The cutting edge of anti-ageing science | Venki Ramakrishnan
22.75k views19767 WordsCopy TextShare

80,000 Hours
Molecular biologist and Nobel Prize winner Venki Ramakrishnan discusses his new book, _Why We Die: T...
Video Transcript:
Venki Ramakrishnan: The number of centenarians has been going up with time. But the number of supercentenarians — people who live over 110 — is not going up at the same rate, and you would expect it to also be going up. That suggests that we’re reaching some sort of hard limit. Supercentenarians are known for the fact that they’re extremely healthy and relatively independent most of their lives; they don’t suffer from many of the diseases of old age that most of us get. And then they have a rapid decline and die after they’ve reached 110. That also
suggests that there’s a sort of general breakdown of systems and things are collapsing. Now, this doesn’t mean that there’s a physical or chemical law that says we can’t live beyond 110 — because there are species, even vertebrates like whales and sharks, that live several hundred years. What it means, though, is that in order to live beyond that, we’re going to have to do something about the process of ageing itself. Luisa Rodriguez: Hi listeners. This is Luisa Rodriguez, one of the hosts of The 80,000 Hours Podcast. In today’s episode, I was fortunate to speak with Venki
Ramakrishnan — a Nobel Prize–winning molecular biologist — who walked me through the cutting edge of anti-ageing research. I found this incredibly valuable and interesting given that the longevity field seems to be simultaneously full of genuinely mind-blowing scientific research, and then also pretty full of baseless claims and false promises. Venki is great at breaking down complex topics in a way that a non-biologist can understand, so I also came away with a way better understanding of the mechanics of ageing and death. Plus, toward the end, we have a fascinating talk about the social impacts of increasing human
lifespan — like what it would mean for our already-ageing population, and why Venki thinks differential access to anti-ageing interventions could actually make both economic and health inequality loads worse. All right, without further ado, I bring you Venki Ramakrishnan. Today I’m speaking with Venki Ramakrishnan — molecular biologist, Nobel Prize winner, and author of Why We Die: The New Science of Aging and the Quest for Immortality. Thanks for coming on the podcast, Venki. Venki Ramakrishnan: Thank you. It’s a pleasure. Luisa Rodriguez: So I hope to talk about which ageing and longevity research is actually promising and which
is overhyped. But first, why did you write Why We Die? Venki Ramakrishnan: I think for several reasons. First is it’s a big existential question. We may be the only species that’s aware of mortality. Other species are aware of death — they’ll mourn one of their own when it has died — but we’re the only species that probably realises that we have an expiration date, that we are unlikely to live past a certain age. That awareness of mortality has really driven a lot of human culture; a lot of human culture is about denying death, and thinking
of it as a passage to something else. And for most of our existence as a species, there’s really not much we could do about it — that’s why people say “as certain as death and taxes.” But in the last few decades, molecular biology has made tremendous advances, and we’re beginning to understand the real underlying causes of ageing, which leads to death. Now, coupled with that, what’s happening is that societies are getting older. People are living longer, fertility rates are dropping — and this means that the population as a whole is getting older, there’s a bigger
fraction at the older age of the spectrum. And that means that we really need to ensure that, as people age, they continue to be healthy, preferably independent, and preferably productive. That’s leading to a lot of investment in anti-ageing research to understand what happens with age and how to combat those effects. Along with support from governments and various funding agencies, there’s also been a huge explosion of the anti-ageing industry — about 700 longevity companies in just the last 20 years alone, and tens of billions of dollars gone into the industry — and that itself has also
generated a huge amount of hype. So I am a molecular biologist, and I work in the area of how proteins are made and how protein synthesis is regulated and controlled. It turns out that those processes are very central to ageing: during ageing, our control of protein synthesis starts going awry. So I’m close to the field, but I don’t actually work in the field of ageing per se. I thought somebody who’s very close to the field, but not in it, and I don’t have any vested interests, this is a good time to take an objective look
at the field and try to separate the hype from the reality. This combination of reasons is why I wrote the book. Luisa Rodriguez: That makes a lot of sense to me. And also it did feel like an incredibly valuable contribution to what does seem like a field with potentially a tonne of promise, but also what sometimes feels like a lot of people getting ahead of themselves in terms of making claims and promises about particular anti-ageing interventions. Venki Ramakrishnan: Yeah. I think there’s a whole spectrum. One end is very rigorous and sensible; and then there are
in-between things that are based on promise, but they’re slightly jumping ahead of the game; and then at the far end there’s things which have no evidence at all being promoted. Luisa Rodriguez: Yeah. So your book is really just, from start to finish, taking a look at all of the things that the anti-ageing research community has proposed, and said, “This one, in fact, seems based on really good science. This one seems like this middle case. This one is basically debunked.” So we’re going to talk about a bunch of those. But before we do, I wanted to
talk about this fundamental question of why we die — starting with a question that I think might seem a bit tangentially related, but that helped me realise that I had some assumptions baked into my views on death and ageing that maybe we should question first. So, for the most part, the immortal jellyfish and an aquatic animal called the hydra don’t age biologically. They mostly die of predation and starvation. How is that possible? Venki Ramakrishnan: I should say when people say they don’t age biologically, they mean a particular thing: that their mortality rate doesn’t go up
with age. In all of us, that mortality rate rises exponentially with age. For example, a 10-year-old is very unlikely to die of old age between 10 and 11. But if you’re close to 100 years old, your chances of surviving a year are only about 50%. You can see that probability of dying goes up exponentially with age. And with these animals, they found that the probability of their dying of what we would think of as “natural causes” doesn’t seem to go up. But that’s not to say it doesn’t go up. There were other species, like the
giant tortoise or the naked mole-rat, which were also thought to be biologically immortal — but if they live long enough, you can see all of the signs of ageing that we see in you and me and other animals. So it could just be that you just have to wait long enough. Now, the reason that these species seem to keep going is because they have cells called stem cells, which are involved in regenerating tissues, and their stem cells are more distributed, so they can regenerate themselves almost constantly in a way that we can’t. So that’s one
reason why they don’t die. I like to think that they’re more like plants in that respect, because plants also have this ability to regenerate their stem cells that are distributed throughout. That’s why if you take a cutting from a tree, you can plant another tree and it’ll just grow. So they’re a slightly weird case, and it’s not clear how much they apply to us. Luisa Rodriguez: Yeah. It made me wonder if, for all of their differences, are there clear reasons why you wouldn’t get an animal evolving not to die? Including more complex ones like humans?
Venki Ramakrishnan: I think the main reason would be that there’s no selective pressure on evolution to extend our longevity. Rather, what evolution really optimises for is for “fitness” — which is the biologist’s term for the likelihood that you’ll successfully pass on your genes. So evolution is selecting for reproductive ability. Now, in the course of an organism, there’s always a tradeoff: how much do you invest in growth and reproduction versus maintenance and repair which will make you live longer? And the equation is different for different species. If you take a small animal like a mouse, it
hasn’t been selected for longevity: a mouse only lives for two years. And the reason is that it’s not an advantage to select for lots of genes that are involved in maintenance and repair, because a mouse is going to be eaten by a predator long before it gets old. So there, the selection has been for rapid growth and maturation and reproduction — so that before it dies of other causes, like being eaten or starving or in a flood or something, it actually has a chance to mature and reproduce. If you look at larger animals, they tend
to live longer, because they are more resistant to predation. And there, it’s an advantage to have them live longer because they have a longer lifetime over which to reproduce. So there’s a rough relationship between size and longevity and lifespan in these animals. And I’ll give you another curious example, which is a bat called Brandt’s bat. Now, this bat can live for 40 years, but it weighs about the same as a mouse. How come a mouse lives only two years? Well, it’s because the bats can fly, so they can escape predation. They can also forage over
a much wider area, so they’re not likely to starve like a mouse is. So for all these reasons, it’s worth it for evolution to select for longevity in a bat where it wouldn’t be in a mouse. So death is not programmed; it simply happens because we accumulate damage. But in some species, it’s not worth investing in repairing all that damage. In other species, it is. Luisa Rodriguez: That makes tonnes of sense. Yeah, your book really did help me understand much better that accumulation of damage, and exactly what is happening mechanically when we age and eventually
die. Just to help our listeners get a sense, can you explain what ageing is concretely, and how it causes us to die? Venki Ramakrishnan: I would say, broadly speaking, you can think of ageing as an accumulation of damage with time. This is a damage to our molecules, which in turn affects our cells and our organelles, and then that in turn affects our tissues. So this damage gradually builds up over time, and it reaches the point where you get loss of function. And some loss of function is tolerated and we’re still alive. I mean, I have
osteoarthritis in my shoulder, when I still like to think I’m very much alive. But other functions are very critical. So if the loss of function is critical — for example, if your heart stops beating or your brain stops working — then you can no longer function as an individual. And that’s when you die. The body can no longer function as a whole unit, a coherent unit. And there’s a paradox here, which is: while we’re alive, millions of cells in us are dying all the time. In fact, some of these cells have to die to keep
us alive. And at the other end, when we die, most of our cells are still alive. In fact, entire organs are alive: that’s why if you signed your driver’s licence appropriately, you could donate your organs when you die to some recipient. So death really means the inability to function coherently as an individual. And that’s due to the loss of some critical function, which, again, is due to buildup of defects from ageing. Luisa Rodriguez: And all of those effects due to ageing, do they boil down into the different diseases that we know about and categorise, like
heart disease and cancer, as opposed to other processes? Venki Ramakrishnan: No, I think you can think of ageing as an underlying process. Well, it’s not just one process, but underlying defects that are building up in many very critical biological processes. And that, in turn, increases the risk of these various diseases. That’s why you can think of these diseases as not exactly manifestations of ageing — because you can get heart disease when you’re young, or cancer when you’re young — but the risk of getting those diseases goes up with age. So you could think of them,
in some sense, as caused by defects that build up with age. Luisa Rodriguez: I guess another way of thinking about this question that helped me understand this better, and that you talk about in your book, is asking to what extent would average lifespan increase if we eliminated the diseases that are often responsible for death in later years in humans? Venki Ramakrishnan: Yeah, that’s a very interesting question. People have estimated that if you eliminated the major causes of death, for example, today — and I’m not talking of accidents or infections, I’m talking of diseases of old
age — things like heart disease, stroke, heart failure (which is all, I guess, part of cardiovascular disease), or you can have diabetes, or you can have cancer. If you eliminated all of them, people estimate that you might only live another 15 years, you might gain another 15 years. And that’s somewhat surprising, but that seems to be what demographers agree on. Luisa Rodriguez: How do you make sense of that? This fact that ageing seems to really contribute to the risk that you’ll get one of these diseases that will cause your death, and yet that only seems
like a small part of the picture? Venki Ramakrishnan: Yeah, I can see what you mean. Well you can think of ageing as an underlying process that increases the risk of all these diseases, because it creates defects, and those defects often will manifest themselves in these diseases. It doesn’t mean you need age to have those defects — you can have those defects when you’re young — but the probability of acquiring those defects goes up with age because things start getting damaged and breaking down. Luisa Rodriguez: Do we have any reasons to think that there are natural
limits to the maximum human lifespan? Venki Ramakrishnan: I think in theory we might not. But the oldest person to have lived was a French woman named Jeanne Calment, who lived to be 122. She was a very colourful character, and one of the interesting things about her is that she smoked a cigarette and had a glass of port well into her hundreds, apparently. I think she also rode a bicycle. So she was a very colourful character. She consumed about two and a half pounds or about a kilo of chocolate a week. That I could probably get
behind. I wouldn’t recommend the cigarettes and the port, though. Anyway, she died in 1997. Since then, and it’s been about 30 years since she died, no one has lived to be over 120. Most people die around 115 or so. I don’t mean most people, but most of these very, very old people, these super outliers. That suggests that maybe somewhere between 110 and 120 is a sort of natural limit, and even if everything goes well — you’ve won the luck of the draw in terms of your genetics, and by sheer luck you’ve escaped all those other
diseases like cancer and heart disease and so on — you still end up dying around that age. And that suggests that there are underlying processes in the body, and we’ve evolved in such a way that they break down at about that age. So even in the best of cases, we don’t live beyond that. Now, another interesting fact is the number of centenarians has been going up with time, mainly because more and more people are surviving into their 80s due to improvements in healthcare and lifestyle and so on. And more of them, therefore, are surviving to
