in Parkinson's disease normally what is happening balance between acetylcholine and dopamine is Disturbed you know in the central nervous system dopaminergic activity and cholinergic activity they are in balanced what really happens in Parkinson's disease that nigrostriatel neurons are degenerated so dopamine activity become less and relative to dopamine cholinergic activity become more and X so dope in Parkinson's disease reduce activity produces hypokinesia and in Parkinson's disease excessive chronologic activity produces primers and at
the Top If such patient is given cholinergic drugs am I clear okay having said everything about any call now we go to the next drug and next drug is Karma call again in karbakol there is also acetate replaced by carbamate but there is no methylation and now you can understand it will stimulate muscarinic as well as to some degree nicotinic are you understanding me right so both of them have longer duration of action but here there was there are carbomates here carbamates here there was methylation here but no methylation here due to this reason it
is able to stimulate muscarinic plus nicotinic action so do you think it will be very useful drug no so these days it is not commonly used systemically karbachol is not commonly used systemically because it can intensely stimulate the generalized stimulation of the ganglia right and initially it stimulates the yes it stimulates the ganglia and then ganglia go into depression so first stimulate and then inhibit right in the same way it stimulate neuromuscular Junctions and then inhibit right so due to this reason it has a strong stimulation to cardiovascular system and then depression strong stimulation to
git and then depression so do you think such kind of drug is very good to use systemically so thank God we are not using systemically so you don't need to remember much about it the only important use of this drug is in the eyes right we use Karma called for the producing meiosis meiosis and also uh for contraction of cilians muscle actually by these actions it help us to lower the intra ocular pressure in patient with glaucoma now how the meiosis and how the silurus contraction reduces intraocular pressure that I will explain later when I
explain when I will explain the ah pilocarbon right I will tell you exact mechanism for a while you just trust me that by producing strong mule contraction of the sphincter pupili and the contraction of the celiers we reduce the intrapular pressure these days in glaucoma to reduce the intricular pressure pylo carbine is a preferred drug as compared to carbocol so this is used in patient of glaucoma only when pilocarpine is in a factor so again you do not need to know much about this drug right this is enough to know that it is a meiotic
agent right it can be used to reduce the intraocular pressure in glaucoma but usually it is not the first line drug then we come to another drug and that is called a methylcholine that is methacholine and again now methylcholine is not systemically used it has one common juice you know what is the use of methylcholine these days those patients where we suspect that these patients have hyper reactive bronchial system there's a term used bronchial hyper reactivity bronchial hyper reactivity mean that if bronchial tree is little bit irritated it will intensely produce Bronco spasticity or construction
right so if we have to diagnose a person of with asthma or we are not sure he's having asthma or not then we check his bronchial hyperreactivity we give little inhalation of methylcholine we give very little very very little methylcholine by inhalation which will produce very little bronchoconstriction in a normal person but that amount of methylcholine will produce strong Bronco relatively strong bronchoconstriction in a patient with hyper reactive bronchial tray Amic layer of course before doing this test you should have bronchodilators with you am I clear right so with a methylcholine is having one important
juice these days that it can it is given by inhalation right to challenge the bronchial tree to check for the hyper reactive bronchial smooth muscles is that right and after the giving this inhalation we check the respiratory function test and we see that there is a little drop in the airflow right or there's a big drop in airflow so this is the only use in methylcholine now let's go back Botanical death activate vowel and bladder very good so easy carboxyl can activate many things but we don't want it right we just put in the eyes
only when pilocarpine and other first line drugs are not working well right and they can be used carboxyl can be used in glaucoma as a second line or maybe last line drug methacholine again there's only one juice it stimulates the musculinity receptors we give it by inhalation to the bronchial tree to stimulate the musculinity receptors on smooth muscle to look for the bronchial hyper reactivity Amma clear and now we come to the last drug in this group that is pylo carbine that is with what I would really love to explain little bit more Philo carbine
this is important drug to know right now pilocarpine again it's a muscarinic drug is that right it's a tertiary a mine right it can it is traditionally a mine and it is stable with acetylcholinesterasis stable mean it is not easily destroyed by acetylcholine nestorages so its Half-Life is long right as compared to astral colon significantly Long pylo Carbine is basically an alkaloid derived from the plants right and it is stable to the action of a style choline stresses now what are the important uses of acetylcholine right number one there are ophthalmic uses okay let me
tell you it is used in patient with glaucoma in patients with glaucoma this is used topically topically mean what right it is applied directly to the cornea and conjunctival Sac we put it there right from there pilocarpine will be absorbed and it will act on The muscarinic receptors on the sphincter pupili and it will also act on musculinity receptors on ciliaris muscle right and it helps to improve the pressure now exactly how it worked let me tell you first I will tell you how the aqueous humor normal circulation is present in the eyeball let's suppose
here is your eyeball and now a very important thing which you must know first of all is I will put the lens here this is the lens here is your what is that IRS right and here is what pupil this is the pupil right there's Iris here now this is cornea this is the Clara am I right this is the Clara here is cornea now actually and of course here is your suspensary ciliary body I must produce so ciliary body with ciliaris muscle is fixed over here foreign and of course you know that there are
zonular player now what is the circulation of aqueous humor I should enlarge this area to show you in the detail now aqueous humor is produced by celery epithelium from here right by that it moves between the lens and Iris on the back of the iris and then from here it moves into interior chamber through the pupil a consumer is produced by of course you must be knowing here is something which is called vitreous body this is full of humor is produced by what is this celery body having celery special epithelium it is secreting the aqueous
humor it is moving through the posterior chamber so sphere chamber is behind the iris an interior chamber is in front of Iris and a prostitution and interior chamber communicate through what is this pupil so aqueous humor is produced in the posterior chamber are secreted in the posterior chamber it moves towards the pupil and through the pupil it goes interiorly into tear chamber and in the interior chamber it moves to the corneal secular Junction this is the cornea and this is saklera and this is the corners clear Junction and here now this is the point to
understand that here there are at corneous clearal Junction there are special type of trabeculi here connective tissue Network we call it trabecular mesh worm Network right and here there is a very special vein which is called Canal of schlem and here also what is this called Canal of schlem now aqueous humor move was secreted by celery surface comes into posterior chamber through the pupil it comes into interior chamber and while washing on the back of the cornea it comes down and on up or you can say from the center it moves to the periphery at
cornmeal Junction it moves through this trabecular network what is this tropical Network and through that it drains into Canal of schlem so it is coming like this from here it will percolate and then come into canala schlem which is special Venus drainage system here and eventually then it will drain into other veins and go to eventually to the systemic veins is that right this is how this is a circulatory system of the aqueous humor now what happened when it was humor expression the intraocular system is very high we say there is glaucoma right now why
what are the different types of glaucoma there are many types but I will explain only now closed angle glaucoma and open angle glaucoma first you want me to explore explain close angle glaucoma or open angle glaucoma yes tell me what you want first open angle or closed angle okay let's have a little break and then we will continue right so we were talking about glaucoma uh I was saying that there are two types of glaucoma there is open angle glaucoma and open angle glaucoma and close angle or nerve angle it's same thing narrow angle or
closed angle glaucoma now first I will explain the open angle glaucoma in open angle first of all what is angle first of all we should know which angle we are talking about it is narrow or wide or actually narrow angle is between the corneal and Iris is that right now or corneous chloral Junction is having this angle and at this angle there is a let me tell you this angle should be considered like this and like this is that right in this angle what is this trapular mesh work a network of connective tissue and collagen
system is that right now this is the angle through which normally aqueous humor field filter and reach to the canal of schlem and then to be drained is it clear now what happens sometimes doctor found that in some patient angle is open they can see that regular mesh work but pressure is high later on they came true in these people actually within this trapular mesh work right there is narrowing angle is not narrow angle is not narrow but this filtering system is having some resistance to flow why maybe with the Aging as our age increase
Our arteries become hardened or softened Our arteries become softer hard in the same way with that age there is some change in the connective tissue here right and it is it becomes difficult for aqueous humor to move through this mesh work and drain properly but when you look at the angle angle is open we also call it open angle glaucoma or wide angle glaucoma now initially doctors could not understand but now they know that there is a resistance within this mesh work in this case if you use a drug which will contract ciliaris what will
