A 20-Minute Call with My Posture Coach
244.1k views3502 WordsCopy TextShare

Bryan Johnson
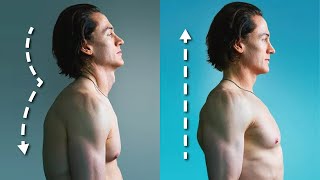
My posture coach Kjetil Larsen walked me through some exercises for proper neck and back posture.
...
Video Transcript:
hi everyone I have a special treat for you today in this video my coach kahita Larson is going to coach me on the exercises I can do to improve my posture he's going to show you the anatomy it's technical but I promise it's worth it okay he tell nice to see you likewise Brian good to see you as well okay he tell and I met about a year and a half ago we were working together because I had a a whole body MRI and we had a few people look at it and everyone gave a
clean bill of healthy analysis but then we took it to kahiti and we said hey here's my MRI uh what do you think and kehito found a few things in there that were concerning specifically he said that I had uh some internal jugular vein stenosis so the the pipe inside of my neck which is responsible for blood flow out of the brain he identified on the MRI that I had significant stenosis and that was potentially causing all kinds of other problems in my brain including my white matter hyperintensities and pressure increases and it explained a
bunch of symptoms I was having such as headaches uh at night piercing headaches and so kahita was the only person that was able to piece together from this scan what uh the symptoms I was having and not even realizing I myself was having a problem so I remember telling you that what are the consequences of this long term this we're still in early stages in research there can this have an influence on the development of various craniological disorders such as early dementia for example and I would say it's plausible and I know that many share
that that view so even though you weren't suffering per se but you were having some headaches a little bit of brain fog stuff like that we started working on that together with Oliver and well we we had a pretty good result didn't we we had a fantastic result we corrected the entire thing so once kahito identified this and we started getting additional measurements to quantify what really was going on we looked at intracranial pressure with eye measurements we did not do a puncture at a lumbar we decided that was too invasive for the situation but
we did extensive eye measurements and then uh we had a we talked to a bunch of experts on what they would do we looked at some surgery surgical options to fix it yeah and he said actually no I think you can solve with posture changes and this was the first time in my life that I had ever dedicated attention to posture no one had ever taught me posture before and so nikahito and I started working together on a weekly basis he showed me a few of these exercises and uh I was skeptical the posture alone
was going to be powerful enough to correct this as I went into it with skepticism but he told me in about a six to nine month time frame uh if I followed his protocol I would and that resulted in me being uh constantly aware of my posture because I had such significant risks to me of impeding blood flow from my brain I didn't want to jeopardize that so I became um it became my non-stop focus of trying to maintain the postural positions that kihito has now in doing blueprint a lot of people have expressed interest
in posture so this is not a video about posture generally if he tell and I working together to try to fix my internal jugular vein stenosis all right so can you tell a lot of people have asked me uh you know about posture and of course my entry point into posture was entirely around fixing this internal jugular vein stenosis so maybe what would be useful is if you and I just did a session uh where I I did the exercises you prescribed to me uh which helped me build the muscles to maintain the posture and
then uh we we basically showcase posture uh as through our exercises together let's let's talk take a few minutes guys I would like to do that with your permission take a few minutes and talk about why is this important because it can sound almost too good to be true and I think that a lot of naysayers will say no it's not possible to improve cranial venous drainage with posture well yesterday there was a study done in 1998 by some famous neurosurgeons siwani and Rhoden and they were looking into why so many of their patients were
having hemorrhages bleeding in certain cranial certain positions and especially a position where they were opening up the skull from the back like this with the neck extended a lot of patients were having hemorrhages and they did a caliber study were very they opened various categories and what they found and what they postulated was that when you bend the neck back like this which is a common posture for a lot of people they kind of sit like this and and that neck back you blocked the jugular veins and that was their theory on that now in
the subsequent years it's not a very popular topic because it has more to do with chronic pain and chronic Melodies which is not a very popular Topic in medicine in general but various papers have come out and been talking about the prevalence of internal jugular veins compression stenosis as a potential contributor to obviously cranial venous hypertension but also CSI fire potential so the typical its role in the typical development of intracranial higher potentially conventional um problem which is a cerebral spinal fluid hypertensive problem and where I came into this is that I had a lot
of patience with migraines headache fatigue they could have vestibular problems this is vertigo and a common denominator that I saw I'm not going to say that this will fix everything but a commonly dominated I saw was this posture and as I got into vascular ultrasound I started measuring internal jugular veins and research shows that normal flow rates are approximately between 700 and 1200 milliliters per second sorry per minute both jugular veins combined and I would often find that patient could demonstrate as low as 200 300 and the lower those total numbers were commonly the worst
