Growth Hormone (GH) - Somatotropin - Dwarfism, Gigantism, Acromegaly - Endocrine Physiology
50.15k views5285 WordsCopy TextShare
Medicosis Perfectionalis
Growth Hormone (GH) Somatotropin, Dwarfism (short stature, stunted of growth), Gigantism, Acromegaly...
Video Transcript:
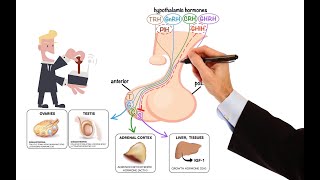
hey guys it's medicosa's perfect status where medicine makes perfect sense containing our physiology playlist in previous videos we talked about genomic versus non-genomic action or how the hormones work on a molecular level and we talked about the famous anterior pituitary and we learn that it secretes TSH act h g h which is the growth hormone FSH LH and do not forget prolactin just remember that in order to grow you need growth hormone and you need the middleman somato Maiden C which is insulin-like growth factor one growth hormone comes from the anterior pituitary igf-1 the middleman comes from the liver now let's get started please watch the videos in this physiology playlist in order recall that we have a CEO and then underneath we have the general manager underneath we have the employees similarly here is the hypothalamus followed by the pituitary and then the employees that listen to the pituitary are thyroid adrenal cortex and gonads they glands that do not care about the pituitary or the parathyroid Adrian medulla and endocrine pancreas and we talked about the fact that these hormones tend to be slower because they are more likely to be fat soluble however the independent contractors tend to have faster actions because they have water-soluble hormones all of this was discussed before remember embryology yeah do you remember my trilometer embryo endoderm mesodermin ectoderm where did the anterior pituitary come from answer ectoderm how about the posterior pituitary enter also ectoderm but different kind of ectoderm recall that the ectoderm is made of surface ectoderm for the epidermis of your skin on the outside and neuro ectoderm which is the nervous system now let me ask you a question which part of the pituitary is neuro I. E the neuro hypothesis enter it's the posterior pituitary and that's why the posterior pituitary comes from the neuroectoderm however the anterior pituitary comes from the surface ectoderm surface ectoderm is for the epidermis of your skin and other organs such as the epithelium of the mouth that's important and the oral cavity also important and the neural ectoderm which is the nervous system recall that the anterior pituitary secrete these hormones the posterior pituitary does not make anything it borrowed two hormones from the hypothalamus and these are ADH and oxidose is why these are unique why these came from the hypothalamus why not from the interpretuitary like the rest of them because they had to come from the hypothalamus since they are related to memory functions so they gotta be closer to memory organs and memory centers example Ada age increases after I lose blood in a car accident do you think I should learn from my mistake and remember this in the future so that I stop being so distracted while crossing the road yeah that's why ADH had to come from the hypothalamus also oxytocin had to come from the hypothalamus because it's important for memory it's important that the female human forgets the pain of a child bearing and the pain of Labor in order to be pregnant again to continue the population note that the population replacement rate should be about 2. 1 children per woman for Humanity to break even without population growth or population decline the anterior pituitary is glandular we call it Adeno hypothesis it secreted its own secretion however the precipituitary is not an actual gland it did not synthesize ADH it did not make oxytocin it borrowed them from the hypothalamus okay how did ADH and oxytocin make their way from the hypothalamus to the posterior pituitary they are neurons put differently the connection between hypothalamus and anterior pituitary is bloody but the contact between hypothalamus and precipituitary is nervous that's why the anterior pituitary is known as adenohypophysis but the posterior is called neuro hypothesis okay better coasters I got you but why hypothalamual hypophysical portal circulation what does the word portal mean a portal system is any system consisting of two capillary beds in series here's the first bed here is the second bed of capillary and between them there is a door there is a channel there is a shunt dor is La Porte Porta portal system medicosis is so multilingual it's unbelievable so before this blood can reach the heart it needs to go to LA port and then to the second capillary bed that's why it's called portal system and then this door will let you to go back to the hot okay but the coasters do I have many portal systems in the body well you have some the kidney is one example the liver is the most important example and don't forget my anterior pituitary hypothalamo from the hypothalamus hypophysical to the pituitary and between them there is a door there is a shunt there is a channel there is a path portal circulation please recall that a collection of cell bodies or Somas in the CNS is called the nucleus when the same collection happens in the peripheral nervous system it's called a ganglion a collection of axons in the CNS is attract in the pns it's a nerve note that the connection between my hypothalamus and the posterior pituitary was done by means of axons that's why it's called a hypothalamo hypophysical tract oh there you go here is you attract a collection of axons in the central nervous system see medicine makes so much sense once you understand what the flip you're talking about where did the anterior