happen when ciliaris will contract it will pull the angle posteriorly when ciliaris muscle will contract it will pull the angle posteriorly and when it will pull the angle posteriorly what will be happen that there will be traction on this network and it will open am I clear Jesus you understand it what is happening that we are using a drug here which is going to lead to contraction of what is this contract it has a traction or pull on the on the tropical mesh work and slightly open it right and that will help the better drainage
of a consumer and intraocular pressure will be going down am I clear so this is how it works in open angle glaucoma but pylo carbine is also very well known for the shoes in acute cases of narrow angle glaucoma now first of all I must tell you what is narrow angle then I will tell you what is narrow angle glaucoma and then I will tell you how popular work actually narrow angle mean in some people right actually anterior chamber is shallow the some people interior chamber is shallow it is not deep this is less and
some people have relatively smaller eyeballs or congenital or you can say that developmentally their eyeballs are designed like this that distance between the iris and the cornea is very little so they are having relatively narrow angles now these people who have a narrow angle they have one problem some of them eventually develop a problem that when pupil will dilate they develop glaucoma how let us suppose if pupil dilate then it means the cons dilateral people I are opening the pupil and pupil will move from this place to the periphery rather than irises like this when
people will dilate configuration of Iris will be change now you see pupil which was previously like this it is large but when people are dilatation dilation is there then actually Iris goes away from the center and moves to the periphery and root of the iris so base of the iris become Broad are you understanding you are not understanding okay let me tell you here come look this is the iris right now this is the base of this is the base of Iris right and here is what people is that right now if we produce pupillo
dilation I'm changing that then this will of course this point will not change this point will go outward right when it will go up outward what will happen that this will be more broadened this will also come here and this will be more broad end are you understanding it so what really happens that when there is pupilo dilation right Iris moves to the periphery and root of the iris or base of the iris become accumulated at what point at what point it become accumulated near the corneoclear junction and this angle will become wide or it
will become narrow it will become narrow so what happened well when if already someone has relatively narrow angle at the top there is people of dilation then root of the IRS which accumulate at the angle and make the angle narrow this is one problem so due to this reason these people who has a tendency to develop narrow angle glaucoma especially in early time they develop this problem when they go to at night or in the rainy season or when they go to Cinemas because in pupil dialect significantly for longer time root of the IRA succulent
at the periphery and hinder the drainage another problem which occur in these patients is that intraocular pressure become very high of course when drainage is blocked due to narrow angle intraocular pressure will become lower high High when it becomes very high then what happens that aqueous humor is unable to move forward because there's a block here it cannot drain aqueous humor accumulate here in the posterior chamber and then this equals humor pushed the iris forward are you understanding what ecosumor is doing when it is accumulating here too much under eye pressure it push the IRS
interiorly that further closes the angle and that closes the angle and so much pressure become High that there is very severe pain here so we this is a case where there is very severe pain and even edema of the cornea develops due to high pressure right I become red so red eye with very high pressure it may be a case of acute case of narrow angle glaucoma your understanding so what are the neuro angle glaucoma in which when you look there you find the angle is really narrow is that right now in this case pylo
carbon is wonderful in emergency cases we put repeatedly drops of pilocarpine what pilot carbon will do here it will lead to what is this so sphincter people I it will lead to the contraction of sphincter pupili and intense contraction will pull the root of what is this Iris away from the corner so when there will be pupillo construction Iris will be pulled centrally right and there will be less accumulation of root of Ira so base of Iris at the angle an angle will become opened and again drainage will become better am I clear do I
need to repeat it again everyone is clear about it so we can say pilocarpine or any drug which is myotech as well as producing contraction of ciliaris they can be used in glaucoma cases in case of open angle glaucoma and in case of open angle glaucoma these this angle is open resistance is within the tropical mesh work but when cilia's contract it has a traction or pull on the Network and open it and facilitate the what is that drainage of the ecosumor but in narrow angle glaucoma or closed angle glaucoma physically this angle is narrow
right either eyes are designed with smaller anterior chamber or there's bipolar dilation and root of base of the iris is accumulated at the angle and at the top when pressure becomes High then pressure in the posterior chamber push the iris interiorly all these things combined make the angle very narrow here if you give the drugs which are strongly neotic or they produce strong stimulation of constrictor people I then constrictor people I will lift the iris away lift the iris away from the Angles and angles will be open is that right so this is the use
of pilocarpine in patients with glaucoma then another use of pilocarpine is pilocarbine can stimulate very strongly your secretions it really piles on sweat tears and saliva pilocarpine piled on it is not other piles which is a disease piles on yes sweat tears and saliva sometimes it's so powerful sweat glands are so sensitive to pilocarpine that if you give one shot of pilocarpine you may have two to three liters of sweating diaphoresis right but what is really important right now is that to understand that pilocarpine has one more juice when we want to stimulate saliva secretion
if and tear secretion there is a disease a condition which is called zero stomia dry mouth don't tell me romantic ways to make the mouth wet we can do it pharmacologically also right zerostomia when there is a dry mouth dry mouth can result due to head and neck irradiation if someone unfortunately other tumor of head and neck and he has been irradiated maybe that will destroy the some of the parenchyma of the parotid glands and other salivary glands so when saliva is less your mouth is all the time dry and do you think having a
very dry mouth is a very good feeling no so how much water the person can drink just to keep his mouth wet mouth may not be wet by drinking so much water but maybe bed will be wet right so one of the treatment is we give pilocarpine and these days we use pilocarpine spray in the mouth or tablets right they can stimulate the slavery secretion if there is some residual what residual gland left there right another condition where we use this is shogran syndrome this is that these autoimmune disease more commonly in females where autoimmune
process destroy the salivary glands and lacrimal glands you can imagine these females their dry eyes and dry mouth yeah right in the syndrome and for these patients also we can give pilocarpine or another new drug which is longer lasting duration of action that is sevy line another drug is savvy line sevy line this is also musculinity drug with longer action and it is also stimulate the slipper production is that right so pylo carbine is an alkaloid they write from the plant having strong muscarinic action right you know whatever the muscarinic actions can be produced by
pilocarpine if it is given systemically usually we don't use pylo carbine systemically major juices are two number one in glaucoma and number two in zero and any other questions you have yes OK another condition some other ophthalmological conditions we also use pylo carbine you know if someone has severe pupillo dilation or midrases due to atropine for example due to some reason you put atropine in someone eye right and then you want to reverse the mid reassess you will put pilocarbon so another uses when you want to reverse the atropy in induced what materials is you
can use pilocarpine you can use pilocarpine then pilocarbine is also used along with the medriotic drug when there are adherence between Iris and the lens this is the lens and if there are some adherents between Iris and the lens some in some inflammatory condition of the eyes right adherence May develop between the Iris and the lens sometimes to break these adhians we alternatively give people a Constructor and dilator right we give popular dilator and try to stretch it outward and then give people a Constructor pull it inward so repeatedly alternate it eventually these adherence may
break so another use of pilocarpin is the alternative use of pilocarbon with medriotic drugs to break the adherence between the iris and the lens is that right do you have any question no let me check what you have learned today we were talking about cholinergic drugs we have mainly discussed direct technical energy drugs indirect acting drugs we will discuss in next lecture right in direct acting called Energy drugs I said acetylcholine cannot is not commonly used as a drug right why number one it has a short duration of action it is rapidly destroyed by colonist
phrases number two it is a diffuse action all over the body no selective specific actions right then I will talk about bethenicol with any call and methylcholine and carbacol and pilocarpine all of them have longer duration of action as compared to a style choline now but then you call what are its most important two uses Power movement and bladder movement that's very good but in cases of obstruction if there's outflow obstruction to Bladder will you use with any call no very good then we come to carboxyl carboxyl as muskrinic as well as some nicotinic actions