100. But Tom Perls, who directs the New England Centenarian Study in Boston, told me that the number of supercentenarians — people who live over 110 — is not going up at the same rate, and you would expect it to also be going up. That suggests that we’re reaching some sort of hard limit. Now, this doesn’t mean that there’s a physical or chemical law that says we can’t live beyond 110 — because there are species, even vertebrates like whales and sharks, that live several hundred years. What it means, though, is that in order to live beyond
that, we’re going to have to do something about the process of ageing itself. Luisa Rodriguez: Right. Do supercentenarians, when they do eventually die, die of the same diseases as people dying at younger ages? Venki Ramakrishnan: I don’t know. But the one thing I do know is that they go into a rapid decline. Supercentenarians are known for the fact that they’re extremely healthy and relatively independent most of their lives; they don’t suffer from many of the diseases of old age that most of us get. And then they have a rapid decline and die after they’ve reached
110 at some point. Luisa Rodriguez: That’s fascinating. Venki Ramakrishnan: That also suggests that there’s a sort of general breakdown of systems and things are collapsing. Luisa Rodriguez: Exactly. Yeah, that’s what feels really fascinating about it. OK, moving on a little bit: one idea that comes up in the book is that genes or physical structures in the body that contribute to ageing and diseases that cause death later in life are sometimes brought about by genes or processes that are actually beneficial early in life. Can you give an example of that? Venki Ramakrishnan: So this idea is
part of the general evolutionary theory we discussed, which is that evolution optimises for fitness. So if there are genes that give you an advantage early in life so you can mature and produce offspring, those will be selected for even if they cause you to age or cause problems later in life. And there are a couple of examples. One is that many of the pathways that allow us to grow and reproduce — for example, the insulin growth hormone pathway, or the TOR pathway — these are pathways that allow us to grow quickly early on, allow us
to mature so that we are not vulnerable, we reach adulthood, we can reproduce. Those pathways themselves are the causes of ageing later in life, and inhibiting those pathways later in life actually extends our life in some ways. Another interesting example is that most of our cells cannot divide indefinitely: they can only undergo a certain number of divisions, and then they stop dividing. This is because with each division, our chromosomes get a little shorter, and when they reach a particular point, they’re recognised as aberrant chromosomes, and the cell is then sent into a state called “senescence.”
And we can talk about senescence later because it has a lot to do with ageing. Now, why would you evolve that? Well, the reason is you wouldn’t want all your cells to have an indefinite capacity to reproduce — because if they acquired mutations and kept on reproducing, they could be a risk for cancer. So this whole idea may have really started off as an anticancer mechanism. So you don’t want to die of cancer early in life, but the result is that you accumulate senescent cells later in life and it causes ageing. Luisa Rodriguez: Is that
a thing that you see frequently? Is that a very common kind of tradeoff that happens in lots of systems? Venki Ramakrishnan: That tradeoff, I think, exists throughout biological processes. I’ve given you a couple of examples, but there are probably many more. Luisa Rodriguez: Yeah, that’s really interesting. How does the ageing clock reset each generation? I guess, in other words, why doesn’t a woman who bears a child at age 30 have a child with more defective mitochondria and misfolded proteins and more problematic DNA mutations than a woman who has a child at age 20? Venki Ramakrishnan:
There are reasons for this. The ageing clock seems to be reset in each generation because, as you point out, a woman who’s 40 years old and gives birth to a child doesn’t give birth to a child that’s 20 years older than a woman who’s 20 years old giving birth to a child: both of the babies start effectively at age zero, or nine months or whatever the gestation period is. So I think it is a fact that the ageing clock appears to be reset. Now, it’s done in a lot of ways. One is that our germline
cells — like our egg cells and sperm cells and their progenitors — are very highly protected, and they have special mechanisms so DNA damage in those cells is less, because DNA repair mechanisms are better in germline cells. I mean, a woman is born with the eggs, they age along with the woman, but they age less than the rest of the woman. And sperm cells, the precursors of sperm cells also suffer less damage. Now, along with that, there are actually many more eggs initially, or the pre-germline cells in a woman, than the actual number of eggs
that are released throughout her lifetime. Why is that? It’s because most of those cells don’t actually make it all the way into a mature egg that’s secreted during every menstrual cycle. There’s a huge amount of selection to eliminate cells that are sensed as defective. So there’s a lot of selection process in the process of ovulation. And the same with sperm cells. Sperm cells are made in the hundreds of thousands and then they have to swim. And any sperm cell that’s not healthy won’t actually make it to fertilisation. So there’s a lot of selection at that
stage. It’s not perfect, of course — that’s why you have defective embryos and defective babies as well — but there’s a strong selection process, and even when the embryo develops, it can eliminate abnormal cells. So that’s the first two parts: prevention of ageing by better repair mechanisms, and a strong selection process to eliminate defects. Now, there’s a third thing, which is that all of the genetic marks that we acquire with age, these epigenetic marks on our DNA, are erased, and new marks are put on so that the genetic program is reset and the embryo starts
from scratch, the fertilised egg starts from scratch. So the marks of ageing on the DNA are erased. All three of them contribute to resetting the clock. Now, there is one interesting thing that I observed in the course of writing this book. You remember Dolly the sheep was the first cloned mammal. It wasn’t the first cloned animal. That was from a frog, for which John Gurdon received the Nobel Prize. But Dolly was cloned from an adult cell of a parent sheep. And the genes from this cell, the nucleus from this cell was implanted in an egg
of another sheep and persuaded to grow, and resulted in a clone of the parent animal. Dolly was very sick, and died at about half the age of a normal sheep. So people said, “This is because you took an adult cell which had already aged and was damaged.” So they said this shows you can’t reset the clock because of various problems. But it turns out that around the time Dolly was cloned, there were other sheep that were cloned, and many of them went on to live normal lives. So it is possible — in principle, at least.
I don’t know how many generations you could do this, because eventually the defects may well catch up, but at least in one generation you can actually reset it. But it’s not efficient, because most of these cloning experiments result in aborted foetuses or defective embryos. Again, there’s a lot of selection going on, and you are selecting for those embryos that actually made it all the way to a full-grown animal, and some of those do have normal lifespan and turn out to be normally healthy. So this suggests that, at least partially, you might be able to reset
the ageing clock. Luisa Rodriguez: Right. And just to check I understand: it’s not that they did anything to the clones that were healthier to try to reverse the ageing process of the cell? It’s just that, in some cases, the cells that the clones came from were less damaged overall and so yielded healthier adults? Venki Ramakrishnan: It’s not completely clear. It could be that the procedure itself is not very great, and cells don’t necessarily reach the optimal state from which to start over again. It could be the way they implanted them. What they do is they
take egg cells and remove the nucleus and put this nucleus that has been prepared from the adult cell in order to clone, and then that has to be implanted in an animal to grow. So things could have gone wrong. And it’s not my field, and so I don’t know the details. Luisa Rodriguez: Right. I’ve just got flashes of a dystopian world where we don’t figure out any of these other areas of research, but we do figure out how to clone ourselves and then harvest our organs, because that is a regeneration. Venki Ramakrishnan: It is a
scary thought. When Dolly was cloned, there was this idea that maybe billionaires might want to clone themselves, or they might want to clone a child that they had lost in an accident. And here’s another big area: people often want to clone their pets, because they want the same — Luisa Rodriguez: I have to admit, I relate to this. Though I think if I thought about it more, I’d decide against. But I get the impulse. Venki Ramakrishnan: Exactly, because it’s not the same animal! It’s a different animal, even though it’s a clone genetically, but it’s not
the same animal that has gone through the same experiences and so on. But as I said, people’s psychology is very interesting. Luisa Rodriguez: Let’s go ahead and get into some of the very specific ways in which different systems in the body age and eventually stop working, and the therapies that could slow or even counteract those processes. One such therapy is parabiosis, where the blood of a young animal or person is fed into the circulatory system of an older person. What’s the best argument for this approach? Venki Ramakrishnan: Well, there’s no question that when they connected
an older animal, like an older rat, to a young rat, the blood of the young animal benefited the older animal. But it’s also true that the blood of the older animal had a detrimental effect on the young animal. There was at least one study which said that the detrimental effect of the old blood was actually greater than the beneficial effect of the young blood. Which means that as we’re ageing, we are accumulating factors that are not good for us, that maybe were useful early in life — this goes back to evolutionary theories — but maybe
later in life, they’re not so beneficial to us. They’re hanging around because we evolved that way. So that has led to the idea that you could look for factors in blood that have beneficial effects. In that case, you could find out how they worked and maybe try to mimic the same effect. Or you could also find out what the bad actors were, the things that caused problems in old blood, and figure out ways to eliminate them. So both are possible, and there’s a lot of work being done in the area. As with all these ageing
findings, it’s not prevented people from jumping the gun. There are companies that sprung up that took blood from young donors and sold them to rich old men who wanted to live longer. You get these sort of bizarre things happening. And it just tells me that, of course, none of us wants to get old and die, but there are people there who are very rich, and they’ll do anything they can to stay young if possible, and preferably not age and certainly not die. And they’re not necessarily ready to wait for the evidence because they feel that
by the time the evidence comes along, they might be too old and they might die, or might already be dead. So I can understand their psychology, but it’s not a very healthy situation for the field. It would be like if in the COVID pandemic, imagine if people just had some early indications of the vaccines and didn’t do any clinical trials and just said, “Yeah, it looks like it’s working. Give it to a billion people.” It would be exactly like that, and you could have had serious side effects and problems. As it is, we know a
very, very small fraction of the population did have side effects, which is true of any vaccine. But clearly you had to do that cost-benefit ratio; you have to establish that properly so people can make an informed decision on whether to approve it or not approve it, and also people can make an informed decision of whether to take it or not. So that risk-benefit ratio needs to be established. Luisa Rodriguez: Yeah, I’m very sympathetic to that. Out of just curiosity, given that they’ve already done it: for the individuals who have received blood from younger people, is
there any reason to think that it’s helped them? Venki Ramakrishnan: I think there’s absolutely no evidence yet that it has helped them in any way. The best case is Bryan Johnson, a tech billionaire, who spends $2 million a year on various anti-ageing measures — including trying all these things, and also measuring lots of data on himself. He’s a data freak, and he thinks of himself as doing a service to the research community by being a guinea pig for all these potential avenues. There was a period when he actually received blood transfusions from his son, and
I think also gave blood transfusions to his dad in a three-way exchange or intergenerational exchange. But what I read was that he didn’t notice any improvements in the markers that he was measuring, and eventually dropped the transfusions. Although I believe he said that in principle, the principle is still true — which I agree with. The principle is true in the sense that there are these experiments. But again, you have to wonder how efficacious they are. Maybe young blood doesn’t really help you much. Maybe it’s the removal of the old blood that actually helped. So I
think people need much more research to clarify what is going on. Luisa Rodriguez: Right, right. OK, moving on: do you have a take on how promising cryonics is? Venki Ramakrishnan: Oh, I think that’s a fairly out-there idea. So there is a legitimate area of biology called cryopreservation, or cryogenics, and this is how can you preserve tissues over the long term? And if you just took a salad and just froze it, you would very often kill it — because water, when it forms ice, will expand, and by expanding inside cells, it essentially breaks open the cells
and destroys the tissue. This is why if you take fresh strawberries, which look fantastic, and then put them in your freezer and then thaw them out, they don’t have anywhere near the texture that they had when they were fresh, because they turned sort of mushy because you’ve frozen them and thawed them. People have worked out procedures to freeze cells. For example, biologists routinely freeze all kinds of cells, including human cells, and then know how to thaw them and they’re still alive and can function. You can even do that with certain tissues. You can do that
with embryos. People freeze embryos. Women will often freeze their eggs. They’ll freeze their eggs if they’re going through chemotherapy, so that they can still, after they’ve finished having chemotherapy, have children. So there are all sorts of legitimate uses of cryogenics. Now, people are trying to figure out how to freeze larger and larger entities, biological entities like tissues or organs. It’d be great if you could freeze organs and store them for future use — but the reality is that people haven’t frozen even a small animal, like a mouse, and resuscitated it into a live mouse. And
I think that’s a real problem. So how do you do that to an entire human being? It hasn’t stopped companies from offering services where they’ll take your body and freeze it — or in some cases, they will freeze only your head, because there’s this extreme idea that, well, our consciousness is all in our brain; we don’t really care about the body. We just want to be existing as a conscious person. How would they even live without a body, even if you somehow thawed that brain? People say, “I’ll dump that brain into a computer, and then
