🥇 Anatomía del ESÓFAGO, Fácil y Rápida
259.34k views3020 WordsCopy TextShare
Anatomía Fácil por Juan José Sánchez
Descarga esta y cualquier diapositiva de mi canal, uniéndote a PATREON!
También puedes unirte a los ...
Video Transcript:
Welcome to a new easy anatomy video by Juan José Sánchez! Today we will talk about one of the organs that begins what is the digestive tract. We will talk specifically then about the anatomy of the esophagus.
So, in this video we will mainly address its macro structure, we will talk about its generalities, its portions, the most important anatomical relationships. Then, we will talk about its irrigation, its venous drainage and, of course, its innervation. Don't detach yourself from the video.
[Music] I invite you to subscribe here in the lower right style, click. [Music] And don't forget to like the video. So, basically, the esophagus is a muscular tube that begins the digestive tube that connects an important portion of the neck, such as the pharynx, with the stomach.
So it goes through three important structures of the body, it goes through the neck, it goes through the thorax to finally reach what is the stomach and take the bolus. So, from the throat to the stomach, this tube measures approximately 25 to 30 centimeters, somewhat less thick and smaller in women since this portion of the body is less developed. It basically begins at the level of the lower edge of the cricoid cartilage, that is the anatomical reference for me to say here the esophagus begins and that is specifically at the level of the C6 vertebra and ends approximately between D11 and D12 or also called T11 and T12 , that is the length with respect to the spinal column.
So, we are going to delimit 3 portions and we are going to explain each of them separately. First, the portion more proximal than its superior portion is the cervical portion. Then, the longest portion, which is the intrathoracic portion, and finally, its shortest portion, which is the abdominal portion.
So these are then going to be the three portions of the esophagus. It is very important that we know that there are strictures of the esophagus, they can be places where the esophagus narrows. It is normal that anatomically it narrows in those places , there are precisely anatomical structures that put pressure on it and that is why it has those narrownesses that look very good, I repeat, in radiological anatomy.
For example, when we make a barium esophagus, the first place at the first narrowness, which at the narrowest point of the esophagus is precisely at its beginning, that is, the lower edge of the cricoid cartilage at the level of C6, that is the first narrowness. There it joins the pharynx and that is why that region is called the cricopharyngeal region where the tendon of the cricopharyngeal muscle is located. Then, we have the second construction that some authors vary here.
Some authors say that it is the aorta, the arch of the aorta, that makes this constriction and they call it aortic constriction. Others say that specifically it is the left main bronchus, the Netter that I took this image from anatomy, the Netter says or names this second constriction as aortobronchial constriction, that is, for that author this constriction is made by both the left main bronchus and the arch of the aorta. And the third stricture is the stricture that occurs when it perforates the thoracoabdominal diaphragm.
So, we are going to call them diaphragmatic constriction. Those are the three places where anatomically we are going to see that the tube, the esophagus, narrows a little, basically reducing its lumen. So, let's start by explaining the cervical portion.
In this sagittal cut, we are going to see that it begins at the level of the lower edge of the cricoid cartilage, this is the anterior part of the cricoid, this is the posterior part. See that at the lower edge there it begins. I say that the esophagus begins, that is at the C6 level and you count the vertebra.
This would be that one that circles c2 c3 c4 c5 and see that at c6 the esophagus begins. It is a continuation, as I told you, of the pharynx but let's be more specific, it is a continuation of the lowest part of the pharynx, which is called the laryngolarynx. Then, after the laryngopharynx, when it reaches the lower edge of the cricoid, it becomes the esophagus and begins the muscular tube already called the esophagus.
As you can see in this image, this would be the inferior constrictor muscle of the pharynx. Notice, the lowest part This one that is shaded here in green from the lower concept of the pharynx is called the cricoesophageal tendon because it comes from the cricoid cartilage to the esophagus. Some authors call them cricopharyngeal tendon.
This cricopharyngeal tendon is the muscular part of the inferior constrictor that is attached to what is the beginning of the esophagus and there is so much pressure on this muscle when it contracts that it is what forms the first sphincter that I We find it in the digestive tract, which is the upper esophageal sphincter, you know, and then the upper esophageal sphincter is formed by the tendon of the cricopharyngeal muscle. A sphincter is nothing more than a valve, that is, it closes the beginning of the esophagus so that the bolus, once it passes, cannot be returned. We are going to see here how the esophagus is always in posterior relation to the trachea, so much so that it is joined by this fibroelastic tissue to the posterior part of the trachea.
Here we basically see the tendon of the cricopharyngeal fiber forming the upper esophageal sphincter and delimiting me from the beginning of the esophagus. So, there is a very important relationship between the esophagus and the trachea, the trachea is always in front of the esophagus, this is a relationship that never changes. Now the trachea begins to deviate towards the right side of the midline and the esophagus does the opposite, the esophagus begins to deviate towards the left side.