we don't use it commonly systemically even though it can produce strong stimulatory and then depression on the cardiovascal system or on the git but karma college is not commonly used systemically presently it is used less commonly in the cases of glaucoma when pilocarbine is ineffective right methacholine methylcholine is used when to check the bronchial hyper reactivity is that right then in the end we are left with pilocarpine what are the two important uses of pylo carbon number one in the mouth and number two in the eyes for the eyes for the eyes we use it
in open angle glaucoma because drainage it can be used also in close angle glaucoma where strong meiosis pulls the iris root away from the angle and open the angle right secondly in the eyes it can be used to reverse the nutriasis produced by atropine thirdly to break the adhes between the lens and the IRS pilocarbon can be used in alternation with not combination alternating use alternating use with the nutrientic drugs right in the end pilocarbon can also be used as a shallow Gog shallow Gog mean the producing agent which produces lot of saliva right and
this type of juice is required in conditions of zero stromia and mouth is very dry right zerostomia can be produced by a radiation of head and neck right or it may be produced by autoimmune destruction of slavery glands like sjogren syndrome in which lacrimal gland is also significantly destroyed if there is some residual gland left there we can stimulate that by the pilocarpine and get some salivation right we can keep our mouth wet and we can also keep our eyes wet they said yeah eyes may become very dry we call it zerothalmia so having zero
ophthalmia or zero stromia is not a very pleasant feeling is that right and class dismiss all right so we were studying about the cholinergic drugs and let's recap a little uh last time we were talking about the drugs which are cholinergic drugs they can be divided into yes two groups they were direct acting direct acting and yes indirect acting very good and indirect acting direct acting for those drugs which could direct which could directly stimulate the cholinergic receptors right and in that the drugs which were working on muscarinic cholinergic receptors we discussed in last lecture
into detail right let me take a little assessment of you there was a drug which direct acting called energetic drug which could activate the bowels and bladders what was that okay and pilocarpine is used in narrow angle glaucoma or clue or wide angle glaucoma both of them right now you can tell me that bethenical right bethenical has powerful muscarinic action or nicotinic action yes muscarinic action very good and another question that pilocarpine increases secretions and it can be used to stimulate the saliva production right in which condition syndrome and when there is zerostomia in or
which may be due to irradiation to head and neck that's great so now we start over today's work we are going to discuss indirectly acting cholinergic drugs now what are indirectly acting cholinergic drugs these are those drugs which basically bind and inhibit choline stress enzymes as we I discussed last time that if this is a cholinergic neuron and if this neuron is releasing here acetyl choline acetylcholine is going to work on this tissue suppose this is a tissue right which may have ION channel receptors which are nicotinic receptor for acetylcholine or seven pass G protein
coupled receptors which are Serpentine receptors now you remember that we discussed acetylcholine can work on nicotinic receptors or can work on muscarinic receptors but very rapidly it is catabolized right and it is catabolized by an enzyme called yes acetyl acetylcholine nestress right this enzyme rapidly destroys acetylcholine now our today's lecture is about those drugs which can actually bind with this enzyme the drugs which can bind with acetylcholine stress and the drugs which can inactivate the action of poly nestrase a drug which has bound and it reduces the action of acetylcholinesce phase and if any drug
bind with acetylcholinistrates and does not allow it to destroy the acetylcholine then endogenously released acetylcholine Half-Life will increase and it will accumulate at the synapses and its action on the nicotinic and muscarinic receptors well prolong an increase so in a way the drug which bind with a steel choline stresses and inhibit them they increase the concentration of acetylcholine in the synapses and indirectly they enhance the cholinergic action in our body is that right so today's lecture is about anticholinas stressors now anticholinar stresses drugs indirectly attain drugs or anticolinesterages there are two types of the drugs
they are reversible reversible Inhibitors of acetylcholinestrages and there are irreversible irreversible Inhibitors of Inhibitors of acetylcholinestrasis right what I mean by this there are some drugs listen carefully they bind with this enzyme right this enzyme and enzyme keep on working on those drugs but it takes a very long time that enzyme get rid of those drugs reversible drugs bind with the enzyme but over many minutes and hours those reversible drugs detach so it means these reversible anticholinistrases keep the enzyme action inhibited for many minutes or even many hours is that right but these irreversible anticholinar
stresses once they bind with the anti-coline stresses right gradually this so strongly bind that enzyme is never recovered this is a very important thing that reversible drug bind with enzyme but sooner or later they detached from enzyme right or the saturnz I am free but once the irreversible drug bind with the enzyme it never let the enzyme free it means enzyme activity is lost for not forever it is lost for many days and weeks until New enzymes are synthesized by the tissue because if you'd you can say you are inhibiting these permanently that what will
happen if patients survive then tissues will produce more enzymes right so it is very important to understand that reversible enzymes reversible drugs inhibit the enzyme for shorter duration right irreversible drug block the enzyme or waste the enzyme activity for the life of the enzyme but actually when new enzymes are synthesized by the tissue then recovery will be there if patients have survived is that clear now I will first start discussing the reversible drugs and then I will go to irreversible drugs so we are talking about the cholinergic drugs and cholinergic drugs are direct acting which
stimulate the receptors and indirect acting which inhibit the choline style choline stresses and increase the concentration of endogenous acetylcholine by reducing the destruction of acetylcholine right now we start discussing one by one anticholinistrases and T holyness phrases is a group of drugs which are reversible reversible later on we'll talk about irreversible foreign ERS phrases there are many group many drugs one of them which I will discuss first of all that is physiostech mean physio trigged mean now physiostick mean is an alkaloid it means it is derived from plant this is number one thing that it
is alkaloid and so it is derived from the plant secondly this is tertiary a mind the structure is tertiary a mind now here I want to make it clear in this group some of the drugs that tertiary mines and some of them are quaternary Amine do you think this thing has any importance that if I say this drug is if I say this rugged tertiary of mine and this is quaternary amine what is the real difference created by this system yes okay very good excellent one of you saying that these drugs will behave differently in
regard to blood print barrier right uh let me tell you tertiary amine are less polar and quaternary Amanda are more polar less lipid soluble again let me tell you the drugs which are treasurya mines they are less polar and more lipid soluble drug which are quaternary amine there are more polar more charged they have more charges on the surface and the less liquid soluble now only this thing that right tells you a lot about it for example the drugs which are less polar they will be able to absorb from git better because less polar drugs
or more lipid soluble drug will cross the biological membrane lipid membranes more effectively because fisostic mean is tertiary mind right and it is more lipid soluble so what it will do by those treatment it will be able to absorb from the git effectively it will be able to Cross Blood print barrier is that right fiber segment will be able to Cross Blood wind barrier even fiso stigma will have more action on the ganglia because most of our ganglia are embedded in fat and these are leopard soluble they can enter into fat and have more action
on the ganglia opposite to that this other drug which I will discuss later for example neostragmen Neo stick mean then I will talk about later pirito pyrido strike mean I will also talk later about a drug which is called adrophonium now why I put this name because I want you to have a clear concept Pfizer stigma is tertiary a mine and all others are quaternary of mine right all these are quaternary amines so it means this is less polar and more lipid soluble and these are more polar and less lipid soluble so it means phy
those treatment will be able to cross the blood wind barrier and produce action in the center of a system and even can produce toxicity in the central nervous system but neostrigment pyridus treatment hydrophonium the more polar molecules they cannot Cross Blood band barrier effectively so they cannot produce CNS toxicity is that right Amma clear in the same way if you compare Pfizer's treatment and neostratic Main right it is more lipid soluble it is less lipid soluble because fiber statement is more lipid soluble it will dissolve into fats and reach up to the ganglion so it
will have stronger ganglionic stimulation and near stigmund does not very effectively dissolve into fat so it does not very effectively stimulate the ganglion am I clear now no problem here another thing which is which you are supposed to know that this is alkaloid but this is synthetic drug this is synthetic drug this is synthetic drug right this is derived from plant and these three are synthetic drugs another difference which is very important to know that first three of these they are having carbamate group and this one is alcohol group right now you may be thinking
why it is so important to know a little detail let me tell you why let us post this is your enzyme I'm going to show the action of different drugs on yes acetyl cholinesterase now look hydrophonium hydrophonium bind with the enzyme relatively Loosely hydrophonium bind with the enzyme relatively Loosely and very rapidly detaches hydrophoneum we can put it like this this is The Binding of adorophonium right right now adrophonium does not make a strong covalent bond it does not make a strong covalent bond and it rapidly dissociates it so its duration of action will be