I’ll exist as a computer entity.” Well, what if you dumped it into two computers, then are there two of you? Which one is the real you? It creates all sorts of silly logical contradictions. The reality is our existence and consciousness is very intimately tied to the rest of the body as well as the brain. The brain interacts with our body: it interacts through hormones and various other signals. It doesn’t exist in isolation. Now, these companies don’t actually promise that you’re going to be able to successfully resuscitate the body. They simply say, “We will freeze your
body using this protocol, and it’ll cost you x amount of dollars. And in return, we’ll keep it frozen for x number of years.” Luisa Rodriguez: Right. “And we’ll cross our fingers that someday we’ll find a way to resuscitate it.” Venki Ramakrishnan: So these people who are into this are betting that eventually some technology will come along to thaw this and somehow fix it all. Luisa Rodriguez: Sure. Well, I’m interested in the gap between successful cryogenics and this full-body or even brain cryonics that you think is, at least right now, very unrealistic. How does cryogenics work
in, say, embryos? How have we gotten embryos to freeze without bursting or similar? Venki Ramakrishnan: They use certain cryoprotectants — think of antifreeze or things like that, which prevent ice formation — and then you can very rapidly freeze them so that you don’t get ice formation. That’s one of the keys to doing it. And the larger the organ — and also if you’re surrounded by other things, like a skull and bones and skin and so on — it’s just much harder to do that sort of thing. Luisa Rodriguez: Right. So it’s much easier to do
for smaller and uniform systems because you can more easily kind of get the antifreeze across it. Venki Ramakrishnan: Yeah, because you can bathe it in your compound and without killing the cell. Luisa Rodriguez: Whereas when you get to a full body, you can’t. Venki Ramakrishnan: Even a mouse. You can’t even do a mouse. So I will start believing in cryonics when they can freeze a mouse and thaw it and have it running around. At that point, I will say they’re making progress. Luisa Rodriguez: “OK, I buy it.” Do you have a sense of what’s being
done to close that gap? Venki Ramakrishnan: I don’t think it’s possible. There are people who, in the case of a mouse, one thing they have done is they’ve been able to freeze the connections: they’ve been able to preserve the connections between the neurons in a mouse. But the way they do that is by injecting antifreeze in the mouse while its heart is beating and it’s still alive, and this antifreeze then goes into the brain and kills it. So effectively, the procedure kills the mouse, and then they can freeze it. But even that simply preserves a
connection; it’s not preserving the state of the neurons. So there’s no guarantee. The idea that you could thaw this brain and it would work like a mouse brain, there’s absolutely no evidence for that. All you can say is if you want to look at the connections in the brain, you could do that with this procedure. It doesn’t mean that the state of the brain — which in some ways reflects its state at the moment of death — would exist. And the other thing is that people would do this when they’re old. You’d be pickling your
old brain. This is not some youthful brain like when you’re 20 or 25. Luisa Rodriguez: OK, so this is maybe on the extreme end for you of not very plausible. I think, in general, a lot of leading gerontologists think that the more ambitious goals of the ageing research community are basically unachievable or science fiction-y. Is it possible that at least some of that is short-sightedness? I have this feeling that many fields seem weird early on, before the paradigm has really shifted. Venki Ramakrishnan: This is the argument that the extreme advocates of life extension say. So
there’s this fellow, Aubrey de Grey, and he says that if we can solve these seven things, then we can solve the problem of dying. One of his claims is that the person to live to be 1,000 years old has already been born. He says it will happen in stages. So what will happen is you’ll make advances that will allow you to live 200 years, and then by the time that person reaches close to 200 years, science will have moved on. So he could now live 400 years, and therefore it just keeps on going. He calls
this “longevity escape velocity” or something like that. Now, gerontologists have looked at every one of his seven things, and not one of them is actually even close to being achievable. And his answer to that was that the former president of the Royal Society, Lord Rayleigh, said that heavier-than-air machines are impossible — and so these people are just like that. That’s sort of what you’re talking about, which is that things that might have seemed completely far out actually came to pass. But there were many other proposals around that time. For example, Jules Verne wrote lots of
science fiction. One of the things he wrote was From the Earth to the Moon. And that actually has happened — not in the way he predicted, but it has happened. But he also wrote a book called Journey to the Center of the Earth. That hasn’t happened, and will never happen, given what we know about the centre of the Earth. So I think for every far-out idea that turns out to be true, there were probably hundreds that were simply crackpot ideas. In general, occasionally science will have these revolutionary advances. But by and large, it advances building
on the knowledge we have, and seeing what the next questions are, and then getting to the next stage and the next stage and so on. That’s the vast majority of science. And occasionally there’ll be revolutionary ideas which will really completely change your view of science. And it is possible that some revolutionary breakthrough in our understanding will come about and we might crack this problem, but there’s no evidence for that. It doesn’t mean that there isn’t a lot of promising work going on. Eliminating senescent cells, and caloric restriction pathways, and cellular reprogramming and things like that,
and these factors in blood. So there are many legitimate areas which could lead to real improvements in health in old age. So I’m fairly balanced: I think there are promising areas, but there’s a lot of work to be done to see which area is going to be promising, and what the risks are, and how to make them work. Luisa Rodriguez: Right. It’s such early days. Before we move on, I’m curious what kind of gains you think we will get from ageing research in the next, say, 20 to 30 years? Venki Ramakrishnan: If I had to
venture a guess, I would say that some of these nutrient-sensing pathways, possibly removing senescent cells, are all things that might help us with some of the symptoms as we age. I don’t know how much they will actually buy in terms of lifespan. It may be that they simply keep us healthier for a bit longer, or even significantly longer, but that we all end up dying at about that same age. It could be that it pushes everything back a little bit, so we start living longer, but at the end we have the same decline that we
have now with all of the morbidities and problems of old age, but that we’ve postponed it by these treatments. So I wouldn’t be surprised if more people started living into their 90s, rather than, say, high 70s or low 80s today. Maybe more people start living into their 90s. That I think I wouldn’t be too surprised about. Luisa Rodriguez: And do you put much weight on ever increasing lifespan super significantly? Doubling it, for example? Venki Ramakrishnan: I think that would require really major breakthroughs in ageing. A number of gerontologists pushed back against all the hype in
ageing, and one of the things they did point out is that the brain is a particularly hard organ in which to prevent ageing. What would you do about the brain? Because neurons don’t typically regenerate at the same rate. It’s a very low rate of neurogenesis. So what would you do about an ageing brain? That’s a hard problem to tackle, and that today nobody seems to have a really good answer to. If we’re very lucky, we’ll be able to prevent diseases like Alzheimer’s. But I think really preventing ageing of the brain could be a big challenge,
and that would have to be overcome before we can think of extending that lifespan significantly. Luisa Rodriguez: That makes sense. You’ve actually just brought up Alzheimer’s, so maybe we transition to the ageing processes that cause diseases associated with the ageing brain. What happens in the brain when we get dementia? Venki Ramakrishnan: I think the problem with dementia is that — first of all, I should say it’s still being somewhat debated exactly what kills you when you get diseases like Alzheimer’s — but the most common view is that you have proteins that become defective. They’re misfolded,
and in the misfolded state, they start forming tangles or aggregates or plaques. And these plaques or tangles, when they accumulate in our cells of our nervous system, eventually kill the cells. There are a couple of compelling pieces of evidence for this. One is that mutations in these proteins can cause early onset of the disease. That suggests that these proteins, which manifest themselves in these tangles or filaments or plaques, are really related to the disease and have some role in causing the disease. There are two main candidates. One is called the amyloid-beta precursor protein, about which
most of the attention was given by the research community — partly because it was identified very early on as the major component of these plaques that Alzheimer himself observed many decades ago. Then there’s another protein, tau, which is an attractive candidate because it’s found inside the cells: the tau filaments are found inside the cells, and there are mutations of tau, which are also very highly correlated with onset of the disease. So that’s one area of evidence. Another area of evidence comes from recent work on the structure of these filaments. You could think of these proteins
clumping together as somewhat random, but it turns out these filaments are not random: they have very specific organisation, and the organisation of these filaments is dependent on what the disease is. For example, if you have Alzheimer’s, it’ll be different from if you have Parkinson’s or if you have Pick’s disease or various other diseases. That suggests that it’s really the specific structure of these filaments that somehow are causing the disease. Now, it’s not absolute proof, but I think it’s relatively strong evidence. But to be fair, there are also other minority views which suggest that disease is
really the result of inflammation or stress, and what these filaments are doing is raising that level of inflammation or stress, but they’re not really the actual cause of the death of these cells. For example, inflammation could be caused by other processes, including infection, and these protein aggregates may be an aggravating factor rather than actual cause of death. Some of this objection may be semantic, as what is the ultimate cause versus the proximal cause? There are all sorts of arguments going on about that. But nevertheless, I would say the broad majority of the community does believe
that it’s these proteins misfolding and aggregating that play some major role in the disease. Luisa Rodriguez: And do we understand why they misfold? Venki Ramakrishnan: Well, all proteins misfold, and we have various mechanisms to detect unfolded proteins and get rid of them via the unfolded protein response. There’s also something called the integrated stress response, which shuts down protein production when it senses unfolded proteins, so that you don’t accumulate more of them. And that gives a cell a chance to get rid of the ones that are there. The analogy I use is: if you have a
traffic jam, you don’t want more cars to enter the freeway; you want to shut down the cars entering the freeway so that your tow trucks have a chance of clearing the traffic jam before, and not letting it build up more and more. So there are these mechanisms that we have for dealing with this throughout our lives, but those mechanisms start failing with age, and the result is that we start accumulating these proteins with age. And of course, if we have mutations, then those mutant proteins have more of a propensity to unfold and cause aggregation, and
that’s why those people tend to get the disease earlier than most of us. Luisa Rodriguez: Right. OK, that’s really helpful. What do you think is the most promising idea for how to prevent those accumulated misfolded proteins? Venki Ramakrishnan: Some of the ideas are targeting these proteins involved in these filaments, like the beta-amyloid protein. What they’ve done is they’ve made antibodies to these proteins, and then they administer them in a way that they get into your brain, and then these antibodies simply deplete these proteins. The idea is that maybe you reduce the amount of plaque. Two
of them have been actually approved recently by the FDA. But to be fair, they don’t work all that well, and they have a number of side effects, such as brain swelling or bleeding. And really, the fact that there’s so much excitement about these drugs, really is a reflection of the fact that this is such a hard disease to treat, that there’s almost nothing out there. So even though these are not ideal drugs, people are excited about them. Luisa Rodriguez: Yeah, they’re something. Venki Ramakrishnan: I’m not sure how promising they will be in the long run.
I think there may be other ways of dealing with it. And one approach that’s being tried is an approach to selectively shut down the expression of these proteins in neurons. That is still at very early stages of research, and I think in the next few years we could expect to see trials. A third approach — which is still at an even earlier stage — is, now that we know the structure of some of these filaments, could you design compounds that block the formation of these structures by interfering with the interaction between the neighbouring proteins in
the filament that form the filament? And that is still very much an idea in very early stages. So I think, in general, it’s a very hard problem, and I would say possibly — and maybe I’m slightly biassed because it involves a technology called RNA, which is my own field; although I have nothing to do, by the way, with the company involved in that — but that technology, which has the potential to really slow down the expression or shut down the expression of the genes that are making those proteins, might well be promising in the sort
of middle term. I wouldn’t say short term, but the intermediate term. Luisa Rodriguez: Would you be up for explaining, kind of biologically, mechanistically, what the ideas are for inhibiting the expression of these proteins? Venki Ramakrishnan: Yeah. So the technology, I’ve heard — and this is all basically stuff I’ve just heard or read about — is a method called RNA interference, or siRNA. What you do is you introduce into the cell a small piece of RNA that’s complementary to the gene that you want to shut down, and it forms a small stretch of double-stranded RNA. And
the cell recognises double-stranded RNA and chops it up, and that then means that that protein is no longer made. So that’s really the basis of it. Luisa Rodriguez: Is it just that the cell naturally cuts up those double-stranded pieces for some unrelated reason? And so that’s how it would treat…? Venki Ramakrishnan: It’s a general viral protection mechanism. So the idea is that double-stranded RNA normally shouldn’t exist in the cytoplasm — and if it exists, it maybe has come from a virus. So I think it probably evolved as some sort of protection mechanism. But in any
case, it’s a very well-established mechanism. I think one of the main problems was, could you introduce this RNA into cells of the nervous system? And that’s where I think they’re making progress. Once they can establish that and they can test it, they can see if it has beneficial effects. Of course, they’d have to also see what shutting down these proteins — which presumably have a normal function — what that does to the functioning of these cells. Luisa Rodriguez: Oh, I see. In theory, those proteins are being expressed because they do something useful, so there’s a
