Bruce Ecker on Memory Reconsolidation in Psychotherapy: Effective Unlocking of the Emotional Brain
29.85k views13661 WordsCopy TextShare
Psychotherapy Expert Talks
► 𝗩𝗶𝘀𝗶𝘁 𝘁𝗵𝗲 𝗽𝘀𝘆𝗰𝗵𝗼𝘁𝗵𝗲𝗿𝗮𝗽𝘆 𝗲𝘅𝗽𝗲𝗿𝘁𝗶𝘀𝗲 𝘄𝗲𝗯𝘀𝗶𝘁𝗲: http://dpfortherap...
Video Transcript:
first of all thank you so much Bruce for being with us I'm glad to be here thank you for the invitation so we have a lot to talk about from your book unlocking the emotional brain your interest in memory Rec consolidation coherence therapy I'd still like to know a little bit more about you first and I know that you work as a research physicist for 14 years prior to being a therapist can you tell us about that yes ah what to tell I was drawn to physics very strongly uh because I uh I wanted to
see into the um the the heart of existence to be honest I just had a a strong craving to see into the the essence of reality and I became a physicist and uh worked in a laboratory for 14 years as you said and I enjoyed the work and learned a lot about myself and Life and Science and doing that and you know published and did good research and all of that but it turns out physics doesn't quite really reach into the heart of existence it reaches Into the Heart of complicated mathematical model that's what and
you don't quite ever touch reality so I um made a big shift after uh about 14 years and switched into uh the subjective approach rather than the objective approach to knowing what's real and uh my interest in the subjective side of things led me to being a psychotherapist how did this happen this transition it took quite a few years uh I was working as a physicist and looking for what what's the other what's the where do I want to land what do I want to do instead I knew that it wasn't going to be physics
and it took me well probably close to six or seven years to settle on Psychotherapy I looked into it I think three different times and on the third time it it landed as a yes the first two times it was no that's not for me I don't want to have that responsibility I don't want to be in that position and the third time around it all came up green yes and I uh went to graduate school and here I am now it turns out to be um actually much more what I'm built for did you
have any did you have any personal experience with Psychotherapy yeah and that had an impact yes I uh I went to physics graduate school uh at the University of California Berkeley and that was in 1968 that I went to Berkeley right in the middle of the hippie era and the Vietnam War and the and especially the human potential movement sure andol therapy and encounter groups and I got very involved in that for my personal growth and that really opened my eyes did you get a chance to go to like the slan Institute and yes yes
and it was a remarkable time just an amazing mind openening time for many of us and that got me deeply involved in inner awareness and growth and what you know the possibility of change and yes so I had experiences of change that years and years later when I chose to train in Psychotherapy my own experience that deep profound change is possible yeah uh guided me on what what types of therapy to train in and what was this by the way what was your main like interest in the start in terms of therapy it was a
a combination several several parallel interests uh certainly gestal type humanistic experiential focused work and the uh the constructivist approach yeah uh was was profoundly exciting and meaningful to me um uh Gregory Bon's work uh the mental research institute's work the book Chang by watler weakland fish had a major impact uh also Carl Young's work his recogition of the coherence yeah of the unconscious mind was a primary influence very interesting and then I had a mentor uh a psychiatrist named Robert Shaw Robert Shaw uh under whom I trained in my internship in my graduate program and
he had a constructivist approach that emphasized the possibility of Rapid restructuring of the underlying constructs maintaining a given symptom yeah and so that all the combination of all the things I've mention mentioned M just put me on this track of looking for really uh it was it was a quest to extend the constructivist approach of the time which was uh really an avoidance of in-depth work there was a big reaction to Freudian and psychoanalytic uh type of therapy and there was a lot of avoidance by the way the systemic therapies also were a major influence
at time tremendously um explosive growth in the I understand you're a marriage and family therapist licensed right that's my license yes in the state of California that was the most practical track for okay okay so but it allows a much broader scope of work than than only marital and family so I do both individual work as well so yeah um I I met uh Laurel Holly uh in those early years the the mid 80s and we shared sensibilities and interests and together we set out as we began our practices to to um uh extend the
constructivist uh approach the solution oriented and strategic approaches which avoided in-depth work well I had experienced indepth rapid transformational change by accessing deep material so I wanted to pursue this possibility of extending the constructivist idea to the depths uh you know how do you get to the deeper implicit constructs that are operating to to guide transformational change efficiently and that was our Quest you know that's what we set out to do and so we L and I we would study our uh session that happened to produce deep lasting shits we didn't know how to do
it reliably but whenever it did happen we studied those sessions very intensively to find what were the key ingredients that had brought it about we did that for quite a few years across many different clients and types of problems and finally did identify a certain series of experiences that was always present yeah leading right up to a a powerful shift happening sewing you down just a little Bruce so I I think from what I understood this is roughly between 86 to 93 right right right so tell me something in this era what are you exactly
doing are you like uh watching audio or videotapes how did you actually go about doing this research uh we were studying our own sessions while also training with various you know uh gals systemic constructivist teachers and trainers and and reading voraciously you know these wonderful uh expansive Progressive new approaches that were developing so uh we took into account everything we were learning and examining our own sessions just to find what are the key moments and the key interactions what did the therapist say or do what did the client say or do that led up to
these moments your uh physics sensibility did it help in any way with this research it did it definitely did I think I brought my physics approach into this uh process to to uh ex just examine examine the without without theorizing without bringing preconceived ideas just examine the phenomenon itself and look at it from many different angles yeah until a pattern emerges yeah you know the pattern that connects I think was one of bateson's fundamental ideas and and also one of his ideas was uh identifying the difference that makes a difference you can you can create
differences of all kinds like identifying the difference that creates a fundamental change in the system that's what we were doing by examining our own sessions uh to see what what was the the immediate cause of transformational shifts and we did identify a certain sequence of experiences and we began to reorganize therapy about or around uh how to bring about that sequence of experiences from the very first session of therapy and let go of everything else we had learned and just head for that sequence of experiences and that did begin to increase the frequency and consistency
of creating uh true therapeutic breakthroughs last you felt this in your own practice Yeah observed it you observed it constantly when clients say I'm not depressed anymore even when I visit my parents or I don't have panic attacks anymore even when the same situation happens so it's like we're on to something here yes we're on to something here um yeah we weren't basing this on our own uh gratification of ideas that we had this was you know very concrete observation evidence of Effectiveness uh and uh then the the U for me I think the most
remarkable thing in the whole development of our careers was uh finding in for me it was in 2005 when I came across the memory reconsolidation research and began to read about the sequence of exper iences that had been identified in the laboratory research that literally unlocks the neural encoding of a of a Target emotional learning yeah it was the same sequence of experiences we had identified and had written about in our first book 1995 depth oriented brief therapy well you know that was just hitting the jackpot we now had neurological evidence that the the the
method techology we had found had a rigorous basis in the brain so what you're saying is that to recap in I think it was in the Thanksgiving of 2005 right very touched by how you read into the the personal story here I'm a fan Bruce I'm a fan well but but yes yes it was you you confirm basically what you already finding out in the '90s yes yeah so tell me something so if you don't mind me jumping right into it one of the things that I found most interesting one of the golden rules kind
of that you found was the idea of not trying to get rid of the symptoms of the client not counteracting could you talk a little bit how we found this out how it evolved this idea yes that idea evolved as one of the patterns we finally recognized by studying sessions that did produce transformational change noticed um uh one of the critically required experience arrive the transformational change was was facilitating or shall I say ushering or bringing the client into a direct experience of the underlying emotional learning the schema the constructs that had not been conscious