more or less less usually hydrophonium work may be 10 to 15 minutes 10 to 20 minute at the maximum 10 to 20 minutes adrophonium but then there are other drugs like physiostick mean neostigmen physostic mean or neostigmen they bind here but they do make covalent bond they make covalent bond but these covalent bonds which are made by neostragmen or phytostragment they are labial covalent bond what are they they are labile covalent Bond labile covalent bond is labile covalent bond is actually a bond which can be eventually broken labile covalent bodies there is a covalent bond
which is a strong bond but it is labial it is not forever eventually it breaks down and Drug goes away an enzyme can restart its function is that right now it is very Loosely bound it is little more tightly bound right so its duration of action will be more than adrophonium right it its duration of action is usually 30 minutes to two hours or in some of some some of these drugs up to four hour these are the drugs which are carbamates listen carbamate make libel covalent bond now what are carba made carbamates are physio
streaming neostrichment pyridostigma right they make the labile covalent bond with enzyme right so they from half hour to few hours they keep on inhibiting the enzyme but when we come to adrophonium it does not make covalent bond adrophonium bind very very weakly it makes a non-covalent bond so it rapidly dissociate within few minutes so its action is not more than 15 to 20 minutes then I told you another class of anticholinas phrases irreversible antical Industries right irreversible anticholinistrases are really dangerous do you know any irreversible anti-choline stress irreversible anti-choline stresses those drugs or rather we
should say toxic compound which bind with this enzyme very very strongly they bind here very very strongly right they are making strong covalent bonds they are making strong covalent bonds irreversible anticholinistrases and another thing initially when they bind initially when they bind they can be removed from the drug but after few minutes after passing of a literal time they saw strongly react with the enzyme then you cannot remove it again let me tell you for example this is the drug which is binding over here it has a special alkyl group here alkyl group when irreversible
anticholinas traces bind with the enzyme of course enzyme is very very sad it's very sad rather it is weeping you know why because this is also sad but not vaping and here it is really tricky it knows it will get out now listen adrophonium bind very Loosely and within 10-15 minutes detaches enzyme recovers activity recovers carbamates like neostigmund fiso statement pyrito statement bind with covalent way right but this is labile covalent bond not a stable covalent bond and eventually they also detach but their action of inhibition remain from half hour to few hours is that
right the real problem is irreversible anticholinistrases irreversible anticholinar stresses are can you tell me some name ISO fluorophyte t isoflorophyte or echo thiophage echo fade at or there is Mela thion or there's another drug which is Para thion now isoflorophyte or echothyofate are I think this H is not there echothyophyte on parathione and related compound they're very nasty compound they make very stable covalent bond with their style cholinesterase right so they really bind it strongly and then another complication is there once they remain sticking to the enzyme for about 30 minutes or more right then
this circle group detaches remember clearly if alkyl group is still there when enzyme is sticking with this drug or toxin toxic compound initially initially alkyl group is there actually there are other drugs which can come and remove the inhibition but once alkyl group is detached it is impossible to remove the compound from there again let me repeat it these groups are having a special alkyl group and this alkyl group alkyl group you understand it's ch2 ch3 ch3 like that propile or okay alkyl group is there in the beginning when drug bind with the enzyme right
alkyl group is still with the complex until alkyl group is there we can bring some anti dot which can remove this from there that empty dot is called probably doc sign what is the name of that anti-dot that is probably dock sign what is the function of priority of sine it can remove this from here it can remove this probably dock sign rally dog sign right but after 30 minutes or so this alkyl group automatically detaches and if it detaches do you think we can recover enzyme regenerate enzyme no enzyme is truly lost forever this
process of loss of alkyl group and then drug permanently enzyme this process is called Aging what is that this process is called Aging aging aging why this concept of Aging is so important why I'm trying to stick your hammer in your mind the reason being if someone is accidentally or someone wanted to commit suicide by these drugs or homicidal attempt if someone these compounds have gone in his body and these enzymes are inhabited if at initial time very rapidly you provide prolidoxin before the alkyl group is lost before the Aging has occurred you may save
the patient right but if due to some reason diagnosis could not be made in time or due to any reason you have not given pralidoxin before the aging process and aging has been done then parallel toxin cannot work as a very effective anti-dot you must know such compounds are present in many insecticides have you heard of insecticide or pesticide poisoning right they are present in many insecticides we spray on the crops right these compounds are not only present in insecticides or pesticides unfortunately scientists are working very hard to make more and more such compound for
military issues and the bad news is that recently they have made some compound which are irreversible anticholine stresses which can age in few seconds which can undergo the aging process Within few second and if someone has been exposed to those nerve gases or nerve agents is that right what will happen very rapidly all the anticholinar stresses in the body will be inhabited and while most of the anticholine the stresses are inhibited and permanently inhabited what will happen all the acetylcholine which is normally physiologically endogenously produced it will dangerously accumulate at the cholinergic sites and there
will be massive massive massive cholinergic outflow and you can understand what will happen so we were talking if someone has exposed to irreversible anticholinist traces right how you will what will happen to the patient that most of the most of the rather all of the style colonist phrases will be inhibited and endogenously produce Estelle choline will accumulate and produce very powerful cholinergic stimulation in the person body right and that will produce signs and symptoms of what is this toxicity by these now there are four tissues or four levels at which estrell choline accumulate and produces
complications number one in this if if if some of these substances which can cross the bloodborne barrier they go to the central of a system and enzymes are inhibited in central of a system there will be very strong toxic accumulation of a cell choline in central of a system and it may stimulate the central nervous system so powerfully that patient may develop convulsions right scissors secondly acetylcholine accumulate in the ganglia sympathetic and pair of sympathetic and parasympathetic ganglion and there's powerful pathological stimulation of ganglions ganglia thirdly acetylcholine accumulate at the what is this neuro effector
site of parasympathetic nerve endings and all over the body this very powerful muscarinic stimulation because at these sites there are muscarinic receptors and last but not least is that there's a lot of accumulation of a stealth choline at neuromuscular Junction and this nicotinic receptor that neuromuscular Junction when they are very strongly stimulated for very long duration right they what happened they produce depolarizing nerve block and paralysis again let me tell you that if this is your cholinergic nicotinic receptor if it is over stimulated you remember from previous lecture if it is it's still calling bind
and detach it will let the cations go in but if Estelle choline is in very high concentration and remain attached with Design Channel for very long duration ion channels will become dysfunctional and neuromuscular transmission will fail and patient will develop paralysis right develop paralysis but not only patient develop paralysis and conversions patients also develop a lot of what is that clinical features related with the muscarinic cholinergic stimulation for example there will be massive sweating there will be lacrimation there will be yes salivation right then as you go down what else will be there bronchoconstriction bradycardia
hypotension right over stimulation of git abdominal cramps and there may be even diarrhea there may be urination right so all generalized fish over stimulation of cholinergic system will produce its signs and symptoms in such patients is that right the point is that when we you treat such treat manage such a patient the point number one is that you should give atropine advantage of atropine is that at Roman pain will block The muscarinic receptors so all those clinical features which are problems which are produced due to over stimulation of muscarinic receptors they will be abolished secondly
we should give some chemical entry dot the classical uh substance available is pearly doxim now pralidoxime how it functions prolidoxine bind the what is that organophosphorus compound irreversible what is this irreversible anti-coline extras drug right and it bind and detaches that but remember pralidaxine is only effective when aging has not occurred aging has not occurred it means when alkyl group especially present with the organophosphorus phosphate compounds all these compounds are also called Organo phosphates so if organophosphate are still having alkyl groups right and they have not gone under aging then pralidoxin will remove the organophosphate
from the enzyme and enzyme will be regenerated but if aging has occurred right some significant time has passed and aging has occurred it means now this uh drug as bound so strongly with the enzyme by losing its alkyl group it has so strongly bound that even if some antidote like Pirelli toxin come it cannot regenerate the enzyme am I clear another way to remember okay so this was some basic concept again very Loosely binding this is what acetylcholine stress very Loosely binding compound is hydrophonium right it is very short acting then there is carbamates right
which are like physiostick mean neostrigment pyrito statement they bind and inhibit the enzyme for half hour to few hours right but organophosphod compounds are irreversible compounds once they bind there they're really inhibited for very long time and after some time by losing the alkyl group right the drug organophosphate compound right binds so tightly that even pearly dog sign cannot remove it and that process is called agent is that right now let's come back and to this discussion we were talking about reversible anticholinistrases and let's discuss first of all phyder statement as compared to other fiso