pituitary come from surface ectoderma where did the posterior pituitary come from neuro ectoderm okay medicosis which part of the surface ectoderm are we talking about remember that the surface ectoderm was responsible for the mouth and the oral cavity right so therefore the Adeno hypothesis basically is an extension from your future mouth the stomodium what does the word stoma means mouth let's go back to your science classes do you remember this Leaf yeah it had pores in it what was the name of the pores stomata teeny tiny mouths holes in the leaf but of course your science teacher did not tell you that that's why he's just a teacher not a YouTube persona sorry I take it back here is my anterior pituitary it came from this timodium the roof of this timodium via the wrathkis pouch which will go upwards okay that's my future interior pituitary from the roof of this timodium okay we got it how about the precipitivity well it's part of the diencephalon going down in an infundibulum so anterior pituitaries here plus your pituitaries here the next step is that both of them will hug and kiss each other fuse together so that you have one pituitary gland under your hypothalamus because their hypothalamus is part of the diencephalon it makes sense of course it does here is my lovely anterior pituitary secreting growth hormone elatin FSH TSH ACTH and prolactin how do we influence the interpituitary Via releasing and inhibiting factors coming from the hypothalamus if you want the pituitary to make more growth hormone hypothanamus will secrete growth hormone releasing hormone or releasing peptide if you want to secrete less growth hormone give me the famous Universal inhibitor somatostatin somatostatin is the same doofus that we talked about in GI physiology it inhibits everything and here is no exception it also inhibits growth hormone secretion after growth hormone is released from the anterior pituitary what will it do it will go to the liver and will tuck the liver into making the middleman somato because this is somatotropin maiden mediary like a bunch of lawyers going to mediation trying to settle it between one another keep it in the neighborhood okay Miracles why do we call the growth hormone sumatotropin i n because it's a protein or peptide related Trope or tropo means to grow something trophic okay and somato means Soma body oh it makes my body grow exactly remember the body of that neurone oh it was called the Soma yeah Soma is the body how about the middleman somato body Maiden intermediate look at the beautiful colors the red cells are the acidophils the blue cells are the basophils both of them are inside the anterior pituitary look at that here is my interior pituitary gland some of the cells are colorful called chromophils color loving cells others do not have any colors because they do not have any secretions and they are called chromophobes they shy from color back to chromophils they are larger they have granular cytoplasm because these are the secretory granules and they secrete their secretions that were stored in the secretory granules oh it makes sense acetophils appear pink we call them acetophils because they are acidophilic and they include the cell cells that make growth hormone if growth hormone is called somatotropin what do I name the cell that makes growth hormone somatotrophs okay how about the next cell that makes prolactin it's also an acetophil and we'll call it lactotrophs for lactation or mammotrophs because prolactin acts on the mammary glands it will grow the mammary glands and will help make and secrete the milk as for the remainder of the cells in the anterior pituitary they are the basophils and they include thyrotrophs for thyrotropin corticotrophs or corticotropin gonadotropes for gonadotropins let's grow your thyroid gland let's grow your cortex of your adrenal gland and let's talk to your gonads the story of growth hormone and the middleman hypothalamus will release growth hormone releasing peptide or releasing hormone which will go to the antipitibitory and will tell the pituitary to release growth hormone which will help you grow by means of its middleman going to the liver and telling the liver to secrete Sumer to meet and see also known as insulin-like growth factor number one because it acts like insulin from my previous endocrine videos you recall that we have two tails of hormones the lipid soluble and the water soluble the lipid soluble cannot Cruise in the blood because the blood is watery and the lipid is fatty so we have to carry it around on top of a plasma protein and since it is carried on the shoulder of the plasma protein it will take a long time before it reaches the cell membrane once it reaches the cell membrane however it can diffuse through the membrane it does not need any help from anyone else because your cell membrane is lipid by layer and this is a lipid hormone it will cruise through the membrane like a sharp knife in warm butter but it takes some time conversely if you are a water soluble hormone no need for plant asthma proteins because you are water and the plasma is water so you can swim in the water no problem and you will reach the cell surface very quickly however once you reach you will realize that you are watery but the cell membrane is fatty and water cannot diffuse in fat so you will wait until you find your receptor once you bind the receptor you will flip the switch on and boom the switch will talk to the nucleus by means of another middleman the second messenger system such as the G protein which we talked about before that's why I told you to watch the playlist in order growth hormone and prolactin have many similarities both are polypeptides I.