of patient's symptoms were as well when we go through what you and I did for the PT exercises and we can just do an exercise then people can just repeat this as they watch if you uh if you permit I would like to explain why this works instead of just showing you some exercises would you like that okay okay I really like explaining mechanisms because it instead of just saying that this is how it is let me find a couple of pictures here so some examples so like I already showed you in the MRI it's
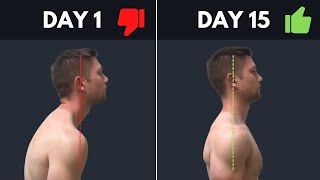
not so easy to see for Layman I guess but like I showed you in the MRI what tends to happen is that the c0 or the head Glides a little bit back on the C1 and then the C1 Glides a little bit back on the C2 the faster there's a famous neurosurgeon called Atul guel I'm not sure if I pronounced that correctly it's an Indian University and very famous in the in the government community and to the best of my knowledge he was the first person to to identify this because when you look on MRI
in what we call the medium plane medium Satchel plane where the cranial cervical Junction is it's not this it's not really visible there but you go out to the side and you look at the facet joints and that's what I showed you you can see this I call it accordion-like retraction you see step by step retraction of each each faster joint now how are we supposed to if each step is back how do we fix that well the first thing we do not do is that we do not try to correct forward head posture which
is a common fallacy because if I try to pull that head further back it will get worse of course but it will because it's already too far back because what people do is that they hinge on the neck and look at my neck they hinge on the neck and the head back do you see that so although the head might appear to be forward they're actually hinging back on the neck already and as they try to pull that further back it gets worse not better so we would like to reverse that and we do that
by making I got this from a guy called Evan osar initially when you make the neck long not back you pull up and you can just imagine when I pull up the head the neck lengthens but my hand actually goes a little bit forward and when you do that this activates both of the important deep neck flexors there are three main steps here the number one is the partial component and like I said you don't want to pull your head back that will make it worse that can also make other things worse what you want
to do is that you want to utilize the minimal effort you don't want to tense your neck up you want to utilize minimal effort and pull the back of your head up that will also involve your head coming slightly forward that's fine that doesn't matter that's completely fine that's step number one it's very important to as certain and you remember maybe Brian we had this we talked about this because a lot of patients when they do this make them such a an amount of effort in the beginning that they kind of clench to stay there
and patients who have that habit from before they can they can do this without it being visible so you're not going to see them doing this it looks perfectly fine but they're clenching to stay there and the problem with that is that it's very treacherous because although it looks good it makes you worse so what I like to do then I like to have a third person do a slight torsion on the patient's neck and this is what we did with Brian as well I think it was resistant to help you out with that with
when I have someone in my office I put them in a position and then when they're not expecting it they cannot expect it then I just try to turn their head a little bit when I'm not expecting it with I'm not twitching it because then it will reflexively tighten up so I just come in and just without them expecting it try to turn them and if there's resistance it means they're clenching to stay there so you have to kill them to stop doing that so they want to employ minimal effort to stay in beautiful posture
and obvi often the more prominent your Adam's apple is and the less conspicuous your Chinese the worst it is you can just and it looks better as well you can probably see a difference between this massive difference aesthetically as well the next step would be the sub occipital exercise the sub box both the suboccipital and the levator scapula exercises have a requirement of the long neck posture while you perform them the Atlantic simple joint is mainly an extension flexion pivot joint it has about 30 degrees of motion this is also very good to do for
whiplash patients so you have the patient first have a long neck and then you put some pressure on on pushing downwards on the forehead start with your chin down and you go up about four about 30 degrees if I go further than this you can see that's that's neck now my entire neck is extending rather than rather than just that upper uppers Atlantic simple joint then I'm going to be doing this and that's not correct okay so that's the exercise for the suboccipital muscles now for the levator scapula which like I said is it should
must not be be be forgotten here it's extremely important extremely important you want to be performing now let me just capitalism it's mainly considered an element of the shoulders which is kind of isn't kind of not the way to scalp is mainly a horizontal stabilizer for the shoulders so this the trajectory of pull for the levator is pretty much this direction attaches to the superior angle of the scapula and therefore it pulls the scapula this way here's where it gets a little bit more technical because the two main ways to move the scapula and this
has to be right to get this muscle correctly if you have your arms a little bit in front of you this will encourage what we call upwards rotation and that will almost entirely disconnect elevator so we want downwards rotation which tends to be viewed as bad scapular positioning that's what we want for this so we put the elbow backwards you can see my shoulder blade points forward in the trajectory that I wanted to whereas it points backwards to see that's when I pull forward that's a clue so I put my elbow back my wrist back