but uh uh by becoming conscious by the client uh feeling and knowing what uh meanings or expectations or model of how the world Works uh or schema was operating that was necessitating or driving the the production of this it was when clients had had a direct experience of that had shifted it from implicit knowledge into explicit knowledge not just as a cognitive Insight but as a whole body uh uh experience and Lucid recognition of emotional truth that was one of the key ingredients that set up transformational change and when we recognized that we realized uh
counteracting is the opposite counteracting is an attempt to get away from what's causing all the trouble and to set up a preferred experience for example what's a common relaxation techniques teaching relaxation techniques to reduce anxiety is a I think a good example of counteracting um well what turns out to be the direct path to transformational change is the opposite of that where you don't try to get rid of or even diminish the symptom you aim for revealing and having the client experience what inside the client is actually important step toward a transformational change yeah well
let me play a little bit of Devil's Advocate Bruce which is this idea of not getting rid of the client symptoms not having a counteractive stance yes imagine clinicians uh hearing us and they work with what so-called personality disorders clients very extreme clients maybe self harm behaviors this kind of thing would you still uh recommend this uh stance of noncontrolling non anti- symptom or do you think that there are some basic conditions needed to do this stance yes yes good question and that's a very important Point yes of course uh always safety first so counteracting
is sometimes the necessary and right thing to do to arrange for safety and even when it's not a matter of safety um it can also be the necessary and right first thing to do for clients who are in such intense distress that their functioning is seriously impaired so using methods that can uh bring about symptom relief counteractive methods that help reduce the symptom uh is totally appropriate than even necessary or urgent in such cases and having that then you can move on to the stance you were speaking yeah yes yes yes what the point is
I think that uh it's important for therapists to know that the counteractive work even though it may be strategically necessary in such cases is very unlikely to bring about lasting deep transformational change a true therapeutic breakthrough could you link this maybe we could Define a little bit better what you mean by emotional schema or implicit learning could you tell us a little bit about that sure I think maybe U some examples might make that yeah thanks clear very clear so um therapists are actually very very familiar with emotional learnings and schemas even if they don't
think of it in those terms for example um imagine working with a client and what the client brings into awareness finally and finally verbalizes uh comes out in words sounding like this um if I feel and show any sadness or hurt or fear I'll be attacked and humiliated so I've got to block my feelings yeah okay just that much you know many therap ists work in a way that accesses and reveals that kind of material so I'm calling those we call those emotional learnings because they are learned expectations when you look at what they're made
of they have this uh form or structure that cognitive scientists call a schema yeah uh there's a vast body of literature and experimental results indicating that the brain self-organized its learnings its knowings into modules coherent modules multicomponent modules that we call schemes and this specific part seems to even take place in CBT they talk about the conditional rules and how they are present SCH yeah there are several different Therapy Systems that conceptualize in terms of schemas there's a therapy called schema therapy Jeffrey Young yeah Jeffrey Young therapy which I think is a is a evolved
out of the CBT framework mhm we had no uh familiarity with that as we were developing our approach arrived at a focus on schemas um from a very experiential aspect and uh with no counteracting no attempt to oppose or correct a schema we don't view uh these emotional learnings or schemas as incorrect or irrational we view them as coherent they make sense they make sense in in relation to what the person actually experienced and learned they make complete sense and so we even named our our therapy system coherence therapy that as the central principle so
that's an example of an emotional learning or schema yeah another is um U and these schemas don't exist in words or in awareness and yet remarkably they are very well defined and specific which becomes apparent when finally the client does uh attend to them and put words on them another example is um the only way to get any attention is to do something really bad right some some people have that one a close a close cousin of that A variation on that is um the only way to get any caring attention is to be sick
or to be VIs unwell and struggling MH that's a schema that's not too uncommon learned helplessness is what's in that so and and connecting this to your constructivist background this is all not declarative knowledge so when they put when client puts this into words it's already symbolizing something more implicit that's right it originally it's implicit it's amazing how human beings learn many many very specific knowings that are life organizing and life shaping with no awareness yeah of the specific learnings or that any learning is taking place and these learnings then are experienced as if this
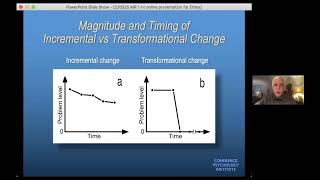
is the truth of the world when it's actually constructs and models and expectations that one has formed on the basis construing yeah that one has formed on the bis of specific events and experiences on your book unlocking the emotional brain you have a quote that I love which is emotional memory converts the past into an expectation of the future without our awareness yes precisely yes whoever said that really knew yeah quite a smart guy yeah so maybe you can bridge this you just said with your distinction that I find interesting between incremental change and what's
called it deep change how do you differ these two yeah yeah well we we we I think I think extensive clinical experience I know in all of our experience it's it's consistent that when when you when you try to build up when your therapeutic strategy is what we call the counteractive strategy trying to build up preferred patterns of behavior or mood or thought uh or even preferred somatic patterns there are approaches that uh try to induce change by changing sematic patterns posture um these tend to create new learnings that get set up separately from the
existing implicit emotional learnings that are driving symptom production and these new preferred learnings operate in competition with the existing problematic symptom generating learnings and can uh regulate the problematic learnings and can suppress uh symptoms to a degree uh seldom completely eliminate symptoms and seldom avoid symptoms in a stable robust manner usually what one finds is that uh the the the existing symptom generating learnings can get re-trigger by circumstances that are a strong enough cue or trigger and the symptoms relapse yeah so counteractive therapy the strategy of counteracting by building up preferred competing learnings or knowings
uh has this quality of of U producing partial symptom relief which is what I what we mean by incremental change just degrees of symptom relief that aren't very robust can tend to relapse you have to then reapply the counteractive alternative techniques or practices so there's an endless effort required and I think really you're you're setting up an increase of What's the phrase Rd Langs phrase The Divide itself divide itself yeah you're setting up an end conflict or or opposition inside the client so you gave the example of the sorry of the relaxation skills for instance
so you're always just trying to Trump over whatever is yes with real ex exactly yeah exactly yeah and in contrast to that the other major type of Change transformational Change uh aims to bring about a fundamental um U well we're talking about symptom producing schemas as emotional learnings a fundamental unlearning yeah the strategy is to bring about a direct uh uh uh unlearning and nullification of the specific emotional schemas that are driving symptom production and when that occurs U the then then the vender change is robust and Lasting and we do observe total symptom sensation
in that case and there are observable markers that that we use uhu in fact the same markers that the neuroscientists who study memory reconsolidation use to confirm the Eraser of the target emotional learning in other words the the true unlearning and nullification of the target learning yeah in a way this could be like our outcome measure this kind of verif yes yes that's what we use as the outcome measure and it consists of three components yeah uh the the symptom no longer occurs in any of the situations where it used to occur doesn't occur at