question of what are they doing that would stop happening? Venki Ramakrishnan: Exactly. But I think those proteins, people have knocked down their expression in mice and found the mice don’t die or anything. Luisa Rodriguez: They’re relatively OK. Venki Ramakrishnan: They’re relatively OK. And of course, if the choice is between being slightly not OK and dying of dementia, I think that would not be much of a choice. Luisa Rodriguez: So those are some promising ideas for how to prevent or treat dementia. Are there any ideas out there that you think are overhyped and won’t lead anywhere,
but that nevertheless are getting lots of attention? Venki Ramakrishnan: No, I think there’s been so little progress in treating dementia that I don’t think… I mean, there might be in the alternative medicines space, but I don’t pay much attention to them anyway. Luisa Rodriguez: Sure. So, no widely popular…? Venki Ramakrishnan: I don’t think so. Although there are things that are supposed to help — for example, exercise and not being obese. Many of these things which are general drivers of ageing also help with dementia — and that’s because dementia is really very closely tied with ageing.
Luisa Rodriguez: Yeah. Would it be fair to say dementia is one of the more closely tied diseases of old age to ageing? Venki Ramakrishnan: Possibly. I think it only feels that way because the other ones — like heart disease and blood pressure and diabetes — are ones where we found solutions for; we know how to treat them. Luisa Rodriguez: I see. Venki Ramakrishnan: But otherwise, I think all of those could be considered. Luisa Rodriguez: They’re actually all very closely related. Makes sense. Pushing on, you mentioned cell senescence awhile back, and I’d be interested in talking
about that for a bit. I’m going to do my best to kind of say my understanding of it, and correct me if I’m wrong. My understanding is that when a cell senses DNA damage, it can either turn on repair mechanisms, it can kill itself, or it can send itself into a senescent state in which it’s no longer able to divide — and the accumulation of senescent cells seems to contribute to ageing. First, is that broadly kind of right? Venki Ramakrishnan: That is broadly correct. Now, early in life, senescence serves a useful purpose, because it eliminates
cells that are damaged — for example, if they’re damaged or stressed, they may be a cancer risk, or in any case, they’re not optimally working, and you need to get rid of them. By sending it into senescence, what happens is that these cells secrete a variety of inflammatory compounds, and these compounds basically attract the immune system cells to come and clear them and also clear the damage around them. Now, with age, what happens is that the immune system’s efficiency itself declines — because the immune system is also ageing, it’s no longer as efficient — and
this leads to an accumulation of senescent cells. So this compounds the problem, because when you have an accumulation of senescent cells, the inflammatory compounds can cause inflammation, they can cause damage to neighbouring cells, they can disrupt normal tissue function — and they can also spread senescence, because they can send nearby healthy cells into stress and induce them into going into senescence, and they can thereby spread. The whole thing also leads to not only loss of tissue function, but also chronic inflammation. So for all these reasons, senescent cells, when they accumulate with age, cause many of
the problems of ageing. This idea of senescence induced by telomere shortening, which is our chromosomes shortening, happens because our telomeres have a special structure, and when they get shortened, that structure unravels. So the cell then sees the ends of the chromosome and it can’t decide whether it’s a DNA break, a break in the chromosome, because it no longer has that special structure. So it senses it very much like a broken piece of DNA, and says there’s something wrong here, and sends it into senescence. So it’s very much related to this response to DNA damage or
to stress. Luisa Rodriguez: One area of research causing a lot of excitement in the ageing research community is removing senescent cells from the body. I’m interested in whether you think that area is promising or overhyped, but before we talk about that, can you explain what the proposed intervention is there? Venki Ramakrishnan: Since the accumulation of senescent cells with age is such a problem, for the reasons I just described, there was this idea that maybe if you get rid of senescent cells, that you would improve some of the symptoms of old age. People figured out in
clever ways how to target senescent cells, because they have certain markers that other cells don’t have, and they have a certain metabolism. So people figured out how to target senescent cells, and when they preferentially killed off senescent cells in mice, they found that these mice were healthier in many ways. They were more active, their hearts were more resilient to stress, they fended off cancers longer. They also lived about 20% to 30% longer. This has led to an area called senolytics, which is the idea of killing off senescent cells. And as with all areas of ageing
research, of course, there’s quite a lot of hype in the field, but I think there is also promise. But the caveat is, before it can be used in humans, you have to design drugs that are easily available, but that very specifically target senescent cells — that can reach them in your body if they’re administered, and they don’t target normal cells, and they don’t have side effects, they’re not toxic. So there are lots of the usual criteria for drugs that you need before you can use it for ageing. I should tell you that there’s a general
issue with anti-ageing therapeutics here. If you get cancer, you’re willing to take highly toxic drugs, because the alternative is you’re going to die very soon. And also, you’re only going to take the drugs for a short duration, until your cancer goes into remission. For other diseases, it’s even more so, like infectious disease. With ageing though, you have to take drugs over a very long time in the hope that it will somehow add to your healthy years of life. So you’re giving it to healthy individuals to prevent them from ageing. So the bar for anti-aging diseases
is much higher in general. Luisa Rodriguez: That makes sense. Venki Ramakrishnan: So I think a lot of anti-ageing therapeutics would be better advised to target diseases of old age — like osteoarthritis, atherosclerosis, or dementia — and they can target ageing processes, but aimed at one of these diseases where you have measurable outcomes and where the risks of not taking it are high, so it changes the equation. Luisa Rodriguez: Yeah, it does seem harder for me to imagine making the kind of tradeoff I’d need to make to take a relatively new drug that we hope will
remove my senescent cells when there’s nothing actually wrong with me, and maybe it’ll accidentally target other cells in the process. From memory, at least some of these interventions, when studied in mice, also seemed to only work really well when started at a very young age. I’m not sure if removing senescent cells is one of them, but I guess that also gives me another reason to pause in thinking about what it would actually concretely look like for people to take anti-ageing medicine that’s kind of generalised, if that means we have to take it at 10 or
15. Venki Ramakrishnan: I think that’s not always true. For example, we may talk about a drug called rapamycin, which is involved in the TOR pathway, one of the pathways affected by caloric restriction. And that drug, even when given to somewhat older mice, still seems to be beneficial in terms of ageing. Now, rapamycin will have other problems, and we can discuss that later, but the general point is that some of these drugs are useful even when given somewhat later in life. Of course, you can’t wait until the very end. They’re not some sort of disease cure
in the conventional way we think of it, because they’re trying to slow down or even reverse the process of ageing, and that takes some time. But I do think that many of these things can be given when you’re relatively old. Luisa Rodriguez: OK, noted. So in the case of senescent cells, the impression I’m getting from you is that the research does really look genuinely promising, but turning it into actual pharmaceutical interventions where the benefits outweigh the costs is where the main challenge is. Does that sound right? Venki Ramakrishnan: Yes, I think so. I think making
sure that the intervention is specific for senescent cells — or specific enough; it doesn’t have to be 100% specific, but specific enough so that at normal doses, you’re not affecting most of your cells, but you’re killing off most of your senescent cells — and then making sure that it’s relatively safe and nontoxic with no strange side effects. I think those are all things that need to be worked out and that can only be done with clinical trials. I suppose they could use these senolytic drugs to treat very specific diseases — for example, various kinds of
arthritis or other diseases of old age — as an initial step. Luisa Rodriguez: Right. Have they worked out how to do this reasonably well in mice, or are the mice kind of experiencing major side effects, and that’s why nothing’s moving? Venki Ramakrishnan: No, no, I think things are moving. In fact, there are lots of companies that have been set up with the idea of using senolytics, and there’s also a lot of basic research that continues to be carried out. So it’s not as if it’s hit some sort of roadblock; it’s just that the problems are
not trivial. But since there’s so much money being invested in the field, I’m optimistic that something will come out of it. Luisa Rodriguez: Wow. OK. So that one sounds genuinely promising. Let’s talk about caloric restriction, which I feel like is one of the areas of ageing research that I’ve heard the most about, and originally found most surprising. From memory, the earliest research done on it was looking into caloric restriction to find out how it might harm people — because presumably, if you starve people, they will be harmed. In this case I think it was mice,
but in fact they actually lived longer — which was, if I’m remembering correctly, a surprising result. Venki Ramakrishnan: Yeah. I think in the early days it was surprising because people felt you needed to have more nutrition in order to survive, and that if you consumed fewer calories, you would have all sorts of problems. And in fact, for most of our history, malnutrition was a big cause of death and ageing. So one of the reasons that life expectancy increased, say, 150 years ago, is that our food security and food supply increased, partly as a result of
using fertilisers. And that, in turn, meant that fewer people suffered from malnutrition and dying prematurely or dying of diseases of malnutrition. But caloric restriction is slightly different. In caloric restriction, you give the animal the bare minimum calories that it needs to survive without starving. So they don’t get malnourished; they don’t lose weight; they get all the nutritional supplements, vitamins, minerals, and so on that they need — but the bare minimum of everything else, like calories. And it turns out these mice tend to not only live longer, but they seem healthier in many respects. For example,
they’re more energetic, they have better skin and fur, their muscles are better. So all of these health parameters are better in these mice. So that’s a general phenomenon that has been observed over a long period, and it’s been reproduced in many species — even in very simple organisms like yeast, which is a unicellular organism. So it’s a broad phenomenon. Now, you have to remember that the experiment they’re doing often compares them to animals that have been fed a rich, all-you-can-eat diet. So there is some scepticism in some quarters about whether it’s actually caloric restriction that’s
so great for you, or whether it’s simply that an all-you-can-eat diet that’s very rich is actually bad. But regardless of that, what we can say, without a doubt, is that the number of calories you consume does matter. Luisa Rodriguez: And what do we know about the mechanism, the pathway? Why would caloric restriction slow ageing? Venki Ramakrishnan: Well, there are at least two or three major pathways that we’ve identified that are related to caloric restriction. One was somewhat accidental, which is called the TOR pathway. The TOR pathway was discovered because they wanted to understand how the
drug rapamycin worked. Now, rapamycin was found completely by accident by a group of Canadian scientists looking at soil samples in Easter Island, because they wanted to know why the natives of the island didn’t get tetanus, and they thought maybe there were compounds in the soil bacteria that protected them from tetanus. Out of those samples, one of the bacteria produced a compound which initially was found to be an antifungal compound. Then a scientist in Canada collaborated with other scientists at NIH and found it had some antitumour activities. And this scientist, Suren Sehgal, continued to work on
it and actually maintained interest in rapamycin. Eventually it was shown that it was an immunosuppressive compound and reduced inflammation. And based on that, it got FDA approval as an immunosuppressant for patients who were organ transplant recipients, so that they wouldn’t reject their graft. So then people wanted to find out how it worked. And a scientist named Mike Hall in Basel, Switzerland, he and two colleagues of his basically used yeast as a system to identify what the target of rapamycin was. They uncovered a pathway called the TOR pathway — “TOR” stands for “target of rapamycin.” It
turns out rapamycin inhibits a pathway that’s involved in maintaining growth. You need this TOR enzyme for the cell to grow, and it does that by continuously activating protein synthesis. And if you inhibit it, you also inhibit protein synthesis — but you also increase autophagy, which is this recycling pathway to get rid of defective cells. So that’s one pathway that’s affected by caloric restriction. The same pathway, it was later shown, senses nutrients, senses calories, senses sugars — but it also senses specific amino acids. So it’s not just caloric restriction; you can think of it as generally
a nutrient-sensing pathway. Now, another pathway was discovered by specifically looking for ageing mutants in worms. These mutants doubled the lifespan of worms. And again, these worms were not sickly and old-aged; they were relatively healthy — so they really did prolong their lives in a way that you would like to have them prolonged. Those mutants affected a different pathway called the IGF-1 pathway, which is a receptor for a hormone called the “insulin-like growth hormone.” You remember early on I said there are genes involved in growth and maturity that may cause ageing later on? This is one
such pathway. It turns out this TOR pathway and this IGF-1 pathway have this crosstalk — so they’re not truly independent pathways, but you can think of them as two hubs which are interconnected, say two airline hubs, but there are lots of flights between those hubs as well. You can see that there’s this complex metabolism that’s affected by caloric restriction, which had effects on ageing. Luisa Rodriguez: Interesting. Is there an intuitive way to explain why caloric restriction and these metabolic pathways would have the effect on ageing that they do? Is it something like the more use