neck long and I pull towards my nose with this trajectory all the way forward and slightly up and like I said the trajectory here is mainly forward and slightly up if I pull mainly up I will get the upper trap generally good as well but it won't it's not what they're looking for here if I pull four of them down I'll get the pack Miner definitely not what we want so this is the trajectory you're looking for and I'm not sure if you can see that maybe you can maybe not but gonna see the muscle
popping out yeah how about this okay so I'll do a few of these exercises and you can coach me as you did before well what you want to do first let's look at your posture first let's do the posture first okay and what we can see here is that the Adam's apple is not so prominent he used to have an extremely prominent Dom sample there's a very cleanly clearly delineated chin and jawline that's what you're looking for here he's not pulling his head back neck looks nice and long I don't know if you're able to
use your right hand Brian and pull pull some of that hair up so you can see a little bit more of your neck is that possible you can see there very nice and long neck the chin this is just fine but the chin could be a little bit tighter but it was fine it was fine you just don't want it to be strained too high or too low so anywhere in that middle middle Escalon is fine this is very nice and then we just try to twist them and make sure he's he's not clenching which
I know he's not yeah now then for the for the um for the suboccipital exercise do you want to do that first yeah okay uh yeah this guy yeah this guy yeah so when I prefer for the suboccipitals the specific sub-occipital I prefer to put the head the weight on the front now normally here is good to use both hands if you have the strength for it to alternate between the two but due to view here we're going to use your right arm just due to view all right you will be continuously pushing down with
your hand with the five well this is individual guys but in Brian's case probably at least five parts of force at least not much more than that and you and you can see here you it's two it's two a little bit too aggressive Ryan you're going too high there we go and yeah perfect there you go there you go excellent this one is really tricky it might not look so hard but it's extremely tricky to do and especially if the now in Bryan's case he knows how to do this but a lot of patients they
are not able to maintain that long neck position or they use too much force to stay there and it's very hard to do this exercise for them without clenching their neck because we want to do this with minimal Force minimal Force that's beautiful Brian well done good now let's move on to the uh let me try it scapula in your case you're in such great shape that we should be able to perfectly see the anatomy here so I have that I have these 20s 20s might do for Mo for 99 of people it will be
way too much I I tend to use an eight pounder when I do this in clinic now for you this might be appropriate when I do this I I hold a barbell behind my back but I would never do that with a patient now you've been doing this for year Brian so we can try but we can try with the 20 we can try let's see what it looks like uh but for the absolute majority of patients we want attraction both of those elevator at the same time now here's the thing guys you want to
pull with the shoulders not with the wrist so you pull you hold your wrist back neck long and you pull your shoulders up and forward and that looks better than I expected actually because this is very this is very heavy you know so I have no other patients doing levator exercises with uh with this weight up and forward up and forward beautiful beautiful beautiful all right the only thing I would like to add there now you know Brian in this case is not a very vulnerable candidate here but for a lot of patients who are
going to be doing this they should be careful in especially in the back part because when you put when you pull your scapula back and you let it come down the collarbone will pinch into the brachial plexus and chronic pain patients which are my typical Patient Group they are very sensitive to this whereas Brian is not so sensitive to that so just be aware of that guys I tend to recommend I do recommend that we stay a little bit elevated from the start start and stop in that position and we pull up and forward so
when we go back to the starting position we never go back and down we just go back so if you don't Ram that collarbone into the brachial plexus that but that was a beautiful presentation right well done excellent thank you you were a great coach I'm I'm glad I haven't we haven't had a session in some time now so I was worried today that my technique was kind of always got to be trash yeah but you know that we haven't talked because you're feeling great and that's how it should be that's how it should be
right all right cool can you tell I I think we can wrap on this uh this was this was fantastic I I just so deeply appreciate you uh for solving something no one else could solve and you you corrected it and I got I got to move on with life and now it's just the permanence of who I am so thank you very much I I just thank you so much for that I do just want to say this one thing so I don't so I'm not you know taking the credit from everyone that there
are people that came before me who do surgical approaches for this and do a great job with that just want to be crystal clear about that for example Nicholas Higgins and a lot of these patients need surgery whereas you didn't so uh thank you so much for that Brian and you know congrats with the great results you had you really worked for it and you deserve it thank you great to see you likewise have a great night thanks for watching everyone if you want a shorter five-step guide on how to improve your posture click on
this video
Related Videos
5:35
How I Fixed My Terrible Posture - 5 Habits
Bryan Johnson
3,455,208 views