all you know if you're thinking in terms of the the sud's 0 to 10 scale you're down to zero it's a convenient way to do some of this say zero yeah in addition the emotional activation that the schema had had created that that altered state uh some therapists think of this as an egate or a self State uh that that bodily activation that the schema produces is also uh no longer occurs at all yeah so the S the expressed symptoms are gone the emotional activation State associated with the expressed manifested symptoms are gone and the
client also reports that those two changes are are effortless yeah there's there's no there's nothing being done to maintain them yeah or it's just spontaneously disappear it's just how the client now is yeah and that persists on and on and on over extensive time and in all the situations that used to produce the symptom those are very clear distinctive markers and it's usually very straightforward uh and easy to to um elicit that information from the client yeah so I guess we have the duty now to spell out the steps of memory consolidation right yes everyone
is hearing us P this is too good to be true at least give me the formula it seems too good to be true I know it does I know it does but you know since the 1990s maybe the late ' 80s therapists are more and more familiar with therapy that that that have this kind of result um EMDR has this kind of result um uh uh dick schwarz's approach U family systems therapy can have this kind of result um there there are quite a few therapies that describe this kind of result so it's it's at
at when we started with this in the late 80s and started teaching it in the early 90s it was credibility a problem wasar that therapy can be this effective but I think it's becoming more and more so all right the actual steps all right the neuroscientists have identified a series of three steps a sequence of three experiences that's that's an important Point um uh some some clinicians and researchers who are looking at how to translate memory reconsolidation research into clinical uh use focus on concrete procedures but I don't think that's the most Illuminating and effective
uh point of view um what what I see in the Neuroscience research is the identification of a sequence of experiences and that's also what matches what we found in the late 80s that we that we wrote about in our first book and the sequence of experiences is this first the client uh experiences a reactivation of the target emotional learning that's producing The Unwanted symptoms so for in relation to the examples I mentioned earlier the client would be uh uh having an affective experience of the only way to get any attention is to do something really
bad for example and therapists many therapists are quite familiar with how to reactivate a schema you simply invite the client to focus on certain cues that are very Central to the schema uh it's simply a matter of for example asking the client uh can you can you remember a time when you were a boy when you were feeling that need and that ache for attention and you weren't getting any attention you had you had so many brothers and sisters and your parents hadn't paid attention to you for days you told me can you bring that
to mind and kind of revisit that yeah yeah okay yes you're feeling it yeah do you feel it in your body yeah where do you feel it oh I feel it here and here good now try saying those words we found and see if it fits the only way I can get any attention is to do something really bad now yeah client says it and yes that feels so true okay so there it is the schema is re activated as an embodied emotional knowing and feeling good the second required step to uh launch the memory
reconsolidation process now is for the client to have an experience of uh of any kind that what the the the researchers call this a mismatch experience or a prediction error experience it's an experience that is a direct knowing that wait a minute reality isn't as expected by this that by this emotional knowing in this in our example the only way to get any attention is to do something really bad um for example this could consist of reminding a client of something I had heard about from him searched for and found from him do you remember
the time your wife U set up a surprise birthday party for you and you came home and all of a sudden here were all these caring friends focusing on you giving you so much caring attention and you didn't do anything bad to to deserve that or make that happen uh did you and the time your boss called you over and talked to you about something that was important to you uh and and you needed that conversation you didn't do anything bad to attract his interest and attention so you've had these other experiences where you received
caring attention without doing anything bad okay just bring those to mind right alongside this living emotional truth from your childhood that's step to a mismatch experience yeah uh a direct knowing that's very real to the client that sometimes reality behaves very differently than this original emotional learning expects in the in the moment of having that mismatch experience what we call in therapy a ju to position experience because we're inviting this strange both at once experience where the original learning feels very real to the client and at the same time this other experience that contra icts
that also feels very real both at once it's a strange edgy experience kind of similar to cognitive dissonance but this is a very fully experiential version of that not just conceptual yeah sorry to interrupt you Bruce just to make this contrast with original cognitive therapy because it could be perceived I imagine wrongly but you can spell out the difference uh that this is bringing out the evidence that reality is different from what the client is saying so let's just re re-evaluate the evidence it is that it is that um but it's done experientially yeah it's
not done as a cognitive insight as if intellectual knowing should manage to uh override emotional knowing so this can is fundamental this experience it's fundamental in guiding A J position experience and this is is important I'm so glad you asked that uh the way we teach this process the therapist says nothing and does nothing to indicate anything negative about the the original emotional learning there's no indication that this is incorrect or invalid or should be gotten rid of it's an an empathic acceptance of both the original knowing and this other which the therapist did not
introduce as a corrective at all it comes out of the client you know in the the example we're using I ask that man tell me has this has this this learning that only doing something bad gets you any attention has that always been true throughout all of your experience or has anything ever happened that seemed different and once the client is explicitly aware of this schema the exceptions the experiences where a disconfirmation happened come right to mind when asked about that yeah and make an impact make an impact yes the J dep position almost forms
itself when you invite when you when you ask that that's one of the ways of finding the disconfirming uh experience there is actually a whole set of uh U techniques and strategies for finding the needed mism the needed discon and that's one of them simply asking whether the client has ever had an experience that went quite differently than what we have found so that's step two that's step two and that's what causes the neural encoding of the target emotional learning to rapidly unlock there's a a neurochemical neurophysical change in the synapses in the encoding uh
that the neuros scientists call the destabilization of that engram that neuro emble that encodes the target learning because the target learning now is destabilized in that way it can be directly unlearned and re-encoded according to the contradictory knowings that are now in View and so the third step simply consists of a few repetitions of the juter position of the the knowings that tell the client reality isn't according to the original schema so the therapist simply guides a few repetitions of the juxtaposition which is really natural and easy to do once the first jxap position experience
is there because this recognition is very very significant to the client this recognition of oh it's not the way it has seemed all along MH that's a big uh that's that's very surprising to the client yeah like I said it has this edgy quality and how do you direct attention between the two of them so do you tend to uh guide them more towards the exception or no yeah no again you if if if the therapist indicates any favoring of disconfirmation experience there there clients are very sensitive to any indication from a therapist that this
this side is invalid or incorrect or wrong to uh to to to to live by and this is the this is the correct favorite as soon as you give any indication of that what does the client do the client will begin to suppress and dissociate from the symptom requiring knowings because they are getting the disapproval of the therapist that would block the process we need the client fully allowing and and uh um experiencing yeah the bad stuff the troublemaking learnings so there's no favoring or tipping at all okay the therapist is in a very balanced
manner saying yes this has felt true all along and and you experienced this so strongly in your childhood and yet look you've also had these experiences that you're telling me are so different than this and in fact the the the my own usual way of guiding the J to position is to then include the question how is it to be feeling both of these very simple how is it to be feeling both of these that signals that I'm not favoring either one yeah and it maximally and optimally sets up the J depos experience yeah the
