Pharmacology - HYPERTENSION & ANTIHYPERTENSIVES (MADE EASY)
1.79M views1962 WordsCopy TextShare
Speed Pharmacology
👉📖 READY TO ACE YOUR EXAM? 📚 GET STUDY NOTES ON PATREON!
https://www.patreon.com/speedpharmacolog...
Video Transcript:
in this lecture I'm going to talk about pharmacology of antihypertensive drugs so let's get right into it hypertension or high blood pressure is a quite common disorder affecting many people who typically don't even notice any symptoms now in order to gain a better understanding of pharmacology of antihypertensive agents first we need to review a basic physiology of blood pressure regulation so when we talk about blood pressure we are generally referring to the force or tension of blood pressing against the artery walls now this pressure in the arteries is maintained by among other things contraction of
the left ventricle systemic vascular resistance elasticity of the arterial walls as well blood volume in other words blood pressure is simply a product of cardiac output and systemic vascular resistance there are a couple of major systems involved in blood pressure regulation first arterial blood pressure is regulated by pressure sensitive neurons called baroreceptors located in the aortic arch and carotid sinuses so for example if blood pressure falls too low those baroreceptors can send signals to the adrenal medulla causing release of catecholamines and thus increase in sympathetic activity through activation of alpha and beta receptors so activation
of beta-1 receptors causes increase in heart rate and stroke volume and thus increased cardiac output which leads to increase in blood pressure on the other hand activation of alpha-1 receptors on smooth muscle causes vasoconstriction and thus increase in vascular resistance which again leads to increase in blood pressure now another major system involved in blood pressure regulation is the renin-angiotensin-aldosterone system so we also have baroreceptors in the kidneys that respond to fall in blood pressure or reduction of blood flow by releasing enzyme called renin additionally renin secretion is also stimulated by sympathetic activation of beta-1 receptors
in the kidneys now renin is necessary for the production of angiotensin II angiotensin II is a very potent vasoconstrictor which constricts systemic blood vessels thus increasing peripheral resistance angiotensin II also constricts renal blood vessels and stimulates aldosterone secretion which leads to sodium and water retention thereby increased blood volume cardiac output and ultimately increased blood pressure now let's switch gears and let's talk about antihypertensive agents so there are several major classes of antihypertensive drugs which work by interrupting different parts of this blood pressure regulating system first we have alpha-1 blockers such as Doxazosin and Prazosin which
block alpha-1 receptors on the smooth muscle thus causing decrease in systemic vascular resistance and ultimately decrease in blood pressure next we have selective beta blockers such as Atenolol and Metoprolol which selectively block beta-1 receptors on the heart thus causing decrease in cardiac output and thereby decrease in blood pressure as you may remember we also have non-selective beta blockers such as Labetalol and Carvedilol that can additionally block alpha-1 receptors and thus simultaneously decrease vascular resistance furthermore beta blockers can inhibit beta-1 receptors present on the kidneys and thus suppress release of renin formation of angiotensin II and
secretion of aldosterone so these effects result in decrease in systemic vascular resistance and again fall in blood pressure to learn more about alpha and beta blockers make sure you check out my video about adrenergic antagonists now the next major class of antihypertensive agents are centrally acting adrenergic drugs which work by blocking sympathetic activity within the brain example of drugs that belong to this class are Clonidine and Methyldopa now Clonidine selectively stimulates presynaptic alpha-2 receptors thus providing negative feedback to reduce catecholamine production and release this leads to decrease in systemic vascular resistance and cardiac output and
ultimately decreased blood pressure Methyldopa on the other hand also lowers blood pressure through the same mechanism however unlike Clonidine it is not an agonist itself so first it must be converted to its active metabolite called methylnorepinephrine now let's move on to another major class of antihypertensive agents that is calcium channel blockers so calcium channel blockers are divided into two main subclasses dihydropyridines and nondihydropyridines now dihydropyridines selectively inhibit L-type calcium channels in the vascular smooth muscle under normal conditions when calcium enters the smooth muscle cell it causes it to contract which leads to increased vascular resistance
and thus increase in blood pressure so when dihydropyridine drug blocks the entry of calcium into the vascular smooth muscle cell the contraction is inhibited which leads to decreased resistance to blood flow and thus lowering of blood pressure example of drugs that belong to this group are Amlodipine Felodipine Nicardipine and Nifedipine when it comes to side effects of dihydropyridines they're related to systemic vasodilation so you can expect dizziness headache flushing and peripheral edema another side effect that may occur with this class is swelling of gums also known as gingival hyperplasia now let's move on to nondihydropyridines
which are non selective inhibitors of L-type calcium channels in other words they are not only capable of blocking calcium channels on vascular smooth muscle but also calcium channels on cardiac cells such as those of SA node and AV node which leads to reduced myocardial contractility slower heart rate and slower conduction that's why these agents exhibit significant antiarrhythmic properties for more details make sure you check out my video about antiarrhythmic drugs now it's important to remember that even though decreased heart contractions typically result in decreased cardiac output nondihydropyridines do not significantly decrease cardiac output most likely
because of the reflex tachycardia that occurs as a result of vasodilation currently there are only two drugs that belong to this group namely Diltiazem and Verapamil now when it comes to side-effects nondihydropyridines can cause excessive bradycardia and cardiac conduction abnormalities additionally Verapamil which happens to be the least selective calcium channel blocker can exert significant inhibition of calcium channels in the smooth muscle that lines the GI tract which can lead to constipation now the next major class of antihypertensive agents are diuretics there are three major classes of diuretics that are used in the treatment of hypertension