There is also a very important relationship with the primitive carotid arteries, this primitive carotid is so lateral to what is the esophagus and with the thyroid gland, specifically its anatomical lobes that have a lateral relationship with respect to the esophagus. Let's see it well in this image, we see that the esophagus is always posterior to the trachea and is always anterior to the spinal column. In fact, they describe it as if it were a bow with its string, the esophagus with respect to what is the spinal column.
Now, there is something quite important that at the cervical level, as I told you, the trachea moves towards the right side and the esophagus a little more towards the left side. This means that at the cervical level only the trachea covers the right half of the esophagus. But it does not cover the left half because they are not both precisely in the midline.
This is why when a surgeon is going to approach the neck to reach the esophagus, it is easier for him to reach the esophagus by cutting through the left side of the neck than to cut through the right side, because he knows that if he cuts through the right side The trachea is obtained first, then the esophagus. On the left side it is free, on the left side the esophagus is free, so it is easier to access it from the left side of the neck. Here we can also see the relationship that exists with the common carotid arteries that are lateral.
In this posterior view we basically see the pharynx that is the beginning of the esophagus, this would be the cricopharynx tendon and see how the anatomical lobes have a lateral relationship. He talked about the anatomical lobes of the thyroid gland, which is the beginning of the esophagus. Also lateral to the esophagus are the parathyroid glands.
Look at these nerves, which is why I brought up this image and are the recurrent laryngeal nerve. This nerve, apart from innervating the upper portion of the esophagus, which is a branch of the vagus nerve, is a very intimate relationship , it enters its way up between the trachea and between the esophagus, it is a very important relationship that the esophagus has. We see this axial short at the level basically between c5 or c4 c6 and what I shade in red is the esophagus so it is in the trachea.
See here the relationship it has with this nerve, which is the recurrent larynx, with this gland that is half seen here, which is the parathyroid, and with all of this, which are the anatomical lobes of the thyroid. See that it is posterior to the esophagus so there will be the vertebral column and these muscles that are the prevertebral muscles. What we see here is basically the primitive carotid also as a lateral relationship to the esophagus and this would be the sympathetic chain also as a posterolateral relationship to the esophagus.
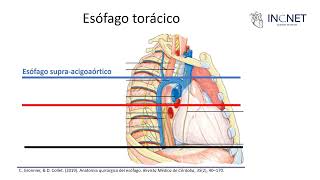
As I always say, the trachea in front of the esophagus, that never changes. So with respect to the cervical portion, we are going to move on to the thoracic portion, which is the longest of the esophagus. This thoracic portion is characterized because its beginning, like the cervical portion, is clearly striated muscle, that is, we can contract at will, when we swallow it is at will that we move the pharynx muscles.
However, the most distal portion of the thoracic region, when the esophagus reaches the abdomen, is smooth muscle so that we can no longer control it at will but it is only controlled by the autonomic nervous system. So, basically, the trachea in its descent through what is the thoracic cavity is crossed, although it is not seen in this image, by the left main bronchus. The left main bronchus is anteriorly related, as is the trachea itself.
As I already explained, the esophagus theoretically comes to the left and the trachea to the right, while the right main itself has nothing to do with the esophagus, the other quite important relationship you have with the aorta. Note that the beginning of the aorta, that is, the ascending aorta, is first anterior to the esophagus. The arch of the aorta is rather lateral, while the descending aorta is first lateral, but then suddenly becomes posterior, so posterior that when both structures, I mean the esophagus and the aorta, pierce the thoracoabdominal diaphragm, the esophagus pierces it.
In front, it passes through the esophageal hiatus, while what is the aorta does so behind. So, imagine the very important relationship that the esophagus has with the aorta, now we are going to see it in a much better image. Another quite important relationship with this plexus, the esophageal plexus, formed mainly by the vagus nerve.
Ok? See that the vagus nerve has both an anterior and posterior relationship with the esophagus. This artery here, which is the famous pulmonary artery, is also an anterior relation to the esophagus.
We see here the relationship, so important, is a posterior view of the vagal trunks. This would be the posterior vagal trunk, since the anterior vagal trunk that innervates and turns the esophagus. In this image you can see very well the relationship that exists, as I explained, anterior ascending aorta, arch of the lateral aorta and the descending aorta first laterally, but then it becomes posterior in what is the esophagus.
An also important relationship with the heart, in fact, there is a space that is seen radiologically between the heart and the esophagus, the retrocardiac space, which is very important for you to know. Now let's move on to the abdominal portion, the nominal person which is the shortest, appears when the esophagus perforates the esophageal hiatus of the diaphragm. This abdominal portion is very important for you to know what to disappear, you were like that which disappears, because in swallowing, when we swallow, the trachea rises and the pharynx rises.