client is literally in front of both of these knowings they both feel real but they cannot possibly both be true that's the essence of the J deposition experience and then it's very natural to empathic review both sides of that again in the rest of the session gee how again I'm so curious how it is for you that you know XYZ has felt like the reality all along to you and here you're recognizing that you've had experiences where that isn't how the world behaved um yeah what's happening inside for you as you sit with both of
these so very natural very empathic very attuned you're you're accompanying the client in this J position experience and in in the accompaniment very natural to comment on both sides yeah two three four times more in the session each time the client returns attention to the both at once that's a repeat and that's the third uh experience in the sequence that uh carries out the the the counter learning that now is not operating as counteracting it's not just setting up a preferred separate new learning counter learning orchestrated this way lands directly on the neural encoding of
the target learning and reimposes it and can actually nullify the emotional learning that's been generating the symptoms we've we've seen this happen right before our eyes hundreds of times uh it's it's common for clients to to say this is a you know I I I'm right now I'm remembering a client who had formed the emotional learning at the age of 18 a woman I will never have I will never marry I will never have a family I'll never have children because she had become pregnant out of out of wedlock and had had an abortion and
she lived in a conservative small town where everybody knew about this MH so this was a catastrophe and the emotional learning that got set up was I will never have a a family or children she was now in her mid-50s was not conscious of that emotional learning Mar children and had sexual problems and depression both of which were maintained by the emotional learning I just mentioned at the point where we made this conscious I simply asked her to repeat it I had her back in being 18 years old telling me about this experience and what
it meant to her and that's when she said absorbed in the revisiting of the experience I'll never marry I'll never have a family I'll never have children I knew that she had married and had children and yet she's immersed in this state specific bubble of emotional reality that had formed at 18 so the I used a different method of finding the contradictory knowledge the disconfirming knowledge in this case it's the method I'm about to tell you is actually the one we usually use first you'll see why I heard her say it and I knew what
to do I said say that to me again just say that to me again and she said I'll never marry I'll never have a family I'll never had children her eyes popped open because she was closed eyes absorbed in the experience her eyes popped open and she shouted wait wait I did marry and have children right there is one of the most remarkable observations in my career of how the emotional learning and memory system works I would imagine that most kids are not so dramatic when no they're not so I don't usually use this example
to teach this because it's it's not really quite representative but it but it illustrates certain things very powerful sure and the reason I brought this one up is to tell you what happened next her head rain back on the top of her chair her eyes were darting around she kep saying this is huge this is huge this is amazing she said I'm feeling energy stream through my body she said I'm feeling the spaces between my toes this is huge and it was huge because that simple emotional learning is what was maintaining her her sexual problem
her sexual aversion because part of the learning was that having sex enjoying sex had ruined her whole life yeah mhh uh and and her depression immediately lifted and in a few more sessions was gone her Depression was largely the UN the the despair about her whole life based in that emotional learning it wasn't really depression it was despair yeah but unconscious despair looks and feels like depression so uh clients often have very strong reactions to the Jer position they express amazement they feel energy stream through their body um uh after the Jud the position after
the third step one thing we do to begin to test for those markers of eraser or nullification that we went over earlier is to is to say okay take a breath clear it all away feel the chair under you all right let's see what happens if you simply go back into how this was before this session and we try to recue the original emotional learning to see if it still triggers yes we invoke the same kinds of visualization the same powerful cues that have always reliably triggered that ego state that emotional bubble and how real
and troubling it feels if the J the positions have been effective now it just doesn't trigger and uh nothing of of that kind is evoked and usually the client spontaneously says something like H you know it feels silly to see things that way now like what was I thinking some clients actually burst out laughing in a in a particular kind of a Glee joyous free energy laughter you know it's like the nightmare is over like that's not me anymore it's not it that that this doesn't feel real anymore just brings this this release yeah of
of of joyous laughter and and tickled tickled amazement yeah Bruce would you mind if we talk a little bit about the importance here of repetition and time because this is such interesting work and maybe and from what I read this is I have some questions I'd like to address that I haven't got completely satisfying answer yet you could help me with that's yeah so the first of all the retrieving of the emotional schema part the discovery phase of your work how does it vary in terms of how hard it is and how much time it
is to actually get a client to reach this pH like where they actually say symbolize the emotional schema and how do you think it varies between clients and why do you think it varies it varies greatly it varies great L uh with some clients uh the whole emotional schema can emerge in just one or two sessions with other clients it can take many sessions one of the uh determinants of that is the degree of emotional intensity involved in the schem excuse me in the schema um if the if the emotional schema uh is extremely severe
if it if it involves traumatic memory then of course the work has to go in very small steps so that each step feels tolerable to the client at each point trauma therapists are very familiar with this many trauma therapists call it the window of Tolerance you don't want to access so much of the memory that hyperactivation occurs and the client has to dissociate or you know go into resist or avoidance um so we we you know the therapist has to have skills here of pursuing the discovery work at the pace the client can tolerate also
some schemas are more complex than others and have more layers and components that can take more sessions to fully to fully retrieve and so your clinical decision making is always on target you're always looking for this but maybe it can take like you're saying many sessions for steadily discovering this yes absolutely in in cases of complex attachment trauma uh some some therapists call that relational trauma developmental trauma um I use the phrase complex attachment trauma there you have numerous very emotionally intense schemas generating many symptoms and those schemas often are cross-coupled so the work becomes
very nonlinear and you're you're working on bringing into awareness several different schemas at once sometimes the progress with one schema is blocked until you do some more work with another schema and it's very complex work uh in the more intense cases of complex attachment trauma where you have oh 12 16 18 different schemas that all have to be put through this process for there to be a very thorough freeing of complex attachment trauma yeah that can take easily 60 80 100 sessions to do okay and even if every session is highly effective work of this
kind yeah even if everything is going as plan let's call it yeah and when it comes to the later phase of the just a position you were saying so you identify the schema you put a mismatch experience even then in more severe cases you would say that it can go on for many times like even if you're on target you have to do the disiz many times over many sessions ah actually that's a very important aspect of this thank you the familiar idea that creating change requires many repetitions over extended time repetitions of the of
the new preferred pattern MH that is the hebbian principle HEBs law right neurons that wire together fire together the fire together wire together yeah oh I got it backwards yeah thank you um uh that is actually the neurological view of counteractive change yeah incremental change that we discussed earlier doesn't matter got it wrong because it's wrong the principle anyway maybe that's why you got it wrong exactly but it comes to explaining I need to get it right yeah it's the the neurological point of view of counteractive change is HEBs law neurons that fire together wire
together right and that takes many repetitions to get them to fire together enough that they wire together strongly enough to be able to compete against the symptom generating learning and manage to override it enough to regulate it enough to get enough symptom reduction but as we were saying earlier this memory reconsolidation process of transformational change is a fundamentally different process and it's fundamentally different on the neurological level also it isn't using heads law um in fact there are several laboratory studies that uh focused on and showed that this this destabilizing of a Target emotional learning