treatment is more lipid soluble right and why it is more lipid soluble because it is not quaternary it is not quaternary a mine it is less polar more lipid soluble so it can go to the central nervous system either statement can go to the central nervous system is that right now what will be the actions of physical stigma if someone is given phytostigmine systemically what will be the action it's so easy to understand all these sides central nervous system stimulation will be there ganglionic stimulation will be there what is this sites will be stimulated and
at neuromuscular Junction uh nicotinic called Energy receptors will be stimulate so we were talking about the therapeutic uses of phytostagnant right now physiostick men where it can be used number one it can stimulate muscarinic receptors it can stimulate muscarinic receptors specially on the git and bladder urinary bladder so it can be used to stimulate the motility in gastrointestinal motility and urinary bladder motility right you remember there was another drug which could stimulate the bowel and bladder but then he call right so physiostick men can also be used in the conditions where normally withinicol is used
the difference in fisostrichment and methane call is with any call is directly acting muscarinic stimulant right you remember I told you with any call could directly stimulate the muscarinic receptors on git and bladder breath activate the bowel then bladder actually physostigmin can also stimulate the bowel then bladder indications are same as you remember that post-operative abdominal distension due to paralysis of git right you can use phy those pigment or if there is non-obstructive urinary retention if there is non-obstructive urinary retention post-operative or postpartum you can use physiostick men again remember the thanicolon fiso treatment both
are used for this condition the difference is methane call directly stimulates the musculinity receptor but geophysical statement actually does not stimulate the receptors it actually inhibits the breakdown of acetylcholine and then endogenous acetylcholine increases its action at cholinergic receptors right secondly fiber statement can be used in glaucoma also you can understand why a 50 statement is right applied topically to the eye right to the cornea it will constrict it will lead to construction of pupil you can understand why accumulation there and contraction of ciliaris muscle is that right again why because acetylcholine is accumulated there
sometimes pilocarpine and physiostechmen are applied in combination how in some some cases in case of glaucoma you can give pilocarbon and fisostrichment both why pilocarbon can directly stimulate the muscarinic receptors and sphincter pupilion ciliaris and phyther segment by inhibiting the choline stresses increase the what acetylcholine concentration in the on the Splinter bipoli and ciliaris muscle am I clear there is no problem right you can understand of course when meiosis will be there the the base of the Iris will be lifted away from the angle and it is good in case of angle closure glaucoma and
when ciliaris contract it produces attraction of pull on the tropical system trabecular mesh work at the angle and that enhances the drainage of aqueous humor and that is good in case of open angle glaucoma right then another uses another use of physiostagmines in those patients where due to some compound cholinergic activity is reduced for example there are some drugs which have anticholinergic activity for example if you have given me toxic dose of atropine then what will happen that my muscarinic receptors are pathologically blocked and if you want to bring action on muscarinic receptors you can
give physiostagment and physiostream will go even to Central our system as well as in the peripheral part of the body and increases the concentration of a style choline right and then acetylcholine can displace the atropine and or even the presence of atropine it may initiate some of the muscarinic action you are understanding it so it can be used in overdose of overdose of atropane so in atropine toxicity right atropine is a drug which blocks which receptors musculinity receptors right and if someone has overdose toxicity of the atropine you can give what is this physiostech Main
and it will increase the concentration of acetylcholine at the synapses and at higher concentration of acetylcholine there will be muscarinic action restored right even there are some other drug like phenothiazines these are the drugs which are used as antipsychotics antipsychotic drugs these drugs also have anticholinergic activity if someone tried to commit suicide by taking lot of phenothiazines right so there will be powerful anticolinergic activity phenothiazines block The muscarinic receptors atropine broke the muscarinic receptors right so it means that atropine has anticholinergic activity phenothiazines do have anticholinergic activity so to restore cholinergic activity in these conditions
you can give phytochragments am I clear why you are looking lost your understanding me okay that's good and then tricyclic antidepressants price I click antidepressant this group of drugs also have anticholinergic activity right tricyclic antidepressants can also bind with the cholinergic receptors and block and if someone tried to commit suicide by taking a toxic dose of tricyclic Entry depressants one of the part of the management is giving the physio stagman right what firefighter statement will do it will increase the steel choline at synapses by inhibiting the strelcholine stresses so that there is an effective what
is that there is effective activity on the cholinergic receptor right so what are the main action of physio statement number one for those treatment can be used to mobilize the git or urinary bladder like methane call it can be used in glaucoma patient right along with the pilocarpine or independently it can be used in those toxic state where there is too much anticholinergic activity in the body then we can use Fiber segment to upgrade our cholinergic activity in the body Amic layer and what could be the side effects of physiostegment side effects of physical statement
number one is central nervous system over stimulation and eventually convulsions right secondly paralysis if either statement is given in toxic doses then so much acetylcholine will be at neuromuscular Junction that over stimulation of nicotinic receptor lead to dysfunction of The receptors and neuromuscular transmission fail and that will lead to what is that paralysis right and then of course if there is too much cholinergic activity on the cardiovascular system that may lead to collapse of cardiovascular system Amic layer so we have to use it judiciously after discussing the pilocarpine now I will talk about Neo stigma
I told you pilocarbine is a natural compound it's an alkaloid but neostrichment is synthetic pilocarpine was tertiary amine and new statement is quaternary so new statement is more polar compound right but both of them are carba mates they are having carbamate groups now neostrigment neostigmund means no Neo C near CNS no CNS rather we should remember neostragment not to CNS right because it's a very important concept either statement goes to Central number system near Stickman does not for example if there is atropy and toxicity if either statement is better because atropine also produces central nervous
system toxicity but new signal cannot go to central nervous system am I clear is that right so what I'm saying that the major one of the major functional difference between Pfizer statement and near stigma is the physics treatment enters the central nervous system neostigmund does not know to CNS number one thing number two because new stigma is less lipid soluble it dissolved less into fat and most of our autonomic ganglia are embedded in fat so near stigma in action on the autonomic ganglia and parasympathetic neuro effector site is relatively less it is not absent but
as compared to physiostick mean it is less so ganglionic stimulation and stimulation at neuromus neuro effector neglionic stimulation and stimulation at parasympathetic neurofactor site is relatively less new statement as compared to find the statement does it make a sense because it is less lipid soluble is that right another thing which is very important that the best action of new stigma is at the neuromuscular Junction and at the neuromuscular Junction action of neostigmin is even better than physiostagment why the recent research is telling us new statement also work directly on the nicotinic muscular energy receptors so
it means that in case of neuromuscular Junction right not only acetylcholine stresses will be inhibited and acetylcholine concentration will be increased but new statement can directly stimulate the cholinergic receptor at the neuromuscular Junction so it means to enhance the to stimulate the neuromuscular Junction neuros treatment is a better drug as compared to fiber statement did you understand it to stimulate the neuromosphere Junctions Neo statement is better drug as compared to the physio statement is that right but now what are the uses of neostragment before really I go into detail of the uses of near stagman
I want to give you a concept of myasthenia gravis where it is used very commonly right what is a disease called Myasthenia grievas so let me tell you let's suppose this is a nerve ending this is Alpha motor neuron and it is releasing here acetylcholine and here is neuromuscular Junction and what is this thing this is the receptor nicotinic receptor where Estelle choline will bind and here is your friend which Lobster Destroyer acetyl cholines still choline stress is that right now what happened at neuromuscular ejection there are many many nicotinic channels there is a disease
called myasthenia gravis Myasthenia mycena mean weakness gravis mean very grave very serious weakness grave us myasthenia gravis what really happens that unfortunately Auto antibodies are formed it's an autoimmune disease Auto antibodies are formed against the cholinergic nicotinic receptors on neuromuscular Junction so what really happens that r20's bodies bind with these cholinergic nicotinic receptors when these ion channels are bound with the antibodies antibody and iron Channel complex undergoes internalization when it is internalized at the neuro muscular Junction the number of ION channel will be more or less cholinergic kind Channel with less nicotine secondly some of