that these metabolic pathways get, the more risk of wear and tear there is? Or something else? Venki Ramakrishnan: I think it’s a combination of effects. One is that caloric restriction definitely tamps down protein synthesis, and that perhaps prevents the accumulation of defective or unfolded proteins. It then also ramps up the recycling pathways that gets rid of defective components, including defective mitochondria. So that’s another beneficial effect. And there is some idea that maybe it’s reducing oxidative damage, or what’s called free radical damage, simply by affecting our metabolism. Of course, caloric restriction may be doing some other
things as well that are not yet well characterised, so we can’t rule that out. But certainly there are good reasons to understand why caloric restriction might be having its effect. Luisa Rodriguez: So, given that most people are not going to be excited about performing caloric restriction in their day-to-day lives — I certainly am not — what are some of the alternatives that ageing researchers are interested in for mimicking the effects of caloric restriction? Venki Ramakrishnan: People are looking at drugs which affect these pathways. For example, the darling of the anti-aging community is rapamycin, which is
an inhibitor of TOR and seems to produce many of the effects of caloric restriction in animals. That is to say, it improves many of the symptoms of ageing, it extends lifespan by some amount — and incidentally, it also works in mice that are relatively old. It would be like giving it to 60-year-old humans on a mouse scale. Luisa Rodriguez: That’s pretty amazing. Venki Ramakrishnan: So that means that you can take it even later in life, relatively speaking, and still obtain some benefits. But as I’ve pointed out, rapamycin is an immunosuppressing drug. It’s an FDA-approved drug
for organ transplant recipients to prevent graft rejection, and it makes you more prone to infections, slower wound healing. It has a number of other side effects. So it’s one thing to have to take it in order to prevent graft rejection — which is absolutely essential just to live — but it’s quite another thing to take it when you’re perfectly healthy, in the hope that it’ll extend your life by a certain amount. So I think the people who advocate it — and there’s also a lot of work on rapamycin analogues which might have some of the
beneficial effects without the ill effects; that’s still very preliminary — but the people who advocate it say that maybe you can give it at a dose where it still has beneficial effects on ageing, but doesn’t have these unwanted effects like immunosuppression and prone to infection and so on. So maybe there’s a sweet spot, but I think that needs to be established. There was one very interesting experiment that was being spearheaded by Matt Kaeberlein, who’s a well-known ageing researcher in Seattle. He used to be at the University of Washington in Seattle, but now I believe heads
up a longevity company of his own. He organised a study of domestic dogs. The problem with using laboratory animals is they’re kept in sterile environments and they’re highly inbred, so they don’t represent a real-life situation — whereas dogs are in as varied an environment as their owners. So you could register your dog, no matter where you were in the US, for one of these trials. And I don’t know what has happened to it. I think it had trouble getting funding or something, but I think it’s a good idea. It’s one way to actually see real-world
effects of rapamycin in a large-scale animal trial. So I hope they do find funding for it. Luisa Rodriguez: Neat. So that’s kind of the best case: they find some level which gives the benefits without the costs. Are there other avenues? Like treating the immunosuppression? Venki Ramakrishnan: No, I would say that’s harder. Another drug is already approved for diabetics, which is metformin. It’s a first-line drug for type 2 diabetes, and that also affects some of these pathways — because one of these pathways is insulin-like growth hormone pathway, and metformin is related to the whole area of
insulin sensitivity and so on. There, too, it’s not entirely clear whether it’s going to work well. There were early studies that suggested that diabetics on metformin actually lived longer and were healthier even than non-diabetics. This was very surprising, because diabetes is a risk factor. You would expect diabetics not to do better than non-diabetics. Luisa Rodriguez: Right. Venki Ramakrishnan: So that created some excitement. But those studies were then questioned in other studies which didn’t find that effect. In fact, those studies found that instead it was statins that had a big effect, and metformin really didn’t have
much of an effect. And metformin does have some side effects. I mean, clearly it’s safe enough to be approved for diabetics, and people take it all the time. But again, the equation is different. If you’re diabetic, it’s a serious condition. You absolutely should treat it, or you’ll have all sorts of negative consequences, including ageing. But you’ll also have organ damage and various other problems. So there’s no question, if you’re a diabetic, that metformin is a good alternative to take. But if you’re perfectly healthy, again, the equation’s different — and why would you have to take
it for a long time unless there’s very good evidence that the benefits outweigh any potential downsides? So there’s a large-scale study proposed. I think it’s ongoing or things are happening. And actually more than one, I would say. One of them, a very well-known study, is being done in New York, and I think we just have to wait for the data to see if it is going to be beneficial or not. But it hasn’t stopped some people from advocating it anyway. And since it’s available, people will often sort of off-target use. You know, they will use
it for anti-ageing; even when they don’t have diabetes, they’ll get somebody to prescribe it. I think that’s jumping the gun. It’s not rigorous science, and people should wait and do the trials properly. Luisa Rodriguez: Yeah. I feel like, on the one hand, I find that very persuasive. On the other hand, there is a part of me that is just really kind of blown away by some of the effects in model organisms, like mice, of some of these drugs. Maybe it would be helpful to hear why we should not immediately assume — which I think part
of me does kind of assume — that surely there is going to be some positive effect when they do this study, given how big these positive effects are in mice. Venki Ramakrishnan: Well, they are positive — but remember, the mice are kept in quite sterile environments. They don’t have the same problems we do. For example, if you’re more prone to infection, if you’re prone to not be able to heal wounds, that’s a major problem when you’re older. You get falls and burns and you can injure yourself. I think this is not a rational way to
proceed. And I think a lot of people are so anxious and obsessed about the idea of getting older that they’re just willing to take these risks and go ahead and do it. You know, I’m a fairly tolerant person. If they want to do it with their own body, you know, that’s their life. But I don’t think it should be approved in general without proper trials. And that’s because otherwise, people who don’t understand all the ramifications can be pushed into taking these sorts of things. There’s a lot of money involved too, which clouds the whole situation.
Luisa Rodriguez: Before we move on, another protein that plays a role in metabolic pathways that got the ageing community really excited is sirtuin. Can you talk a bit about sirtuin, and whether it’s overhyped or not? Venki Ramakrishnan: Well, it’s a somewhat controversial field. So a gene called sir2, which makes a sir2 protein, was shown to affect ageing in yeast. Now, you wouldn’t think yeast ages; it’s a single-celled animal. But it turns out that budding yeast — which is the kind of yeast that we use to bake our bread or brew our beer with — has
a large mother cell which buds off smaller daughter cells. So you can watch the mother cell and separate out the buds and keep the mother cell going. And it turns out that it can only divide a certain number of times, and then it goes into some sort of senescence. So you could think of that yeast cell as ageing, that mother cell is ageing, and you could actually study ageing in yeast. And this was a really innovative idea by somebody named Guarente at MIT. Then they looked for mutants to ask what would increase this replicative ageing.
One of the strongest candidates they came up with was this protein called sir2. The idea was that if sir2 was overexpressed, you would extend lifespan, or if you activated sir2, you would extend lifespan. This then led to a search for compounds that would activate sir2. One of the compounds was a compound called resveratrol, which was found in red wine and also found in various fruits, I think. So this created a lot of excitement, because there was always this idea that the French, even though they have a very rich diet, don’t get heart disease because they
drink a lot of red wine. But of course, you’d have to drink 1,000 bottles of red wine in order to get this dose of resveratrol, so it didn’t quite make sense, but there was a lot of excitement. But then other people, including people who originally came out of that same lab — like this fellow, Matt Kaeberlein and his colleague Brian Kennedy in Seattle — showed that this activation of resveratrol depended on a molecule that was used as a reporter for the activation assay and may have not had anything to do with activating sir2 at all.
Then other people countered that maybe there are similar molecules in the cell, et cetera. Then people found that if you activated the analogue of sir2 in worms or flies, then you extended their lifespan. But it turned out that this was a particular anomaly with the way that they did their genetics experiment — in the sense that in introducing these genetic variants, they’d also changed other genes, but if they kept the background exactly the same, then the effect wasn’t observed. So there’s lots of caveats. And the NIH did a large-scale study and found that giving mice
resveratrol had no effect on their longevity. So from my reading of the literature, and talking to various people involved in ageing research, I would say most of the community does not buy the sir2 story anymore. But I should say, in fairness, that the people who advocate sir2 have not given up. They’re sticking to their guns. But I would say, I call them “the faithful.” It’s only the faithful, the true believers who believe in it. Most of the community has sort of moved on from that. Luisa Rodriguez: Right. OK. It really does sound, if I understand
correctly, like it just fell apart in a bunch of different ways. Venki Ramakrishnan: And companies which really invested a lot of money in sirtuins — for example, Glaxo Wellcome, which bought one of these startup companies for a very large amount of money — Luisa Rodriguez: $720 million, I think? Venki Ramakrishnan: Exactly. I think they basically stopped that. They closed down that division, as far as I know. So nothing really has come out of it since it was done well over a decade ago, I think two decades ago. Luisa Rodriguez: OK, so it sounds like caloric
restriction is clearly relevant, has some promising lines of research, but is a case where there have been some that have kind of fallen apart. Venki Ramakrishnan: I think it’s probably a very promising area. It’s one of the more promising areas, and it fits in with a lot of things that we know about diet and moderation being generally good for you. Luisa Rodriguez: Neat! Another area of ageing therapy being explored is introducing Yamanaka factors into the body. If I understand correctly, Yamanaka factors are a set of four specific genes that encode proteins that “reprogram” a mature
cell’s epigenetic markers, so that they no longer necessarily only express the genes related to their specialised cell type anymore; they go back to being unspecialised and can in theory become any kind of cell. Can you explain what Yamanaka factors do in more depth, and how they might allow us to reverse ageing? Venki Ramakrishnan: Yeah, it’s a little complicated, and I have to backtrack a bit. When a fertilised egg develops, it becomes an early embryo. Eventually the embryo starts specialising into organs and tissues, and you get skin and hair and blood cells and bones and cells
of the nervous system and various organs and so on. The interesting thing is that that fertilised egg has in it the potential to form any of those tissues, because it eventually all came from that fertilised egg. But what’s also interesting is that even in some of the later stages, when it’s a mass of cells, the early embryonic cells, each one of those cells could become any type of cell. Those are called “pluripotent stem cells” — “pluripotent” simply means that they can become anything they want. Now, as they develop further, they become specialised stem cells. They’re
still stem cells, because they’re generating various kinds of tissues and not just dividing themselves, but they’re also differentiating. But they’re specialised stem cells. So we have hematopoietic stem cells, which can make all of the cells of the blood system — which means not only our red blood cells, but also all the cells of the immune system which are generated in the bone marrow. Those are hematopoietic stem cells. Other stem cells can generate all of the cells of the nervous system, including our neurons and glia, and various cells that make up our nervous system; others make
up our skin and hair and so on; others make up bone and cartilage. You get the idea. So these stem cells are now more specialised. They can still make different types of cells, but it’s a narrower subset. They can’t make everything. Like a hematopoietic stem cell can’t make neurons, for example. And then you have the finally differentiated cells, which are the neurons or the skin or the various different types of white blood cells. Those cells, when they divide, they can only divide and be more of their own types. They can’t even generate different subtypes. These
fully differentiated cells can also only divide a certain number of times because of telomere shortening and other things. They can undergo a certain number of divisions, where stem cells can divide much more often, many more times. So that’s the basic picture. Now, as we get older, these stem cells also go into senescence, and we lose stem cells. So we lose the ability to regenerate tissue — and that’s essential for life, if we want to maintain muscle mass, maintain skin, maintain our organs. There’s a rough saying that every cell in your body is replaced every seven
years. Of course, some organs are very slowly replaced. And some tissue, like the heart, a lot of it is not replaced. That’s why heart attacks are so serious, because those muscles don’t just automatically regrow. Whereas if you get a cut, your skin simply regrows and heals. So that’s the rough picture. Now, what Yamanaka factors do is: each of these specialised cells are specialised because they have their own genetic program. So the skin cell expresses the kinds of genes it needs to be a skin cell; the neurons have a different program, so it expresses a different
subset of genes. Of course, all the cells express some genes that are required in every cell just to carry out the basic functions of life, but then they have these specialised subset of genes that they express. So what Yamanaka factors do is they alter that genetic program, and they can in fact take a fully differentiated cell all the way back to a pluripotent cell. These are called “induced pluripotent stem cells,” or iPSCs. Now, these iPSCs, in principle, can then be induced to form any other kind of cell. So you could in principle take a skin