and its nullification is a fundamentally different process than the HEBs law process uh and for example exposure therapies the process of Extinction yeah is the same process you build up a competing opposite emotional learning that hopefully overrides the target learning memory reconsolidation is a fundamentally fundamentally different process and it does not require numerous repetitions of the new pattern over extensive time does not does not the laboratory Studies have shown this you know 10 or 15 minutes of counter learning uh several repetitions sometimes it doesn't even take 10 or 15 minutes several repetitions of the disconfirming
experience after the target learning has been destabilized by the mismatch uhuh can completely erase the existing learning permanently so how do you bridge this this makes total sense to me but how do you bridge it with the need and now I'm not sure if I should use this word with sometimes doing this process several times with uh so does make sense yes well yes yes the the process works cleanly as I described it in many cases but it doesn't always yeah it doesn't there are complications that can take more sessions and more steps uh for
for introductory training in this whole framework we teach the basic steps keep it simple just get that map of process that's the core yeah and then yes there are additional steps required when complications arise which kind of complications various kinds of complications uh I mentioned one type earlier when I was talking about complex attachment trauma when the schema you're focusing on actually is coupled into other schemas yeah and isn't isn't free to dissolve yeah because other things will have to dissolve along with it yeah by dissolve I mean be unlearned be nullified right so there's
a more complex process that has to be worked uh that's one type of complication another type of complication is what what uh turns out to be a type of resistance to the Nullification of the schema resistance can occur client resistance can occur at any stage of the process the any of the steps mentioned [Music] um and review Resistance as coherent self- protection if the client is and of course by resistance we all mean the client is not allowing the process that the therapist is trying to guide right so when we guide A J to position
experience even when it's a very well-formed Dr depos experience uh the the the dissolution the Nullification of the target schema is not simply a mechanical result MH it turns out that if the client's implicit knowledge system anticipates some form of suffering or distress or hardship or cost that is anticipated to result from the schema being nullified the dissolution of the schema is not allowed so it's a very top-down uh I guess you know maybe you could say meaning driven process it's not just a mechanical process so when we when we believe we've guided a a
well-formed jop position experience that was also uh experiential it's you know that the client allowed the experiencing of both sides it looks like all that was in place and the schema remains in force in effect the content of the schema continues to feel real continues to trigger in the situations where it has triggered in the past that begins to be an indication to the therapist there's some way in which schema nullification is expected to bring suffering or some cost that is not workable yet from the client's unconscious this implicit point of view so that's also
like another emotional schema protecting the client from the process yes exactly exactly uh and so then we shift into that Interruption shift into we we launch the entire process a new focused on that and in effect we regard this resistance as the symptom I never use the word symptom with clients I'm sure um but now that symptom of not allowing the ju to position to be effective not allowing the schema to dissolve uh becomes the focus yeah and it begins with a simply a very natural question the way I tend to do it is to
say to the client you know I'm just wondering if uh you know I think I think we both understand at this point that where you want to get to is to where it would no longer feel real and true that doing something bad is the only way to get caring attention is that right is that where you want to get to the client will say yeah it is so then I'll respond okay let's take a look ahead let's see if we can just get a glimpse of how that will be for you to be there
not not how to get there but by imagination What will that bring for you just see if you can imagine for example um um being at work on a long hard day at work and you know you're working all day alone in your office and it feels kind of lonely and it's getting a little Bak with the trudge through all this stuff you've got to get done before you go home but now in this experience of this situation try on this knowing no there's caring attention available you could go talk to your boss you'll be
home with your wife soon you don't have to do anything bad to get care and attention that you need this is symptom deprivation it's it's actually a symptom deprivation that's one of our Discovery techniques but now it's being applied to the whole schema very cool yeah it's like a Meta syn Meta wow right you're having the client try out being without the schema whereas in the original or initial process of discovery work we might use symptom deprivation to to have the client try out being without the symptom yeah yeah that the unknown schema the Undiscovered
as yet schema is generating that helps us find the schema yeah that's very cool now we're doing symptom deprivation on the schema itself and and that what will that bring the client tries out experiencing I can get attention without having to do something bad what does that bring have the client check that out in this context in that context it will surface some way in which truly knowing that it's no it's not necessary to do something bad to to get carrying attention is going to bring some trouble something unwelcome something that does not feel workable
whatever it is say ah and then I'll say boy I wonder if that's why this you know this this learning yeah hasn't been free to just fall away even alongside so much that you now recognize you've experienced about how you can get carrying attention without doing something bad we've got to find how to make this workable for you because doesn't feel like that's a workable situation so you tried to nullify now this part well yes now we're together in recognizing how it's not workable to let the schema go uhuh and we're face Toof face with
a specific distress or dilemma yeah concerning that and we work on that and yes we do the whole process again and it will involve some transformation in the client's relationship to that contingency so you told us this sorry yeah yeah you gonna say just the last part of that at point where the anticipated difficulty now does feel workable to the client there's a comfort level now with how to be in that situation we return to the J the position do it again and now the schema does dissolve no it's possible yeah yeah yeah yeah so
so these are that's one of the main things that can be a complication and keep the schema in effect even after Jud the position experiences and require more sessions yeah so could you give us like a a span I know it's always hard to do this kind of questions but uh span between your least severe clients to or your most severe clients what would the typical I don't know for sure I've never actually seen I believe in your literature the term personality disorder or this kind of lingo but even so my more severe cases how
long would you stretch out coherence therapy yes yes um uh well starting with complex attachment trauma that's one of the more severe situations uh and as I said it can go up toward a 100 sessions uh to to carry out the process and unlearn and nullify numerous powerful intense often trauma Laden schemas okay uh and you bring up the situation of Personality Disorder as it's often called in the field yes that's another type of situation where it can take many many sessions and if the personality or character pattern is rigid enough severe enough it can
prove impossible to do yeah this has happened to you oh yes yes yes I've had cases where I I could not succeed in bringing about transformational change uh because uh well in in some types of character disorder the client is um and I you know I I I I don't tend to use the word disorder as you mentioned we don't use that phrase in our book because it's a pathologizing phrase as if something's broken or or malfunctioning in the client and you know we as I mentioned we have a coherence m Paradigm a coherence Viewpoint
and we view even these character patterns as coherent in other words they were formed to protect and they are adaptively necessary according to that person's experience of life so nothing's broken yeah but it's sometimes so rigid so hard so rigid that and some of those patterns involve a profound avoidance of inner experiencing uhhuh uhhuh uhhuh absolute avoidance of the kind of inner accessing of what's there that's necessary yeah usually for the memory reconsolidation process to happen there are U more procedural ways to carry out memory reconsolidation that don't entail accessing the core material explicitly okay
and that's a whole area that needs to be developed I just want to include that as a possibility here uh but it's not how we tend to work okay but it's a possibility so yes character rigid character problems is definitely an area where it can take many sessions or even prove to be uh uh unsuccessful and then one has to resort to counteractive methods that can help a person okay manage and and limit yeah symptom production just going to add that I think those may be the two major categories okay that require large numbers of