10:28
How To Correct Your POSTURE & Increase You...
CHRIS HERIA
3,398,191 views

1:00:41
Challenging Bryan Johnson On His “Never Di...
Doctor Mike
1,509,600 views

29:11
Does Bryan Johnson’s $2m biohacking routin...
Freethink
4,472,570 views

14:07
I Wasted 2 Years Trying To Fix My Forward ...
Waughfit
367,815 views

17:43
Why You Should Be Eating Garlic EVERY DAY!
Talking With Docs
23,108 views

11:56
Secret Service Agent's Brutally Honest Opi...
The Diary Of A CEO Clips
1,243,377 views

10:18
My Anti-Aging Skincare Routine
Bryan Johnson
672,136 views
7:24
Why This Doctor Is Trying To Sue Me
Doctor Mike
4,063,257 views

10:12
How I FIXED My Terrible Sleep - 10 Habits
Bryan Johnson
1,578,047 views

10:40
BEST sleeping position to FIX Neck Hump, H...
Dr. Jon Saunders
11,122,591 views

9:46
How to Fix Forward Head | Slumped Posture ...
ATHLEAN-X™
4,422,402 views

20:03
“I feel like I’m 25 again” - Dana White’s ...
Bryan Johnson
675,317 views

19:52
Why you’re so tired
Johnny Harris
2,473,253 views

13:06
HUGE Magnet VS Copper Sphere - Defying Gra...
Robinson Foundry
1,417,325 views

1:09:40
Most Extreme Anti-Ageing Routine: How To S...
Live Well Be Well with Sarah Ann Macklin
20,016 views

33:45
Can She Survive My $2,000,000 Anti-Aging R...
Bryan Johnson
957,523 views

10:58
3 Reasons You Have LEVATOR SCAPULAE Pain (...
Precision Movement
250,367 views

5:16
Correct Your Posture in Just Minutes!
Dr. Eric Berg DC
1,086,149 views
9:56
SUPER SIMPLE & Effective Fix For Rounded S...
Conor Harris
137,019 views