them will be internalized and others channels even if they are not internalized because they are having the antibody on them can still choline effectively work there no so what really happens that at the neuromuscular Junction antibodies bind with the cholinergic nicotinic ion channels right lead to internalization of iron channels or inhibition of ion channels and then acetylcholine cannot effectively work at the postsynaptic membrane cannot produce enough end plate potentials and muscle cannot be attracted because if end plate potentials are not produced enough then propagation propagating action potential cannot be produced and neuromuscular transmission fails and
muscles will be weak your understanding it reminds me a an old story I think in 1930s there was a medical student and this is a true story there was a medical student and he was having his high school sweetheart they really loved each other and those were not the days when you just go and sleep around right so they they talk to each other they will eventually marry right The Passion of the boys to dance a lot and his girlfriend was really very good dancer but something happened to her gradually she stopped taking interest in
dancing and she started saying she feels a lot of fatigue and N hardest condition becomes so Progressive she it becomes so Progressive that even she find it difficult to walk she will walk few uh steps and then she will feel tired you're gonna understand under these circumstances the engagement was under risk but he was not like most of the boys that medical student I don't know how just by chance he started trying some drugs on her on his girlfriend and one of the drugs which by chance was applied was physostigma by chance he just gave
it to his girlfriend he was trying to give different types of cocktails made of different drugs one of the cocktail was having and you can understand she was drinking phytochragmen and dancing a lot that night and that was when first time we came to know that anticholinergic drug anticolinistration sorry anticolinesterasis can be used in Myasthenia gravis right at that time it was physiostick men presently we don't use physics treatment for that purpose neostigmin is superior because if someone has myasthenia gravis you give physio statement it will go to Central of a system and make some
troubles neo-streamen will remain work mainly on the peripheral part but let's come back and see what is the problem in myasthenia gravis the alternative bodies are destroying and inhibiting what nicotinic receptors and then uh muscles become progressively weak in this condition especially more a person work his physical work more tired he feels is that right now how our drugs work actually neostigmen will come and inhibit what what is this and Estelle cholinesterase when new stigma will inhibit the acetylcholine stages the concentration of a style choline will be more then more acetylcholine will be working on
less receptors but less receptors will throw more cations in and successfully produce the propagated action potential and person power of the muscles will come back is that right so this is myasthenia gravis in which neostragmen is being used presently very effectively right you understand the whole mechanism now another condition is there and there also a person has myasthenic weakness but mechanism is different I'm going to explain a second patient in this patient at neuromuscular Junction nicotinic receptors are normal post-junctional membrane is normal in myasthenia gravis problem was with at the post-junctional membrane The receptors were
having antibodies and they were internalized and they were inhibited acetylcholine was perfectly okay and in myasthenia gravis problem was with the post-junctional membrane pre-junctional membrane was Final okay here there is another disease in which the calcium channels here you know in the nerve endings there were calcium channels unfortunately patient has developed R2 antibodies against the calcium channels which are present on the nerve endings so if this calcium channels are blocked with the antibodies are inhibited by the antibodies then the action potentials when it will come they will produce relatively less calcium and flux because calcium
channels functional calcium channels which are available are less so there will be less calcium going in so naturally release of hastile choline will be less so what really happens here that in these patients acetylcholine releases very less acetylcholine is very less in these patients acetylcholine release was normal now when acetylcholine releases less against stimulation of the post-dunctional membrane will be less and muscles will develop weakness so both of them are myasthenic syndromes this is myasthenia gravis what is the name of this condition this is called a very funny name let me tell you let's imagine
a situation in these two conditions there is some difference I have not told the name I'll tell you later in Myasthenia grava's post-junctional post-junctional membrane has autoimmunity attack in this condition pre-junctional membrane has a problem right this is one thing here muscles are weak there are some muscles are weak but there's one difference here as person physically work more and more he feels progressively worsening weakness here person feels weak in the beginning but with willpower if you work a little he will gradually feel better let me tell you a condition that let's suppose you invite
these two patients at your home in on the dinner this is patient number one with myasthenia gravis and this is the patient number two with another problem and you know they are having some weakness you put very good cooked lamb on the table okay you put the lamp for both of them you are expecting that both of them are very slow is that right but when you start the dinner in the beginning this will be working relatively better but progressively this person will become very tired so what will happen you start eating better and you
feel he's going to take all the land but he will not in the end he'll be just looking to the lamp but cannot move is you understand it and look at that person in that person he will start in the beginning very slowly very very slowly why because he is bringing action potential but little calcium is going in so little neurotransmission he moves very slowly to the lamp But as time passes by he's bringing more and more action potential then calcium start accumulating and eventually significantly more calcium start coming start accumulating and still Cooling release
become better and eventually this person will keep on eating the lamp so this person start better and eventually become very poor performer in eating this person start poor but eventually become better you understand why he become better why because with repeated action potential he will accumulate calcium in the nerve ending and become more effective in religion style colon is that right So eventually this person will eat up the lamp that is why probably this disease is called what is the name of this Eaton Lambert eaten Lambert syndrome Eaton Lambert syndrome is that clear so we
can have myasthenia gravis as a muscle weakness we may have eaten Lambert syndrome patient with with muscle weakness now let's compare and contrast in myasthenia gravis OK first few things common this muscle this patient has muscle weakness and this patient has also muscle weakness this is common here is autoimmunity against the neurotransmission system here is also autoimmunity against the neurotransmission system now we come to the differences here autoimmunity is against the postsynaptic or post-junctional membrane nicotinic channels calcium channels are okay pre-synaptic membrane is okay in this case postsynaptic membrane is okay problem is with the
pre-synaptic nerve ending and calcium channels are having autoimmunity against it is that right another difference is that in myasthenia gravis patients start very poorly but while performing you become extremely poor right you start eating the lamb very slowly and very soon he stopped this person start eating the land slowly but eventually it becomes little fast is that right so lab is written by him little Lambert syndrome mclear the point which I want to highlight new stigma can work on both cases when near statement is given in myasthenia gravis patient a style choline of stress is
inhibited right acetylcholine accumulate in higher concentration and work on the Lesser number of receptors but higher concentration of acetylcholine working on lesser number of receptor may give enough stimulation but in little Lambert syndrome when you give what is that acetyl cholinesterase if it is inhibited by Neo stigmain then what happened even though in Eternal Lambert syndrome acetylcholine is released in lesser amount but because we have reduced the catabolism of Steel choline it will accumulate into normal concentration and normal concentration is enough to stimulate the postsynaptic membrane which is healthy is that right another third condition
where we can choose this drug is and toxicity of tuber curarain you know teamwork you ready this is suppose another muscle and here is these channels what are these channels cholinergic nicotinic channels and here is your friend who is that may be blocking some of these channels Cubo QR e now what happens in patient who has been exposed to cubocularine and muscle that are very weak or paralyzed one way to rapidly activate the muscle is give new stag man if you give neostrigment or related compound it will inhibit what is that so it will inhibit
a steel choline asterisk and a style choline concentration will become very high and it will competitively displace the tubercular in and over activate the remaining channels and person's muscle will start working am I clear so we have talked about three type of muscle weakness myasthenia gravis muscle weakness little Lambert syndrome muscle weakness and muscle weakness resulting due to exposure to tuber curarain in all these three conditions new stigma can work by increasing the concentration of acetylcholine are the neuromuscular Junction and last but not the least I told you in the beginning neostigmin is having a
little activity to directly stimulate the channel the alternative neuromuscular Junction is that right so neostrichment has two number one it inhibits the stralcolino stresses number two it can directly stimulate the receptor so neostigmain is a strong it's a strong indirect cholinergic drug but it is also weak directly acting nicotinic stimulant nicotinic Channel at muscle stimulant right any question here there's no question can you tell me that there's any other use of neostrichment can you tell me some other use of New York statement why don't you tell me that near segment can also be used to