sessions yeah uh the the situation where very few sessions are needed are the ones where uh as you might predict the the symptom is maintained by one underlying schema and the client is comfortable with inner experiential accessing yeah and cooperative and there are no anticipated results of schema dissolution that are a big problem and then you can see a really a life-changing transformational shift happen in in one session yeah the ideal client that rarely happens in private practice oh it's not so rare it's seen when when you work this way uh that see a lot
rely yes and it happens within the work with you know with some clients a client's working on a certain problem it's relatively complex it's taking you know 12 20 sessions whatever but the client comes into a particular session and brings up a new problem uhuh not something I've heard about before so I begin the process on that that yeah that unwanted pattern of behavior or feeling or thought or sematic disturbance whatever the client has defined start the start the process and it often happens that we do the entire process in one session amazing yeah and
find the schema and find dissolution I can I if you want I can give you an example of that please do uh it just happened uh about two weeks ago okay a woman who' been working on different things started a session by saying uh listen I'm really upset I've got to work on this today and she describes a problem I have not heard about before she said uh yesterday I really fell apart um um my you know my husband has a fairly serious Medical condition and he's in chronic pain from it and for weeks and
weeks in fact for months I've been doing research online I've been finding out important stuff and I've been feeding information and suggestions to him and he hasn't been following what i' the information I've been giving him and not only is he not using the information he never even refers to it he never even mentions all the help I've been giving him and finally yesterday I lost it I fell apart I just sort of I don't know what it is I'm just in this dark dismal I'm just a mess I'm very very upset and that's she
couldn't def Define it any more than that initially yeah she was really immersed in a in in an altered state that was really dark and dismal she had kind of collapsed this was a kind of emotional collapse so okay that's that's the symptom I know what the symptom is um you know her husband not using her caring help is very distressing yeah in some way yeah so I began the discovery work what's underneath what's under this what are the emotional learnings that are driving this collapse so I simply said okay focus on how this feels
to you and with my caring you know or empathic accompaniment she was able to really hover with this really focus just focus on how it feels in your body picture your husband while you're focusing on how awful this feels and just by hovering with that more specificity began to show up she began to verbalize uh I feel so hurt I feel I feel so rejected oh oh I feel I feel unlovable okay so I know to her this feels like the truth of the matter but what I recognize is I'm hearing attributed meanings uhuh I'm
hearing specific emotional learnings if a significant other doesn't receive my caring help I'm unlovable this means I'm unlovable and I'm rejected and we we sat with that for a few more seconds and then what came was oh and I don't matter and with that she dissolved into deep crying sobbing deep deep tears that it that was the core I don't matter and that's that's a fairly common construct or attributed meaning to find and especially with clients who are presenting a low self-esteem there's often and I don't matter core of meaning that they learn from mistreatments
in childhood so now she was in touch with it I had this set of attributed meanings that's the target emotional learning yeah and now that I know what the the what the the target learning is now to carry out the core process the next step in preparation sequence as we call it uh is I have to find something that will disconfirm those meanings mismatches yeah mismatch so I was thinking about okay these are the meanings uh not all uh not all Targets not all emotional schemas are made of attributed meanings uh in fact the one
we worked on earlier was of a different type um many uh schemas are uh um like if then models of how the world is expected to behave if I seem fine I won't get any caring attention if I do something bad I'll get kep caring attention okay yeah that's a different type this woman had attributed meanings and so now I'm thinking what could disconfirm this sometimes finding uh a candidate disconfirmation experience can take several sessions sometimes that's a challenge M so now you would have to find if I understand logically some experience that would prove
that in other occasions she actually had meaning and she had meaning when whenever she she didn't have have to have the other loved person uh receive something yes you're getting close specifically and this shows how important it is to have thorough retrieval of the target learning because it is based on the detailed makeup of the target learning that you search for a disconfirmation yeah the disconfirmation that will be used for the mismatch experience must be very specific yeah and I'm so glad you pulled that out of it really that's a very important understanding of how
this process works and how the clinical methodology needs to work for consistent Effectiveness um so uh I have great specificity of the target learning these very specific meanings and now I have to find a very specific disconfirmation so I know that the disconfirmation has to be an experience in which those specific meanings are not true in other words her husband not receiving or using or even remembering all of her offers of help does not mean that she is unlovable and doesn't matter yeah that's a tall order how can I find that I locked out I
locked out but this way I locked out actually happens fairly common in my experience uh across many clients I I suddenly remembered because I know what I'm looking for I suddenly remembered something she had mentioned to me in a previous session and I thought it had a reasonable chance of creating a disconfirmation so I just went for it I just tried it didn't know if it would work or not and you'll see you'll see what it is when I explain what I said to her next I said listen didn't you once tell me about your
husband's childhood I think I remember you telling me that what he suffered uh as a boy was um he felt massively dominated and controlled by his mother I just said that and I looked out it worked she was silent she was very silent MH there was there was a there was a stone silence for a few seconds and then she said with a like a burst of energy right right oh that's why he's not taking my help okay he's afraid of being controlled and dominated by me like he was by her he's preventing that he
always does that you're right I didn't make the connection so you give her an alternative meaning precisely precisely but in a way I didn't give her that alternative meaning she already possessed that knowing and that's often what happens uh in fact the example I gave earlier of the woman who said wait wait I did get married married I did have children she already possessed that knowledge yeah yeah simple knowledge that by itself would seem to have no emotional significance yeah yeah but when it's pulled in for a j the position it has enormous emotional significance
and the same happened with this woman I merely brought her attention to a knowing she already possessed an inj position with the attributed meanings she was plunging into it made all the difference in the world you said it exactly correctly this was a different meaning for the same behavior of her husband so Bruce there is a an article that I would like to leave out the link also for people interested very interesting article that memory reconsolidation understood and misunderstood that you wrote and you you point out there are some Mis common misconceptions and you already
touched on some and you uh already fleshed out memory Rec consolidation is not Extinction for instance yeah but now I remembered from what you just said if you could also uh divide this or differentiate this from the idea of corrective emotional experience which you also do in that article because some people hearing us might think okay nothing new there you made a new corrective emotional experience yes how would you part of the reason I'm smiling like this is that uh in I I mentioned right at the start that I'm I'm hard at work on a
new article MH and I just happened to write the section that answers your question great it's a section that revisits the idea of corrective emotional experience through this lens okay so I have this fresh top of mind to share with you but I'll try and make it succinct um many therapists uh understand and try to carry out a corrective emotional experience by guiding the client into a a rich emotionally real experience of uh something that was missing in their developmental history typically um it's um I think we hear about corrective emotional experience most often in
the context of a reparative attachment therapy therapy where the therapist is deliberately using the client therapist relationship to create experiences of what was missing in the client's attachment learning history yeah so that you know the the empathy you receive from the therapist therapist safety positive regard the good alliance what what are often regarded as the non-specific common factors which are needed for any therapy to be effective I think can be used uh uh in a particular way to actually be the disconfirming experience of insecure attachment schemas that that keep the client experiencing um lack of