As the esophagus is attached to the pharynx, the esophagus also ascends so that when I swallow this abdominal portion to become part of the thoracic portion and it simply disappears, even a part of the stomach also ascends to the thorax, I am going to explain how that mechanism occurs. So in this abdominal portion is where the esophagus ends, approximately at the level of the D11 vertebra, emptying into the cardia portion of the stomach. This junction is called the gastroesophageal junction.
The line you see indicates the change from the esophageal epithelium to the gastric epithelium, and is known as the Z line or zig-zag line because of its shape. Now, see that there is a thickening in the distal part of the esophagus and that forms the lower esophageal sphincter, so we have an upper one that forms the cricoesophageal muscle and a lower one that is basically formed by a thickening of the walls of the esophagus itself, See that in this esophageal hiatus, this is the diaphragm, okay? It is joined by a ligament that is the brake ligament, brake is an adjective that means diaphragm, so this ligament is called the phrenoesophageal ligament.
It is what makes it so that when you swallow and the abdominal portion of the esophagus disappears because it rises, since it is quite elastic, it quickly pulls it downwards and the esophagus returns to its abdominal portion again. What you see in the image is a cushion of fat that is inside the phrenoesophageal ligament. We are going to talk about the irrigation of the esophagus, a densely irrigated organ like all the organs of the target tube.
From top to bottom, first is the inferior thyroid artery with its esophageal branches. Then, we see that the aorta gives off bronchial branches and, through that bronchial branch, it also takes advantage and gives branches to the esophagus. So, those are the bronchial branches of the bronchial artery.
Then, some branches that are direct from the aorta, that is, the aorta, as it comes out, allows direct branches to give to the esophagus, to a branch, then, aortic. And in its final part, this artery that is here, which is the branch of the abdominal aorta, that diaphragmatic artery, also called the inferior phrenic artery, that inferior phrenic artery. See that it also gives some twigs to what is the esophagus, as you can see here.
Now, another artery that is also responsible for supplying the esophagus is the diaphragmatic or inferior phrenic artery. Not seen in this image. But like this, as this is lower diaphragmatic, there is one that gives the aorta before perforating the esophageal hiatus, the aortic hiatus gives it up here and that also helps to irrigate the esophagus.
Lastly, this branch of the celiac trunk, which is the left gastric artery, also called the coronary stomatal artery, helps to irrigate the lower portions of the esophagus. So you see that it is a densely irrigated organ. Venous drainage is very important since two venous systems of the body converge in the esophagus.
Notice that what you see like this, here in dark blue, are basically the azygos vein that drains part of the esophagus, the hemiazygos vein and the accessory hemiazygos vein upwards, the posterior intercostal or posterosuperior veins drain what is the most esophagus, as does the inferior thyroid vein. So, all of this venous drainage searches in some direct or indirect way for what is the superior vena cava to reach what is the right chamber of the heart. That is the famous systemic circulation, that of the entire body, it is the one you see here in dark blue.
But something very important is that the lower part of the esophagus formed by the left gastric vein, this left gastric vein, you will see that they drew it here in a more blue and that is because it drains not into the systemic circulation system but into the of the portal circulation of the portal vein. So it drains into the portal vein. This means that in the lower part of the esophagus there is an anastomosis, that is, a union between both circulations is the systemic and the portal and somewhere, as you can see here, the portal systemic anastomosis, where the veins can dilate, forming the famous esophageal varices.
Well, and that would be clinical, it is not part of the video, but just so you know why there is often bleeding from varicose veins in the lower part of the esophagus when there is blockage or damage to the portal vein, basically it is because there is an anastomosis between the two systems . Finally, the innervation of the esophagus is an organ of the digestive system. Obviously, it is controlled by the autonomic nervous system.
The peripheral cannot control it because we move the esophagus at will. Its parasympathetic innervation is given as I told you, but the anterior and posterior vagal trunks are the precarious holm oaks and moles in the ganglia that are on the internal walls of the esophagus and from there the post ganglionic cells come out to innervate the esophagus itself. .
They are the ones that are basically in charge of peristalsis, that is, esophageal movement, and they are also basically in charge of the secretion of the glands. While the sympathetic innervation is given by the trunk or sympathetic chain, the pre-ganglion fibers come from the spinal cord, reach these vertebral ganglia and from there are entangled in the sympathetic area and then the esophagus. The function of the sympathetic is to do the opposite, that is, to stop the movement of the esophagus and stop the secretion of the glands.
So friend, this has been the entire video. Do not forget Subscribe to the little circle that appears here and like and share it too. You can follow me on Instagram at @ juan_sánchez1315.
Thank you for your attention.
Related Videos