move the bubble and blood Factor sites so to stimulate the bowel and bladder number one you had directly acting cholinergic drug which was methane call number two indirectly acting drugs right and in which you can talk about Stickman and neostrichment is that clear so to if there is a tonic urinary bladder or if there is paralytic Alias you can use the but when we are going to stimulate the neuromuscular Junction the Neo stigma is preferable over 50 statement am I clear any question up to there and what are the side effects of neostrigment very simple
generalized over stimulation of cholinergic system if there's new segment toxicity what will happen there will be over activity of acetylcholine all over the body except central nervous system right so it means Pfizer statement toxicity is more dangerous because it produces cholinergic crisis in the central nervous system also but near stagman produces cholinergic crisis only in the peripheral tissue not in the central nervous system am I clear now we come to another drug pyridor statement pyridostigma and its friends the speed is very important you know many things P for what foreign and another drug which is
related with that and that drug is yes pyridostic mean and it has some other drugs in association with it which are similar mbnomium I don't know from where they find this name MB nomium the speed stands for what P stands for what P stands for prolonged not for other things he stands up for long but if you doxin has a Peridot Stickman has a prolonged duration of action look why those treatment is up to two over Action News treatment is up to two over action parietal statement may work up to four or five hours or
six hours it will keep on inhibiting the enzyme and binomian men inhibit the enzyme for four to eight hours now what does it mean that these compounds are even though functionally similar as fisostrichment and neostragmen but paridous treatment has prolonged duration of action and its related compound and binomium is also for long duration of action due to that reason there are these drugs like pyridostegamen are used more commonly in The Chronic treatment of myasthenia gravis because in case of new statement the causes duration of action is short you have to give more frequent tablets but
in case of Peridot statement you have to give less frequent tablets am I color so this is enough to know remaining things are same but it was treatment is synthetic it is going to inhibit that style choline stresses right and it will increase the transmission at neuromuscular Junction in case of myasthenia gravis even in uten Lambert syndrome right but the most important thing as compared to neostrigment is that it is longer duration let's come back remember learn the fiso stigma well then remember neostrigment is different from either statement because it cannot go to Central level
system Paradise treatment Alpha does not go to central nervous system but as compared to near statement Pfizer Stickman as sorry pyridor statement has a very big P P stands here for long direction is that right now we come to the heterophonia hydrophonium is very phony what is the meaning of phony not funny funny phony personality like to be these drugs but actually it really goes and bind with the receptor sorry bind with the enzyme but enzyme will kick it away within five to ten minutes such action is phony do you think phony personalities are important
in life no they add the some diversity in our culture don't underestimate everyone if everyone is as serious as you are and I am I don't think world will be a place where people will enjoy funny personalities right so what I'm saying adorophonium because it is a phony drug why it is funny drug it's a fake drug it tried to be inhibitor of a style called Industries but a trial is successful only for few minutes five to ten or ten to twenty minute at the max 20 minutes and it is important should I tell you
why it is so important in some conditions even it is superior to Neo statement parado stigma there are some condition where we need our phony friends you cannot take everywhere your serious friends is that true or not there are some situations where you go with your phony friends right let's see our funny drug adorophonium what is the importance of it let me give you a situation if a person come to you listen if a person comes to you and he has strong muscle weakness and you are suspecting myasthenia gravis for example I come to you
and you are my physician and I complain of all those things that muscles are very weak and I do a little thing and I feel very tired and for one or the other reason you suspect I may be having myasthenia gravis one of the way to check that to diagnose the myasthenia gravis is one of the ways that just give me a trial of anticholinar stress drug if you give me anticolinar stress drug and after the drug my power increases it is a good pointer that I am having mercenia gravis you are understanding for example
if your wife makes you very depressed and you are very fatigued then neostrigment will not make you powerful but if you are really having myasthenia gravis and its first time case and you want to diagnose it one of the ways just give a trial of the anticholinistries right and anticolinar stress this will inhibit the you know the remaining story inhibit the enzyme increase the concentration of acetylcholine and even if postsynaptic or what at neuromuscular Junction even if nicotinic receptors are less accumulated Estelle choline will do some transmission and immediately there will be Improvement in power
there are many ways to do it one of the way to do that before giving the drug systemically you ask the patient to do some hand grapes you see how many hand grips you can do it and when he feels very tired and then you give it and you see how good he becomes after that compare and contrast the physical performance and power of muscles before and after the Drug Administration now another question if you are using for example long acting relatively long acting drugs for the diagnosis and if patient is not having my skinny
syndrome for example I'm not having Myasthenia syndrome but I am having weakness so due to some other reason this or that and do you think my muscle power will increase no and then you give another injection still muscle power not but what will happen I will start doing salivation lacrimation diarrhea urination abdominal cramps bronchosphere and if you have done something like this CNS stimulation do you think it's a good thing it will work for six hours do you think so everywhere it's not a serious issue somewhere funny is good ad drop onion is wonderful in
these circumstances why a patient patient come complaining of the weakness you rule out other causes you are strongly suspecting myasthenia gravis inject the first take some for example ask him to do the blinking and when he become very tired these patients start the blinking initially they are rapid then they become slow then they are unable to blank they start looking like this then you give the injection they become very rapid like this it's immediate diagnosis of or another way is a patient happened to be a okay I will not go into that that example okay
they ask the patient to show some Power by the hand grip right and you see after how many events patients become very what tired for example after doing three times he refused to do more you give the injection of hydrophonium you do it thirty times what does it mean right but if patient is not having myasthenia gravis and he develops some cholinergic overflow it will be only for 10 minutes or 20 minutes not for six hours you understand it so do you think hydrophonium is a superior drug or not for the diagnosis of myasthenia gravis
as compared to others so this is one very important use of hydrophonium it's coming with the name of tensilon 10c long we call it tensilon test that we inject the hydrophoneum to a person is that right this is one use of hydrophonium that you do a tensilon test tensalon is the the name by which the hydrophoneum is available in the market right you am I clear then there's and one more use of this phony drug addrophonium let me tell you in some very confusing situations again heterophonium may help you is that right let's see let
us suppose you are having two patients with myasthenia gravis you are having two patients with the Myasthenia gravis and one fine morning both patients come to your clinic they are under your treatment right and you know what is the basic problem in myasthenia gravis patient these channels are yes these nicotinic channels are having antibodies against them is that right now of course antibodies are there and channels are not available for for function this is patient number one and this is patient number two neuro transmission system right you are managing them you have you are treating
these patients by what what is this yes and let's suppose you are treating them these patients by neostrichment right now listen carefully previously when you adjusted the those doses of your new segment with them or parietal statement they were physically performing well but today morning both of them come back to you and they are again very weak you ask them are you taking this treatment this is yes we are taking new segment but still they are very very weak what could be the reason there are two reasons actually autoimmune response against these receptors fluctuate should
you are understanding it Auto antibodies concentration against these channels fluctuates right some few sometimes they are very high in concentration sometimes less they are not stable autoimmune reaction let us suppose this person antibody concentration has become very high now he was taking his previously prescribed dose but because autoimmune attack has been flared up right so now the acetylcholine is whatever is coming and whatever drugs you are doing ah is not enough to activate the muscles so he is having weakness you are understanding me now in this case you need to increase the dose or decrease
the dose of anticholine stress yes you will increase the dose or decrease the dose we will increase the dose this is the case where we need to increase the dose because this is basically you can say under treatment under present circumstances when immune response against these channels has become flared up right it has been increased so the previously prescribed new stigma parido statement is not enough right to relieve the patient from symptoms of weakness because uh more channels are blocked by the antibodies and very little channels are available so we need to we can say
this is myasthenic Crisis this crisis in the patient life will be called which crisis myasthenia gravis has been aggravated myosthenic crisis now imagine the other person this person has come to you he is having my skinny crisis right and he needs to increase the dose or decrease the dose increase the dose of anticholinistrases now we come to the patient number two he was lucky why he was lucky his immune system had reduction in the intensity of attack so it is producing these days less antibodies because in this patient autoimmune attack against the neuromuscular Junction has