empathy yeah or or even abuse so sometimes they just oppose the the yes emotional schema yeah exactly the idea is to well view through the lens of memory reconsolidation we understand that A J to position is needed but in practice what many therapists do is a counteractive version of corrective emotional experience with all the best intent they're trying to get the client away from all those Troublesome learnings and focused on this very positive experience of empathy and nurturance and safety and positive regard in the client therapist relation ship the therapist I'm sorry the client can
certainly have a rich strong experience of all those positive qualities of relationship and can feel them can have uh feel nurtured without a juip position experience taking place the insecure attachment learnings can be suppressed or dissociated or were non-reactivated during the experience of the missing relationship qualities so there's relief there's Comfort but not a ju to position experience I think all therapists who try to use corrective emotional experiences know very well that sometimes they work and create a transformational shift and sometimes they don't we believe the memory reconsolidation framework reveals very clearly the critical specific
factors that determine whether a correct does or does not result in a lasting deep change so again the difference that makes a difference exactly yeah thank you yes so in effect what we recommend is a new definition of corrective emotional experience and I just put this into this new article uhuh great uh that it should be there we need an updated definition you know we started with Alexander in French's definition then a new definition was given uh in a book that came out I think it's a 2012 Book C Cast castane H I'm not sure
I'm saying his name yeah castan and yeah yes their book yeah uh they say some important things they're updating the understanding of corrective emotional experience and I think we're adding a new stage to that process by defining corrective emotional experience as that the J toos is needed in other words the problematic emotional learning yeah that you're hoping the corrective experience will dissolve needs to be activated and present and welcomed in the room alongside this so-called corrective experience you know we're not even fond of the word corrective because again it's a pathologizing connotation as if the
original learning is incorrect yeah no the original learning was a very correct model of what was really being suffered so we don't want to disrespect the client's original experience and the client's original learning by suggesting that it was incorrect incorrect uh um so we prefer different phrasing but um the so you found a step another step necessary step that should be included in order to make corrective emotional experiences more consistently and reliably effective at bringing about lasting change did did that answer question it totally did and it Bridges because you talked now about what could
be called a common nonsp specific common factors and as you know there's been this argument that you know the dodo bird verdict all win blah blah blah and you've actually been uh had quite an interesting reaction to this in a way because you've written that rather than regarding all therapies as having done equally well perhaps we should see them as having done equally badly so I did write that and I must ask you now to elaborate on this it's too good a sentence not to talk about it it's it's a it's a very intriguing area
okay yes uh well I you know it's well known uh it's certainly well known to uh therapy outcome researchers and it's fairly well known across the whole clinical field that outcome Studies have found a ceing essentially the same level of Effectiveness or let's say the same level of efficacy of therapy methodologies across oh how many 14 or so different therapy methodologies that have that have been found to have the same ceiling and you know usually that's written about to say by by saying that therapy has been proven to be effective that's a true statement uh
but when you but how how effective is is the question I ask and when you look at the numbers these statistics in the studies it's it's actually the same level of Effectiveness that placebos have that Placebo therapy has I'm not satisfied with that level of Effectiveness for the clinical field and I know that therapy sessions that produce transformational change produce a much higher level of Effectiveness than that and transformational change has not been the norm or the standard of Effectiveness in the clinical field we're working to make it be the norm and the standard of
Effectiveness and we think the memory reconsolidation knowledge can really help toward bringing that about so let's see back to your question um the the the most prevalent um understanding and explanation of why so many therapies have the same level of Effectiveness modest though it be is the idea that the nonspecific factors um factors of therapy in in therapy that are different than the specific techniques or methodology used by the therapist factors like the quality of the relationship the quality of the therapist's belief in the methodology the clients personal qualities that the client brings to therapy
non-specific common factors are what make therapy be as effective as is measured that's the non-specific common factors theory of therapy and of the the outcome research We Believe oh so it's important to include in that description uh the the the the aspect the piece of non-specific common factors theory that says specific factors can never be the dominant major cause or source of therapeutic Effectiveness specific factors the specific methodology or techniques used can account for at most about 15% of efficacy what we're pointing out is that the memory reconsolidation research the empirical rigorous findings which are
now extensive not Theory not the izing that the rigorous empirical findings have identified specific factors that predictably and verifiably produce transformational change profound change and that this is a major challenge to non-specific common factors Theory and it's possible to understand now why rcts randomized control trials have uh produced the modest level ceiling on therapy Effectiveness because randomized control trials don't identify they don't pull out of the many many therapy sessions studied by many therapists those few sessions that did accomplish a lot transformational change by happening to do the requisite experiences you know Alex I think
one thing we haven't mentioned in this interview that is very relevant right here and therefore it comes to mind for me is the fact that there is no other known process in the brain that can erase an emotional learning other than the memory reconsolidation process this destabilization of a specific learning by a mismatch experience there's there that's the only known neurological process the only known type of neuroplasticity that can destabilize an emotional learning and allow it to be nullified profoundly um so there is there is some empirical validity or support let's say for the hypothesis
that whenever we observe eraser robust disappearance of an emotional schema and its manifestations in therapy we we can infer that the that those three steps of the necessary sequence that brings that about have happened in therapy whether or not they were noticed by the therapist or conceptualized as such by the therapist so there are systems of therapy that do produce that sequence of of experiences and do produce transformational change but the therapy's conceptualization of the change process and the therapy's description of itself don't identify by yeah that or those experiences and yet they are embedded
AR is that if we actually looked at the session we would find this process in that yes and we've done that we've begun to carry out that demonstration our book blocking the emotional brain has a chapter dedicated entirely to that chapter six gives gives a a review of uh detailed case examples from four different widely used therapies EFT ADP EMDR yeah ipnb ipnb yes and we show uh where in the momentto moment process the three experiences took place resulting in the transformational change that was observed I'm sorry this is a little tongue and Chic but
isn't it a little bit uh funny or delicious in a way that you come from a very experiential constructivist background but what you're saying in a way is what nowadays would be defined as a medical model argument in the sense that if you contrast with the contextual model you're arguing for a specific specific process that argues for the outcomes we watch ah oh I see what you mean yes it it's a specific process but I don't equate that with a medical model right um that's a very interesting point I haven't thought about it that way
before so thank you well I'm basing myself on the idea of Bruce wampo definition or distinction between contextual and medical yeah yeah yeah no that's an important distinction and while I dis agree with Von about non-specific common factors Theory I disagree strong now about that I think U I think there's strong strong evidence strong challenge to show that specific factors can be the major uh source of therapeutic change um but about the medical model I I I I agree uh clinical symptoms and conditions uh uh are not uh uh appropriately uh uh understood in in