19:39
🥇 Anatomy of the STOMACH. Easy, Quick and...
Anatomía Fácil por Juan José Sánchez
297,325 views

Soothing water music to sleep 🌺 Stress-re...
Peaceful drops of water

18:20
🥇 RESPIRATORY SYSTEM in 18 Minutes!!. Eas...
Anatomía Fácil por Juan José Sánchez
445,380 views
23:59
Embriología, anatomía y fisiología del esó...
INCNET
2,700 views

18:37
🥇 Anatomy of the DUODENUM. Easy, Quick an...
Anatomía Fácil por Juan José Sánchez
250,048 views

2:29:19
LEGENDARY MELODIES YOU COULD NEVER GET BOR...
Spanish Strings
9,239 views

16:10
🥇 DIGESTIVE SYSTEM in 16 Minutes!!. Easy ...
Anatomía Fácil por Juan José Sánchez
372,782 views

13:30
ANATOMIA DEL ESOFAGO
Profesor Matias Rodriguez
884 views
13:30
ANATOMÍA: Aparato Digestivo - Parte 1
Facultad de Ciencias Médicas
352,900 views

17:58
🥇 Anatomy of the PANCREAS and PANCREATIC ...
Anatomía Fácil por Juan José Sánchez
264,690 views

47:41
Fisiologia respiratoria 🫁 | Primera parte
TiagoMed - Dr. Santiago Sambracos
45,961 views

Gentle Spa Piano🌿 Relaxing Music with Nat...
Peaceful drops of water

27:32
🥇 ANATOMY OF THE TONGUE. Easy and Simple ...
Anatomía Fácil por Juan José Sánchez
178,625 views
18:23
VIDEHISTO #38 | Sistema digestivo I - Esófago
Histología 2 FMed UBA
13,626 views
25:05
Anatomía del Abdomen - Pared abdominal (MÚ...
Medizi
48,832 views

19:08
🥇 Anatomy of the YEJUNO-ÍLEON, (Small Int...
Anatomía Fácil por Juan José Sánchez
164,645 views

44:06
Fisiología del estómago
Sinapsis EMP
145,149 views

13:13
🥇 Anatomy of the TRACHEA. Easy, Quick and...
Anatomía Fácil por Juan José Sánchez
217,074 views
23:30
🥇 PERITONEUM 1/3. Generalities and Divisi...
Anatomía Fácil por Juan José Sánchez
258,971 views

18:11
🥇CIRCULATORY SYSTEM in 18 Minutes!! (Card...
Anatomía Fácil por Juan José Sánchez
631,609 views