cell, take it all the way back to a pluripotent stem cell, and then persuade it to grow into some other kind of cell. Which you couldn’t do before. You could never convert — Luisa Rodriguez: That does seem pretty incredible. Venki Ramakrishnan: It is amazing. And of course it’s a huge industry, because you can imagine it has all kinds of uses. For example, as we get older, we lose cartilage. If we lose cartilage in our joints, we get osteoarthritis. We have people who have diabetes because they lose their pancreatic cells that make their insulin. Or if
you have a heart attack, maybe you have heart muscle that’s damaged and you would like to regenerate it. You can see the possibilities are enormous. So the stem cell industry, which is what’s called regenerative medicine, is a huge industry — billions or hundreds of billions of dollars. And it’s been around for a while, and it’s had some successes — perhaps not as many as one might have hoped, but definitely has had some successes. But the idea is that maybe you could use this for ageing. And I would have thought this was rather improbable, but it
didn’t stop some scientists from applying Yamanaka factors to animals. And if you take it all the way back to pluripotent stem cells and you introduce these pluripotent stem cells in animals, they often will form tumours. Not always, it’s rather context dependent, but there’s always this underlying risk of cancer — because two of these factors are actually oncogenes, so they’re effectively involved in proliferation and growth. So in order to avoid the risk, what they did was to give these Yamanaka factors transiently to the animal so that they wouldn’t go all the way back, but they would
just go a little way back, but perhaps regenerate the kind of stem cells they need that were being depleted, and maybe regenerate these tissues. But in any case, these mice, originally they did it with these mutant mice, which are called progeric mice. These are mice that age prematurely. They looked to see the effect, and they saw all sorts of positive effects. Then they did it with wild-type or non-progeric mice — ordinary, normal mice — and they saw similar effects. So I would say this is a promising area — and it’s the only area that could,
in principle, even think of reversing ageing. Many other things would slow down or prevent ageing. This might, in fact, reverse the clock. But of course, like all of these things, it’s very early days. We’re at the threshold of something. There’s a lot of very smart people who’ve gone into it. Many of them quit their jobs in academia and joined major longevity companies like Altos Labs, which is funded by a bunch of billionaires and has branches in California and also in Cambridge here in England. So they attracted some very good brains. There’s a lot of money,
and I wouldn’t be surprised if something eventually comes out of it. But again, it’s extremely hyped and people are not coming to grips with how would you deliver this? Our organs age at different rates. How would you make sure that you’re doing this reprogramming in a safe and efficient way? Also, what about the risk of cancer? Of course, it hasn’t prevented people from trying all sorts of strange things like having stem cell injections and so on. None of this is FDA approved or anything, but people are offering it. Luisa Rodriguez: OK, so there’s clearly some
amount of hype that at least isn’t justified yet. On Yamanaka factors in particular, it seems like there is some early promise. And I’m pretty fascinated by them, so I actually am interested in asking a few more questions. For one, is a mechanism — at least in mice, and that people would be hopeful to see in humans — basically just that you introduce Yamanaka factors into the body and they basically allow — Venki Ramakrishnan: They essentially reset the genetic program because they’re transcription factors: they’re involved in turning on various genes, and they can reset the genetic
program. And in doing so, they’re really effectively reversing development of these cells. Luisa Rodriguez: So they’re allowing more of them to become these pluripotent or semi-pluripotent cells, so that they can continue to do the regeneration that stops happening as often later? Venki Ramakrishnan: That’s right. Luisa Rodriguez: It does seem pretty wild to me that you’d see benefits. You didn’t actually explain the intervention, but I’m kind of just picturing, I don’t know, an intravenous syringe or something, and then they’d just be somewhere in the body. Do you introduce them to the particular organ? How do you
kind of get them where they’re supposed to be? Venki Ramakrishnan: No, I think they’re systemic. Luisa Rodriguez: They are. Wow. Venki Ramakrishnan: They’re introduced in a systemic way. Luisa Rodriguez: If I read this in a science fiction book, I wouldn’t believe you that it had these effects. Venki Ramakrishnan: I was frankly pretty astonished myself. But there’s no question, and it has been done by several groups now. There was a group in Cambridge, a group in Spain, and the original finding I think was done in San Diego. So I think the effect is definitely real. I’m
not sure they actually extended the lives of these animals by much. They improved many of the symptoms of ageing. I think it’s one of these things where there’s lots of early, exciting results, but it needs to be followed up. Luisa Rodriguez: Sure. How worried are you about the potentially cancer-causing effects? Do you know if there’s any promising research to curb those? Venki Ramakrishnan: I think it’s always a worry. I mean, if you’re introducing genes that are known to be oncogenes and overexpressing them, it’s always a worry about what will happen over the long term. You
know, giving something transiently to mice over days or weeks is very different from if you have to interfere with our own biology over the long term. So I’m sort of open minded about it. I think it’s an exciting area. I think the whole cellular reprogramming is an exciting area, but I don’t know enough about it to know what the risks are. I just feel, given what we know about teratoma formation with iPSCs in some cases, the fact that these are oncogenes means that we need to proceed cautiously. And I think it’ll need a lot more
animal trials before it’s ready for any kind of clinical trials in humans. Also, you would want to use it only for conditions where there’s a real health problem. You would do that first, before you would use it in a general way for arresting ageing in the general population. Luisa Rodriguez: Right, right. So you can imagine these being used to treat diabetes in patients who… Venki Ramakrishnan: Or people who do have certain syndromes which cause premature ageing. Luisa Rodriguez: Oh, right. I see. Venki Ramakrishnan: Which are real diseases. You could perhaps see if they help with
that. But I think even that is a long way off. I think it’s some way off. They would need a lot of work in animals and understanding mechanisms and dosage and things like that before they go to humans. Luisa Rodriguez: OK, turning to another topic: why does our risk of cancer go up as we age, and why do we die of cancer? Venki Ramakrishnan: So, just as I’m not a person who works on dementia, I’m also not a cancer biologist, but I’ll tell you my understanding of it. Cancer seems to be a problem of regulation
of the cell. Normally, our cells divide, they form tissues; and then they at some point stop dividing, or they divide at a very slow rate in order to live as a community, as part of the tissue — and the whole system then lives in harmony as an individual. Now, when that regulation is lost, the cell starts dividing without constraints and really hijacks resources to itself. For example, when a tumour grows, it also secretes factors that encourage the growth of blood vessels to grow into the tumour, to keep supplying it with blood, so it can keep
growing even faster, and keep on growing. It’s really a system that’s gone out of control and starts taking over in an abnormal way. This prevents not only the normal functioning of organs, but it also sometimes destroys those organs entirely by invading their tissues and just taking over. And this loss of control of regulation is because the program of expression of our genes has been affected, and that then is the result of damage. It’s a result of damage to our DNA that accumulates with age, or rearrangements — so DNA breaks and gets recombined, and you get
rearrangement of genes or chromosomes. Or it can have to do with modification of our chromosomes. So our DNA is constantly being modified, and the proteins associated with our DNA are also modified. This is part of a phenomenon called epigenetics — because it’s not actually the DNA sequence itself that’s being affected, but it affects the way in which you express those genes. All of these, when they go wrong, can cause cancer. And because these damages and changes accumulate with time, the risk of cancer goes up with age. Luisa Rodriguez: Yeah. So that all makes sense to
me. I think I just had a surprisingly poor understanding of, mechanically, why we then die of cancer. And maybe it isn’t the same in all cases, but can you say a little bit about that? Venki Ramakrishnan: I think ultimately it’s because it takes over our entire system and prevents the function of critical organs. For example, if you get liver cancer or kidney cancer or pancreatic cancer, those organs can’t function, but it also then invades all the other tissues. So you simply can’t function as an individual, and you get a critical systems failure. That’s really what
happens. Luisa Rodriguez: Right. And from your book, it seems like a big piece of the cancer puzzle is the protein p53, which is a tumour-suppressor gene. You note that almost 50% of all cancers have a mutation in p53. Can you explain the relationship between p53 and cancer? Venki Ramakrishnan: Our cells are constantly subject to DNA damage, and we have very elaborate mechanisms to repair the damage: first of all to sense the damage, and then to repair it. And p53 is a protein that’s normally inactive, but when the cell senses DNA damage, it activates p53. That
p53 then turns on various genes, because it’s what we call a “transcription factor,” which affects the transcription of mRNA, which is the copying of genes into mRNA, and thereby make proteins that those genes encode. The response to p53 is a huge range of effects. For example, it can arrest cell division. It can then turn on DNA repair. Or if the damage is very extensive, it can even trigger cell death, which is called “apoptosis.” Or it can send cells into senescence. If you have a potentially cancerous cell and you send it into death or senescence, you’ve
eliminated the risk from that cell. Or if it’s not too bad, you can repair it and you can arrest cell division while you’re repairing the damage. So it’s a very general response, and that’s why mutations in p53 are found in so many cancers. Luisa Rodriguez: Right. Because the mutation will mean that p53 doesn’t do all of that — what seems like really an impressive array of cancer-addressing functions. Venki Ramakrishnan: Yeah, and that’s because it’s a transcription factor which affects the expression of key genes, each of which affects a different aspect of this whole broad response.
Luisa Rodriguez: Yeah. That makes sense. Does that help in the treatment of cancer, to know exactly the kinds of things p53 might be failing to do that we could try to recreate? Venki Ramakrishnan: I mean, p53 has been the subject of investigation. I’m not an expert on this, so I don’t really know to what extent. But I will tell you one very interesting thing. Cancer is caused by defects in our DNA, so you would think that interfering with DNA repair would be a bad thing for treating cancer, because it would cause more defects and that
might lead to more cancer. But it turns out that that is actually a target for cancer. So some cancer drugs actually affect our ability to repair defects in the DNA. The reason is that many cancer cells already have several defects in their repair machinery, and they’re accumulating mutations quite rapidly. So if you affect their ability to do DNA repair, then they’re more likely to die than your normal cells — because our normal cells might have other options for repairing DNA, but you may be closing off the options for these cancer cells. So many recently approved
cancer drugs actually are inhibiting DNA repair in some cases. Luisa Rodriguez: That is fascinating. Venki Ramakrishnan: Of course, you wouldn’t want to use these drugs in healthy individuals, because you wouldn’t want to block DNA repair over an extended period. But of course, if you have cancer the equation’s different, because you’re taking it for a short time to kill off your cancer cells. Luisa Rodriguez: Yeah. That is really interesting. Before we move away from p53, I was just really fascinated by the observation that elephants and whales have way more copies of the p53 genes than humans,
and I think also get way less cancer. Am I getting that right? And is there any more to add there? Venki Ramakrishnan: I think the paradox is that they’re larger animals, so they have many hundreds or thousands of times more cells than, say, a mouse does. And yet a mouse is much more prone to cancer than an elephant. So why is that? Because if you have many hundreds of times more cells, the chance that one of your cells becomes cancerous will be that much higher. And, of course, all you need is one cancerous cell to
proliferate, and then it’ll kill you. So you would think the more cells you have, the more likely you should get cancer. But in fact, that’s not true. These large animals actually have a lower rate of cancer. And this is something called Peto’s paradox, after a scientist named Richard Peto. It turns out that these large animals, like elephants, have about 20 copies of the p53 gene, so they have a much higher amount of p53 floating around. This means they’re more sensitive to sensing DNA damage and stress, and therefore they’re better at preventing cancer from developing in
the first place, and that’s probably what protects them. And very large animals like blue whales also have other DNA repair enzymes that seem to be prevalent in them. Luisa Rodriguez: Interesting. This is just a very uninformed question, but do you think it’s at all plausible that eventually there will be genetic therapy that either repairs mutations to the p53 gene, or even that inserts more copies of it? Is there any line of research there? Venki Ramakrishnan: Yeah, I don’t know what the consequence would be. I think these things are all an evolutionary balance. If you have
a lot of p53, just to give you a hypothetical example, you might generate lots of senescent cells. So I think everything has been balanced with these evolutionary tradeoffs. An elephant has a different physiology from what we have, so if you did the same thing to us, it might not be the same effect as an elephant, because the elephant has other things that are different about its metabolism. So I think this is not something you could predict. You have to try it and see in model systems. Luisa Rodriguez: That makes sense. And maybe there are, in
fact, reasons why we could have more p53 genes, but we don’t because there are some tradeoffs that we’re not aware of. Can you talk about how our mitochondria are involved in ageing? I guess starting with what are mitochondria, for those who have a vague memory, but not a super clear one? Venki Ramakrishnan: Mitochondria are organelles in our cells, and they arose in an interesting way. About 2 billion years ago, one of our ancestral cells swallowed up a bacterium. And normally, when that would happen, either the bacteria would die or the cell that swallowed up the
bacteria would have bitten off more than it could chew and it would die. But in this particular case, this combination survived and the bacterium reproduced inside the larger cell, and the larger cell kept dividing. And eventually, all of the descendants of that combination resulted in what we call “the higher life forms,” which includes us. And the bacterium eventually evolved into an organelle called mitochondria. These mitochondria are specialised. They’re where the high-energy molecule of the cell, called ATP, is produced. This ATP you can think of as a molecular battery: anywhere where you need energy in a