terms of a medical model uh be and and and I don't think uh using or showing that specific factors are effective equals a medical model because a medical model is a pathologizing model that views the symptom as being produced by something malfunctioning something pathological something broken yeah and we have the coherence model that I mentioned earlier that uh sense actually demonstrates in the course of therapy yeah that the symptom is produced by emotional learnings and the clients emotional learning and memory system the client's implicit Learning System is actually working properly in maintaining these original emotional
in forming them in the first place working properly in maintaining them without fading out for decades of a lifetime the neuroscientists have shown that implicit emotional learnings are not supposed to fade out the the the brain evolved in such a way as to maintain these emotional learnings durably across time without fading so the Persistence of these original emotional learnings is not dysfunction or mal function or pathology and the re-triggering of these emotional learnings in the present for for self- protection and well-being according to the original learnings is the proper functioning of the emotional learning and
memory system and the limic system so it's specific yeah I don't see any pathology or malfunctioning in any you know it's it's it's similar in a way to to what happens when you uh you know cut your finger and then for several days there's inflammation and redness and and pain and tenderness that all of those painful symptoms are the healing and immune system working properly that's not a malfunction yeah I see an analogy there yeah yeah so I think the absence of any pathologizing yeah and the uh the indepth uh uh identifying of the coherence
of symptom production makes our framework definitely nonm medal than a medical model yeah yeah Bruce we're drawing to a close now but let me still ask you how sad it is very sad yeah because I'm having a lot of fun so let me try to fit in still two more things little things two more okay yeah very very briefly first of all because again I I haven't really found out more about this what do you think is the potential of all that we've been talking about memory Rec consolidation knowledge to self-help do you think it's
possible eventually to actually a person understanding and trying to plan and go through their own memory consolidation process yeah we thought about that a lot because we've been trying to figure out how to write a book for the public I can imagine yeah you could you know you could easily write a book um um of the genre of Malcolm Gladwell Al outliers and uh some of his others very clever interesting books uh what's the What's the title of the book about quickly knowing something um uh Thinking Fast no no that's that's that's Malcolm Gladwell has
has one like that um one word title udes my memory yeah you know blink memory solid blink that's it thank yeah link I was the word think was coming yeah me too yeah um yes you could write a fascinating book that opens up this wonderful amazing world of how the emotional learning and memory system works but that's not self-help yeah it's more like trying to figure out self-help yeah and it's eluding us so far because as is Apparent from so much that we've discussed here in order to do the memory reconsolidation process u in a
fully effective manner you need to access the target emotional learning with some uh explicitness the details and that's very directly and very often these emotional learnings are full of intense distress and we often find in therapy that the client absolutely needs the empathic accompaniment of the therapist to tolerate accessing this material yeah um one of the ways that shows up very clearly is when we give a when the material such such material has been accessed during a session some piece of Discovery work has happened effectively the client is now in touch with a certain piece
of the schema will write the words of it on an index card give it to the client just read this once a day between sessions just to stay in touch with it yeah just to build it into routine daily awareness and often that goes perfectly well the client does it but sometimes the client comes back in the next session and says oh yeah the card gee I forgot all about it and it turns out it was resistance okay appropriate self-protective resistance because we look at how come what happened usually when I hear that response I'll
say gee I wonder if I wonder if you know I wonder if it felt workable to be in touch with that stuff while you were here with me in the session but I know I'll say this I know that sometimes being alone with the same stuff between sessions doesn't feel so workable yeah was it something like that and usually the client will say you know now that you mention it and now that I look back yeah yeah so the relationship does provide that space possible absolutely the relationship the non-specific common factors are are really necessary
uh in a catalytic sort of way yeah for the process to be Allowed by the client the specific process to be allowed by the client so um now purposes yeah ah thank you yes you so you can see that uh self-help is problematic uh it won't be very successful for many clients and they'll think it's a bad book book doesn't work you know then there's also the problem or the yeah the possibility that some people won't avoid or bounce out of the material they could access the material and be stabilized and and and be destabilized
by accessing it and get in some trouble yeah you know um there so there's ethical risks and safety risks involved in writing a self-help book on this stuff that we haven't solved yet okay if you can help us I'd appreciate it yeah I'll bring my Millennial mind to figure it out maybe you co-author of the book and sure I would love that our first million exactly try to go get to the Amazon top 10 yeah well maybe let's let's let's make our second million first because I've heard that the second million is always easier to
make then exactly well one last question that I've been asking all of our colleagues Bruce and I really want to finish off asking you okay is which advice or what advice would you wish to have received when you were starting out as a psychotherapist ah great question you know the true answer here's what just comes the answer is um um remember I mentioned the advice from uh Robert Shaw and um yes it's ation the advice from my mentor it was also one of Laurel's Laurel H's mentors M that's that's how she and I met by
the way we attended a workshop we were assisting at a workshop that Robert Shaw was very romantic it actually was but that's another story for another interview yes one over a glass of wine I think exactly um um next time I'm in Lisbon let's do that please let's see so yes from Robert Shaw but also from the constructivists that I mentioned earlier you know um the um the metal Research Institute constructivists and even the Milan uh and systemic constructivists um this idea that it's U and Robert Shaw was very emphatic about this it's possible to
get to the constructs that the client is living from and using to make sense of experience to get to the specific constructs that are involved in generating the symptom and to create rapid transformational shifts that was the advice that I got early early on that just sent us in this direction and led to everything we've done so I received the advice I most needed to get at the start of my career that's the answer that showed up as soon as you asked that question it's beautiful I like that i' never had that thought and it's
a it's a good feeling so yeah that seems very fulfilling I guess it is it is life life treated us well so brua I think that's a perfect way to finish our talk let we just say how happy I was to have this chat with you thank you it's totally Mutual this has been a real pleasure thank you
Related Videos

55:38
Memory Reconsolidation -- an interview wit...
Experiential Psychotherapy Training
1,333 views

52:04
Diana Fosha on Accelerated Experiential Dy...
Psychotherapy Expert Talks
39,089 views

33:07
Can you heal from trauma without therapy? ...
MedCircle
92,634 views
1:37:03
The Physics of Transformational Change: Br...
The Plant Yourself Podcast
714 views
20:14
MEMORY RECONSOLIDATION: Key To Transformat...
CPI Admin
50,639 views

38:30
Courtney Armstrong and memory reconsolidation
The Science of Psychotherapy
2,210 views

16:06
The Greatest Mathematician Who Ever Lived
Newsthink
479,652 views
22:40
Memory Reconsolidation: A Unified Framewor...
Dr. Tori Olds
8,658 views

58:04
Jon Frederickson on Deliberate Practice an...
Psychotherapy Expert Talks
18,945 views
44:40
Donald Meichenbaum on the Evolution of CBT...
Psychotherapy Expert Talks
8,988 views

48:05
George Stricker on a lifetime of Psychothe...
Psychotherapy Expert Talks
3,039 views
1:25:28
The Brain's Process of Profound Change: A ...
CPI Admin
8,096 views

59:15
Jeffrey E. Young: From Cognitive Therapy t...
Psychotherapy Expert Talks
103,981 views
26:13
Bruce Ecker Interview | Coherence Therapy ...
Dr. Tori Olds
10,114 views
18:57
How to 10x Your Emotional Intelligence - D...
The Weekend University
23,068 views

1:04:15
Giancarlo Dimaggio on Metacognitive Interp...
Psychotherapy Expert Talks
9,035 views

1:01:31
Virtual Lunch Together with Bruce Ecker
Leading Edge Seminars
1,165 views

1:23:55
Memory reconsolidation: A potent process o...
CPI Admin
4,078 views

8:27
Coherence Therapy Demonstration Session lo...
Experiential Psychotherapy Training
4,412 views

10:50
The night we met: Bruce Ecker's memory rec...
CPI Admin
2,237 views