first we have loop diuretics such as Furosemide which work by reducing reabsorption of sodium chloride in the kidneys leading to significant diuresis with less volume in the vascular space less blood returns to the heart so cardiac output decreases this in turn leads to decrease in blood pressure particularly in patients with volume-based hypertension and chronic kidney disease secondly we have thiazide diuretics such as Hydrochlorothiazide which also reduce reabsorption of sodium chloride in the kidneys but to a much smaller degree than loop diuretics this leads to initial decrease in intravascular volume decrease in cardiac output and ultimately
lower blood pressure however the long term effects on blood volume are minimal and sustained antihypertensive effects are thought to be produced by thiazide induced vasodilation lastly we have potassium-sparing diuretics such as Triamterene and Spironolactone which increase diuresis by either interfering with the sodium potassium exchange in the kidneys or by blocking the actions of aldosterone potassium-sparing diuretics are often used in combination with loop and thiazide diuretics to reduce loss of potassium that can occur with the use of these drugs for more details make sure you check out my video about diuretics now let's move on to
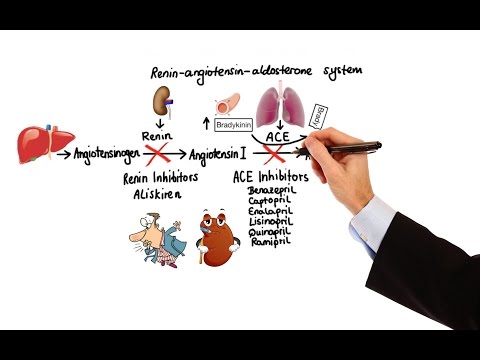
another group of antihypertensive agents that is agents that work on the renin-angiotensin-aldosterone system so here we have three pharmacological targets that can be used to reduce the activity of angiotensin II which is ultimately responsible for causing blood pressure to increase first we have renin the enzyme responsible for conversion of angiotensinogen to precursor of angiotensin II that is angiotensin I so renin is the target of renin inhibitors which selectively inhibit this enzyme thus decreasing production of angiotensin II the example of drug that belongs to this class is Aliskiren secondly we have angiotensin-converting enzyme that is responsible
for conversion of angiotensin I to angiotensin II this enzyme is the target of ACE inhibitors so just like inhibition of renin inhibition of angiotensin-converting enzyme also leads to decreased production of angiotensin II however what makes ACE inhibitors different is that in addition to lowering angiotensin II levels they can also elevate bradykinin levels bradykinin is a peptide that causes blood vessels to dilate by stimulating the release of nitric oxide and prostacyclin however normally angiotensin-converting enzyme inactives bradykinin so it's inhibition leads to bradykinin induced vasodilation the example of drugs that belong to this class are Benazepril Captopril
Enalapril Lisinopril Quinapril and Ramipril finally we have angiotensin II receptors type 1 or AT1 receptors for short so binding of angiotensin II to these receptors is actually responsible for most of the effects of angiotensin II including vasoconstriction and stimulation of aldosterone release these receptors are the target of angiotensin II receptor blockers or ARBs for short the example of drugs that belong to this class are Candesartan Irbesartan Losartan Olmesartan and Valsartan so in summary the agents that work on this renin-angiotensin-aldosterone system either block the production of angiotensin II or block its actions on the AT1 receptors
this in turn leads to decreased systemic vascular resistance but without significant changes in cardiac output additionally these agents reduce the effects of angiotensin II on renal hemodynamics specifically angiotensin II constricts the efferent arteriole thereby generating back pressure in the glomerulus which can lead to injury so by reducing activity of angiotensin II these agents also improve renal blood flow and thereby reduce the risk of renal injury now when it comes to side effects because these agents suppress aldosterone release their use can contribute to development of hyperkalemia furthermore ACE inhibitors in particular may cause dry cough or
in rare cases angioedema which can be life-threatening this is thought to be due to increased levels of bradykinin and substance P now before we end this lecture I wanted to briefly discuss few other antihypertensive agents that do not fall into any of the classes that we covered thus far so first we have Bosentan which is a competitive antagonist of a potent vasoconstrictor called endothelin-1 which acts on the endothelin-A and endothelin-B receptors located on pulmonary vascular cells by blocking the action of endothelin-1 on these receptors Bosentan leads to vasodilation which decreases pulmonary vascular resistance for that
reason Bosentan is often a drug of choice for treatment of pulmonary hypertension next we have Fenoldopam which is a selective dopamine-1 receptor agonist the dopamine-1 receptors are located on the smooth muscle cells in the peripheral vasculature as well as the renal coronary cerebral and mesenteric arteries by stimulating dopamine-1 receptors Fenoldopam produces generalized arterial vasodilation which leads to decreased peripheral resistance and thus lower blood pressure additionally Fenoldopam inhibits tubular sodium reabsorption which results in natriuresis and diuresis due to its rapid onset of action and short duration of action Fenoldopam is often used in the hospitals for
short-term management of severe hypertension another fast-acting agents that are also used for hypertensive emergency are Sodium Nitroprusside and Nitroglycerin which simply serve as a source of nitric oxide a potent peripheral vasodilator lastly we have direct acting smooth muscle relaxants namely Hydralazine with mechanism of action that has not been entirely determined yet and Minoxidil which works by stimulating opening of ATP-activated potassium channels in the smooth muscle which leads to membrane stabilization making vasoconstriction less likely while these agents significantly decrease peripheral resistance they also produce significant compensatory reflex tachycardia and renin release for that reason these drugs
are typically administered in combination with a diuretic and a beta blocker on the flip side topical application of Minoxidil promotes hair growth which is why this drug is used more often for treatment of baldness rather than hypertension and with that I wanted to thank you for watching I hope you enjoyed this video and as always stay tuned for more
Related Videos