reaction, it uses ATP to help drive that reaction. That ATP is produced in mitochondria. So in that way, you can think of mitochondria as the energy factories of the cell, where energy is produced. Luisa Rodriguez: And then what happens in an ageing mitochondria, or what causes mitochondrial dysfunction, and what kinds of effects does that have on the human body? Venki Ramakrishnan: So mitochondria not only are responsible for energy production, but they also are sensors of the state of the cell. They’re very intimately tied with our metabolism: they can sense the overall energy levels of the
cell, control what’s going on throughout the cell. When mitochondria stop working or don’t work efficiently, then the rest of the cell also suffers. It suffers from not having enough ATP, but it also suffers in many other ways. And as we age, our mitochondria become defective. The reasons why mitochondria are particularly sensitive to age: one is that this is where oxidation of sugar or fat occurs. So oxygen that we breathe in eventually makes its way into our mitochondria, and that’s where molecular oxygen is actually used to oxidise sugar. Complete oxidation, you get carbon dioxide and water.
If you get incomplete oxidation, you can get these partial species called reactive oxygen species, this partially reduced species — and they are highly reactive, and they can cause damage all over the mitochondrion, including to the mitochondrial DNA. Remember, they’re descendants of bacteria, so they have their own genome. That genome has shrunk over the 2 billion years, but they still encode really critical genes for mitochondria to be able to survive. So that’s one reason. The other reason is that it causes defects in our mitochondrial DNA, and that effect can also result from replication of the mitochondrial
DNA causing defects. But for whatever reason, mitochondria become defective and they stop working well, and that then leads to the cell not working well, and generally leads to ageing. Luisa Rodriguez: Great. This really brings me back to my biology courses. What area of research are people most excited about for addressing mitochondrial dysfunction? Venki Ramakrishnan: There are many areas. One was the idea that if oxidation is causing all this damage, maybe antioxidants are a good thing. There were early experiments which suggested that maybe antioxidants could help with the ageing process. The idea of oxidative damage causing
ageing, there’s quite a lot of evidence for it — although what people have found is that if you take antioxidant supplements, that’s not necessarily going to help you. Now, that doesn’t mean that the oxidative damage theory itself is wrong. It may simply mean that these supplements don’t work in the way that you want them to, they don’t get to where they’re needed, and they don’t necessarily neutralise the species that are potentially causing the damage. So just the fact that supplements don’t work doesn’t mean that the whole idea is wrong. That’s one avenue. The other is
that as mitochondria become defective, the cell can get rid of them and potentially regenerate them. The way that the cell gets rid of them is a process called “autophagy” — where entire defective mitochondria are taken and made to go into an organelle called the lysosome, which basically destroys them and recycles those components. As we get older, those mechanisms also don’t work as well. But some of the pathways that are involved in ageing, one of them, by interfering in those pathways, also improves autophagy. It increases autophagy and that then helps with recycling of all sorts of
defective compounds, including mitochondria. And then there are ideas of how to maybe regenerate mitochondria or help regeneration of mitochondria. Interestingly, regular exercise is thought to help with regeneration of mitochondria, along with many other beneficial effects. There are some promising avenues for it, but I don’t see that there’s a particular drug on the market now, or even a target that’s close, but it’s certainly a major area of research. Luisa Rodriguez: So for exercise, do we have any idea how that helps repair mitochondria in particular? Venki Ramakrishnan: One is the idea that exercise may turn on these
pathways, like autophagy. But another is exercise also induces mechanisms of regeneration and repair, and that then also benefits us more broadly than just mitochondria. Exercise has a number of benefits. It also reduces stress, which itself accelerates ageing. So there are numerous benefits to exercise. Luisa Rodriguez: Yeah, I was struck by that. It felt like almost every chapter of the book had an “…and exercise helps.” And it got me on a mini exercise kick, which hopefully lasts. OK, let’s push on to our final topic. We haven’t yet discussed the question of whether we should try to
extend human lifespan in the first place. So let’s spend at least a few minutes talking about that. One potential impact of increasing longevity is radically changing the shape of the population pyramid, with fewer young people alive relative to the number of older people. What do you see as the potential social ramifications of changing that population pyramid? Venki Ramakrishnan: I think if people live longer, that means a larger fraction of society will consist of older people relative to younger people. So that ratio of young people to old people will change. It’s particularly true that fertility rates
continue to drop. Most Western societies are well below replacement age — and countries like the US are only able to maintain population because of immigration, otherwise the US population would also start to decline. This means that you absolutely need to keep older people healthy, otherwise they’re going to be an incredible burden on the rest of society. It’s also not going to be pleasant for them to keep living longer if they’re not going to be healthy. So there’s a lot of effort to keep them healthy. It might involve things like work. I mean, what are all
these people going to do? You can’t have a smaller and smaller fraction of the population supporting old people who are in retirement. So there’s the question of what’s going to happen to careers, and will you have to change retirement age? I know in the US there isn’t really a formal retirement age, but are you going to change expectations of how long people can work? There are lots of issues with this. One is that we all face cognitive decline. Cognitive decline starts from when we’re very young; it doesn’t just happen when we’re old, although it’s more
obvious when we’re older. But in the early part of our lives, we compensate for cognitive decline with knowledge and experience. So we’re often more productive: even if we have cognitive decline, we’ve compensated in other ways. But there reaches a point where we’re not gaining much in terms of knowledge or experience; we already know a lot and we’ve experienced a lot and we’ve plateaued out there, but we’re undergoing cognitive decline. And then you do see real decline. So that’s one problem. Another problem is older people hang on to their jobs, whether it’s a faculty job, or
being a corporate executive, or being the chief executive of the United States. There’s a question of generational fairness, because you are actually preventing somebody younger and more able from filling that job. So I think this is going to create a number of issues in society — both in terms of making society more livable and accessible for older people, but also what to do about these things. My feeling is that as we get older, we should sort of adapt to different roles: we don’t have to do the same job we did when we were in our
20s and 30s and 40s. We can slowly adapt to a role, and as we get older we can do things that are still useful but not actually taking resources and opportunities from younger people. Luisa Rodriguez: So if I’m understanding, it’s something like if we achieve more significant life extension, older people will want and/or need to be employed, which might mean they keep jobs that otherwise younger people would be getting. And one, maybe they’re not the best people to be doing those jobs anymore; and two, there’s a question of fairness. Is it kind of naive to
think that the economy will expand because there will be more overall workers, and that it’ll kind of figure out how to allocate that labour such that the economy grows, and that’s actually a good thing? Venki Ramakrishnan: It is possible. I mean, we live twice as long as we did, on average, say, 150 years ago. And nobody would want to go backwards and say we all want to have a life expectancy of 40. Luisa Rodriguez: Exactly. Venki Ramakrishnan: So I think it’s possible, but it’s an adjustment that needs to be made, and it needs to be
thought about and it needs to be done in a way that’s fair across generations. And maybe the economy will expand, but if the population doesn’t expand, it’s not clear that the economy will continue to expand in the same way. Yes, you may get productivity gains by other methods — AI or automation, things like that — but there is a real question about what the effects will be. Luisa Rodriguez: Yep, that makes sense. You also argue that increasing longevity could in theory increase inequality. Can you say why that is? Venki Ramakrishnan: I think almost every medical
advance has benefited rich people before it’s benefited everybody else, and often rich countries before it has benefited poor countries. You can see that all the way from early measures like public health and sanitation, to fertilisers and food supply, to antibiotics to cures for cancer, heart disease, et cetera. The result is that today, even in rich countries, the top 10% economically live almost 15 years more than the bottom 10%. My stepdaughter, who’s in public health in New York, pointed out that if you looked at New York City alone, people in the richest ZIP code live 35
years more on average than people in the poorest ZIP code. Of course, this is not just due to ageing, because a lot of it is due to infant mortality, poor health, poor healthcare throughout their lives, crime, poor nutrition — so there are many factors that affect this. But longevity and ageing, I’m sure, is one of them — and many of the things that we can do to stay healthy in old age are not as easily available to poor people. So there is this disparity. Now, imagine if you have treatments that are very sophisticated and only
wealthy people can afford them, or people with good insurance: then you will dramatically increase this disparity in life expectancy or lifespan. And it’ll have knock-on effects, because the rich people will live longer, and the wealth you accumulate roughly depends on how long you live. They’ll keep accumulating wealth throughout their lives, and they will pass on greater wealth to their offspring, and then those people will also live longer. So you can just see how you can get a divergence between rich and poor. And you might get two classes of citizens: rich people who live very long
and have healthy lives, and poor people who have short and relatively unhealthy lives. I should point out that even today, not only do the rich live longer, but they live a larger fraction of their lives healthy: their healthy years are even more than the poor. So the poor not only live shorter lives, but they live unhealthier lives as well. You can see how all of these things are going to potentially create big differences — unless we do things to combat that. For example, by having universally accessible healthcare and good environments, education, preventive health, public health,
primary care. If we were able to distribute these evenly across the population, then that would be a big help. Luisa Rodriguez: Yeah. So given those risks, do you have an all-things-considered view on whether extending human lifespan and healthspan is worth doing? Venki Ramakrishnan: I think it’s not a question of what I think. If scientists find out ways to extend lifespan in a healthy way — I mean, nobody wants to extend lifespan and just be miserable for 30 years — but if they can extend the number of healthy years that we live, it’ll be impossible to
stop. Because once the technology is there, who’s going to say, “I’m not going to use it”? If somebody came to you with a pill and said, “If you take this pill, you’re going to have 10 extra healthy years of life,” most people would take it. So I think it’s not really something you can… Once knowledge is out there, you can’t unknow things, and you can’t deliberately say, “I’m not going to use it” — because other people will use it, even if you don’t. Luisa Rodriguez: OK, we have time for just one more question. I’d like
to ask you: what is the biggest thing you changed your mind about or that surprised you while researching Why We Die? Venki Ramakrishnan: So, I came with a naive idea, which many people have, which is that ageing happens because it benefits the species or the group — because you want each generation to get out of the way so that the next generation can try different combinations of genes and survive. And of course, once I looked into it and read about it, it doesn’t make sense evolutionarily. Ageing is not actually programmed; it’s a sort of byproduct
of the way selection works. It’s because there’s no mechanism to select, there’s no reason to select against ageing up to beyond a certain point. So that was one surprise. The other thing, that somewhat follows from that, which is another big thing, was that the limits to our lifespan are not based on some chemical or physical law, and certainly aren’t programmed for each species, but rather the result of evolution and the balances it has chosen for each species. So knowing that, it means that, in principle, you might be able to change that situation that evolution has
selected for. So those are a couple of surprising facts that I found. Luisa Rodriguez: Those are great. Just on that, I’m actually curious: what was it that convinced you that it is not actually evolution selecting for population turnover? What about that didn’t check out? Venki Ramakrishnan: When you look at this phenomenon called group selection, where the idea is that you can select for things that benefit the group, it turns out that’s a phenomenon that only works if the group are all genetically related. For example, bees in a hive are all essentially clones of one another,
so each gene will affect all of the members of the individual. Otherwise, you have a phenomenon called “cheaters” — evolutionary cheaters. The simple example is that if you had a gene, let’s say there was a program that told you that this genetic program is what makes you age and die at this rate. And now you get a mutation that makes you live longer. Well, that mutation would allow you to live longer and therefore reproduce more, and would be selected for, so it would quickly overtake the population. So the idea of group selection doesn’t really work,
except in very special cases where the group’s very closely related. And that’s something that I began to understand in the course of [writing] this book. Luisa Rodriguez: Yeah, that’s really interesting. OK, I will let you go. My guest today has been Venki Ramakrishnan. Thank you so much for coming on. It’s been a pleasure. Venki Ramakrishnan: Thank you. Luisa Rodriguez: If you liked this episode and want to learn more, or if you’re interested in hearing arguments for even more radical life extension than Venki thinks is plausible, check out our interview with Laura Deming on the science
that could keep us healthy in our 80s and beyond. All right, The 80,000 Hours Podcast is produced and edited by Keiran Harris. Audio engineering by Ben Cordell, Milo McGuire, Simon Monsour, and Dominic Armstrong. Full transcripts and an extensive collection of links to learn more are available on our site, and put together as always by Katy Moore. Thanks for joining, talk to you again soon.
Related Videos