been less so most of the receptor have recovered now whatever previously prescribed dose is that is overdose for this person why because acetylcholine which is accumulating here it is working on more receptors as compared to the previous time and when it is working too much it produce what over stimulation of The receptors and make them dysfunctional and muscles become paralyzed and he is also having weakness but this is called cholinergic crisis what it is called cholinergic so you should have a very clear concept that patients who have myasthenia gravis if they are on the treatment
and again they develop weakness it may be due to myasthenic crisis that under the underlying diseases exacerbated or it may be cholinergic crisis because underlying disease has gone so we were talking about my Scenic crisis and cholinergic crisis in both cases patients come with muscular weakness but in myasthenic crisis because antibody concentration and immune attack against the uh receptors nicotinic receptor has increased right so due to that reason there is weakness and in these cases that we need to improve increase the dose of anticholines phrases opposite to that in cholinergic crisis probably either patient has
taken overdose of the drug or underlying disease process has has been suppressed right or has been less active and more channels are available due to that reason the acetylcholine is overworking and due to cholinergic crisis ah muscles are again showing weakness I told you when these receptors are under stimulated muscle become weak when they are over stimulated still muscle become weak now in these cases if you are really confused and you are not sure which patient has myasthenic crisis and which patient has cholinergic crisis because patients don't have it written here and they don't have
these diagrams on their faces so how to know that patient who is who was previously diagnosed as myasthenia gravis patient who has been stabilized on a specific drug with a specific dose and suddenly has developed weakness is this weakness due to myasthenic crisis or is it due to call energy crisis answer is your phony friend will come to help adrophonium you just inject adorophonium to both of them if Myasthenia crisis is the underlying problem you inject the adorophonium right it will suddenly further inhibit the enzymes Estelle choline will rapidly go up and muscle will start
working better so patient power improve after a drofonium right it was which crisis and if after the hydrophonium already a style choline was excessive it become far more excessive and whatever little power he had he is a developed versioning of the signs and symptoms then it was what cholinergic crisis a of course called Energy crises are made worse by hydrophonia but only for 10 minutes or 15 minutes is that right am I clear of course you will be having a antidote with you but the thing is that because adrophoneum is short short duration drug it
can be used to differentiate the myosinic crisis from the cholinergic crisis that so now listen carefully if I'm a patient who is on the diagnosed patient of the myasthenia gravis and I am on the suppose neostratic vein previously I was well stabilized and from last two three days I have developed very serious weakness again and you are really not sure am I having my cynic crisis or cholinergic crisis you will do tensile on test your inject the hydrophonium and C if my power improves then it means that I am under which Crisis myosinic crisis ensure
to increase the dose of near statement but if after the tensile on my power further decreases then it means that I was under cholinergic crisis and my dose of neostrichment need to be decreased am I clear so this phony friend hydrophonium help in two things number one at initial diagnosis of foreign treatment when again they develop weakness during the course of the treatment adrophonium helped you to differentiate the myosinic crisis from cholinergic crisis is that right now again let's go back find the stigma alkaloid tertiary mine can go to the central nervous system near stigma
yes quaternary compound does not go to the central nervous system more effective at neuromuscular Junctions right then peridotic mean long acting anticolinesterase of the same class carbamate and there is another compound what is that or mbnomium is that right any one of these they are having longer duration of action and in the end don't forget your funny friend adrophonium that it can help you in the initial diagnosis of mycena gravis as well as it can help you to differentiate the myosinic crisis from crisis now last but not the least there are some drugs which can
go to the central nervous system and increase cholinergic activity there right but don't act much on the periphery they are used in the treatment of Alzheimer's disease you know Alzheimer's disease there is deficiency of cholinergic system in the central of a system do you know Alzheimer's disease yes Alzheimer's disease now especially there is a nucleus of Maynard right it provides lot of cholinergic stimulation to the cortex right this is degenerated and cholinergic activity and cerebral cortex become less and that reduces the patient's cognitive function patient ability to learn and patient's ability to remember the things
this is the right Alzheimer's disease now they are trying some drug we should go into central nervous system and inhibit the and cooling stresses especially the cholinear stresses here and slightly increase remaining activity of the remaining cholineergic system right the drug which they the first drug we just started using was Tech rind Tech Ryan is that right and then now they are not using it because Techron produces strong hepato toxicity right the other drugs now which are available they are dhoni zappel donate zeppel second drug first for stack line and third drug which is available
reverse stick mean River Ted mean and one more is galenta mine Gallant GLA and T Gallant Amine right so these drugs are commonly used in patients with Alzheimer's disease right and they don't reduce the progression of the disease but they believe at least there is some symptomatic relief any question here yes is there any question there's no question okay another thing when there is severe cholinergic crisis for example sphere called energy crisis may come due to any drug toxicity which can which is directly acting cholinergic drug or toxicity of indirectly acting cholinergic drug or severe
toxicity classically occurs by those anticologies which are irreversible as I told you isoflorophyte or echothyofate or malathione or parathione I told you they are inhibiting the irreversibly they inhibit what anticolinistrases and can produce very severe toxic symptoms which are due to very strong overflow of cholinergic activity in the body so cholinergic overflow of cholinergic activity can be remembered by dumbbells do you know dumbbells dumbbells what are the spellings of dumbbells yes L then again another l wow it's too much L and how many has 2s then L should be one my friend I don't know
why you are interested in 2s else 2s okay dumbbells dumbbell stand for what D for diarrhea okay let me change the right U for yes urination M for meiosis without doubles you can even memorize as I told you that there will be sphere sweating CNS stimulation by cholinergic activity there will be sweating there will be Reclamation there will be meiosis there will be salivation there will be abdominal cramps and diarrhea and urination bradycardia bronchospasticity excitation of the muscles is that right but let's come by dumbbells if you cannot remember by that way B for Bronco
spaz and then B for yes bradycardia I think you people have done some specialization in Remembering this e for excitation of CNS and muscles L for lacrimation as for salivation and sweating sweating and Sally Vision this is very important to remember that what happens to a person when he has cholinergic crisis right again one way is to remember from the dumbbells D for diarrhea U for urination and for meiosis B for bronchospasm B another B for bradycardia right e for excitation of Central of a system and skeletal muscles L for lacrimation as for sweating and
as for salivation or another way is to work from the top of the body to down excessive cholinergic activities central nervous system over stimulation and excitation then too much sweating too much lacrimation meiosis then salivation and with that of course abdominal cramps and diarrhea git then you come down then bronchos passes stay then there is bradycardia is that right then you come further down yes urination whatever is left now muscular weakness right so this is one way to remember or another way to remember but you must know what happens to a person when he has
cholinergic crisis any question okay class adjustments
Related Videos
1:57:49
AntiCholinergic Drugs | Parasympatholytic ...
Dr. Najeeb Lectures
118,902 views

4:11:29
Adrenergic Drugs Part 1 | Pharmacology | D...
Dr. Najeeb Lectures
158,540 views

4:35:34
Thyroid Hormones | Gland | Hypothyroidism ...
Dr. Najeeb Lectures
263,351 views

3:49:35
Antihypertensive Drugs | Pharmacology | Dr...
Dr. Najeeb Lectures
512,825 views

3:14:21
Antipsychotic Drugs | Typical vs Atypical ...
Dr. Najeeb Lectures
255,501 views

1:16:53
Autonomic Pharmacology | Cholinergic Agonists
Ninja Nerd
439,284 views

7:47:08
ADHD Relief Music: Studying Music for Bett...
Greenred Productions - Relaxing Music
11,084,516 views

14:01
What's next for AI at DeepMind, Google's a...
60 Minutes
204,878 views
3:56:09
Adrenergic Drugs Part 2 | Pharmacology | D...
Dr. Najeeb Lectures
163,331 views
![Upbeat Lofi - Deep Focus & Energy for Work [R&B, Neo Soul, Lofi Hiphop]](https://img.youtube.com/vi/THh4fT0O7IY/mqdefault.jpg)
3:22:29
Upbeat Lofi - Deep Focus & Energy for Work...
A Lofi Soul
672,180 views

4:31:14
Antianginal Drugs Pharmacology | Dr Najeeb🩺
Dr. Najeeb Lectures
114,350 views
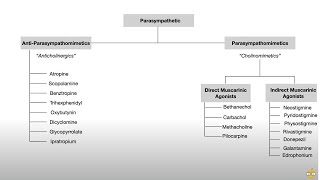
33:57
Autonomic Nervous System (Pharmacology, Re...
Dirty Medicine
661,253 views

1:29:35
Music for Work — Deep Focus Mix for Progra...
Chill Music Lab
3,889,093 views

3:36:46
Gastrointestinal Motility | GI Motility | ...
Dr. Najeeb Lectures
193,935 views
1:39:58
Diabetes Mellitus | Types of Diabetes Mell...
Dr. Najeeb Lectures
137,833 views

1:45:41
Autonomic Pharmacology | Adrenergic Agonists
Ninja Nerd
345,998 views

3:03:35
Diuretics | Pharmacology | Dr Najeeb
Dr. Najeeb Lectures
1,158,146 views

44:05
Autonomic Pharmacology | Muscarinic Antago...
Ninja Nerd
179,858 views
2:48:55
Parkinson's Disease | Alzheimer's Disease ...
Dr. Najeeb Lectures
73,185 views

1:59:15
Autonomic Pharmacology | Adrenergic Antago...
Ninja Nerd
184,398 views