17:19
Pharmacology – HEART FAILURE (MADE EASY)
Speed Pharmacology
431,235 views

18:04
Pharmacology - DIURETICS (MADE EASY)
Speed Pharmacology
1,033,175 views
![Antihypertensive Drug Chart: Pharmacology Made Easy [Classes, Medication Trick, Mechanism of Action]](https://img.youtube.com/vi/owcZmS5KwHw/mqdefault.jpg)
16:08
Antihypertensive Drug Chart: Pharmacology ...
EZmed
516,069 views

13:50
Renin Angiotensin Aldosterone System (RAAS)
Zero To Finals
8,153 views

27:12
Authorities reveal cause of death for acto...
ABC 33/40
1,578,254 views

18:58
#1 Best Way to Lower Blood Pressure Natura...
Dr. Ford Brewer
445,346 views

23:16
Pharmacology - ANTIARRHYTHMIC DRUGS (MADE ...
Speed Pharmacology
1,657,276 views

8:13
11 MISTAKES Measuring Your BLOOD PRESSURE ...
Violin MD
806,270 views

7:46
Elon Musk Cold Open - SNL
Saturday Night Live
14,999,711 views

14:29
Pharmacology - DRUGS FOR HYPERLIPIDEMIA (M...
Speed Pharmacology
1,118,952 views
17:17
Pharmacology - DRUGS FOR DIABETES (MADE EASY)
Speed Pharmacology
1,610,073 views

24:07
Jon Stewart on Trump’s Heel Turn on Zelens...
The Daily Show
7,384,368 views

10:40
Even Canada Shocked By Mexico's Bold Move ...
PPR Mundial
119,677 views

20:05
How To Lower Your Blood Pressure (Cardiolo...
Talking With Docs
1,940,949 views

11:48
'My jaw is dropped': Canadian official's i...
CNN
4,981,614 views

16:46
How do Calcium Channel Blockers Work? (+Ph...
Drug Chug
229,977 views

10:02
Antihypertensive Medications | ACE-Inhibit...
NurseInTheMaking
230,004 views

11:42
Ex-CIA Director predicts chilling effects ...
MSNBC
180,831 views

21:34
GLOVES OFF: Jasmine Crockett drops NIGHTMA...
Brian Tyler Cohen
1,203,593 views
41:56
Hypertension | Clinical Medicine
Ninja Nerd
284,129 views