2:46:55
Does Consciousness Extend Beyond Brains? T...
Holberg Prize
4,704,653 views
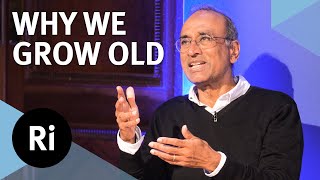
57:19
In search of immortality - with Venki Rama...
The Royal Institution
43,063 views

3:29:56
Dr. Peter Attia: Improve Vitality, Emotion...
Andrew Huberman
2,670,166 views
2:33:02
Graham Hancock: Lost Civilization of the I...
Lex Fridman
2,442,517 views

1:45:22
Can We Slow Down Aging? Venki Ramakrishnan...
The Proof with Simon Hill
26,635 views
1:02:30
Venki Ramakrishnan, "Why We Die: The New S...
Harvard Science Book Talks and Research Lectures
103,350 views

1:22:11
Alpha Waves Heal Damage In The Body, Brain...
Healing Energy for Soul
26,369,418 views

3:11:18
Robert Greene: A Process for Finding & Ach...
Andrew Huberman
14,046,617 views

1:45:01
Revelații despre CREIER Neuroplasticitate,...
George Buhnici
115,957 views

1:37:34
The Groundbreaking Cancer Expert: (New Res...
The Diary Of A CEO
3,167,355 views

2:10:43
Dr. David Sinclair: The Biology of Slowing...
Andrew Huberman
3,440,324 views

3:59:42
Brian Keating: Cosmology, Astrophysics, Al...
Lex Fridman
8,278,710 views

1:01:06
Na Rubu Znanosti - Znanost sudnjeg dana
ARHIVANRZ
31,444 views

1:43:38
Social change is often abrupt & unpredicta...
80,000 Hours
523 views
49:54
Venki Ramakrishnan: The New Science of Aging
Eric Topol
4,401 views

1:26:30
Rewiring the Brain: The Promise and Peril ...
World Science Festival
697,814 views
4:14:59
The economy and national security after AG...
80,000 Hours
11,079 views

3:43:02
Pharaoh - Kings of Ancient Egypt documentary
The People Profiles
433,486 views

47:00
5 Amazing Foods That Regenerate Stem Cells...
Shawn Stevenson
17,096 views
27:53
Venki Ramakrishnan: The most promising way...
New Scientist
28,122 views