E water soluble okay that's why we say sumatotropin prolactin if it ends in in it's probably protein or protein related polypeptide peptide Etc both are secreted by acidophils from the anterior pituitary and these are the somatotrophs and the lacto tropes say respectively both hormones you will utilize not the D protein but the jackstad pathway and believe it or not both hormones are prolactation wait a second medicosis I get that prolactin is pro lactation but is growth hormone prolactation too yeah that's why some Farmers give growth hormone to dairy cows to secrete more milk oh that's why it's important to understand that both of them not only are structurally similar they are also anatomically similar and histologically similar and the cells are in close proximity to each other so it's not shocking to imagine the growth hormone sneaking and fooling the prolactin receptor and bind to the prolactin receptor to make more milk both growth hormone and prolactin will utilize the Jack stat pathway this is an example of non-receptor tyrosine kinase just like receptor types in kinase however it does not utilize tyrosine kinase we want to understand what tyrosine kinase is I have a specific video titled receptor Tyson kinase and another video titled non-receptor tausing kinase again the growth hormone and prolactin utilize the jagstat pathway however this Jack stat pathway is not peculiar to growth hormone and prolactin it's also utilized by hematopoietic cytokines and immunomodulating cytokines or chemical says how can I remember that all of these utilize Jack set pathway well think of a baby growing if I'm growing I need growth hormone if I'm growing I need breastfeeding if I'm growing I need to grow my red blood cells white blood cells and platelets oh and I need to fight infections this is the story of non-receptor tyrosine kinase again it had its own video but let's review it quickly here's the growth hormone binding the receptor the receptor is made of two parts as you see here a monomer and another monomer when growth hormone binds it flips the switch on which means jack is active by means of phosphorylation when Jack is active Jack will activate stat by means of phosphorylation when stat is active it will talk to the nucleus to do whatever you want hey growth hormone what do you want I want to grow what do you want I want protein anabolism we'll do that for you because I have the machine I have the DNA I have the RNA transcription translation protein synthesis I have everything I will make some proteins for you to help you grow what else do you want well I want to increase glucose in the blood I can help you with that I also want to raise free fatty acids in the blood we will help you that and this will be a story in Biochemistry growth hormone binding to the receptor when it binds the monomers become closer to each other and they dimerize they become a dimer instead of two separate monomers they combine together forming one dimer and then before you know a Jack is active when Jack is active it will activate stat by means of phosphorylation when stat is active it will go through the poor of the nucleus into the nucleus until your DNA hey it's time for transcription which means to make RNA and after transcription it's time for translation which is protein synthesis what kind of protein depending on what growth hormone wants for example Mrgrowth hormone wants to raise the glucose in the blood that's why growth hormone will favor glycogen lysis but it will not favor glycogen synthesis and remember in Biochemistry that glycogen lysis had many steps which had many enzymes each of these enzymes are proteins who made them the nucleus the nucleus made them to please growth hormone that's just beautiful remember before that you need to divide Endocrinology into two lands insulin land and everything else is in the anti-insulin land because insulin alone is anabolic how about the others catabolic what do you mean by the others the other team include glucagon epinephrine nor epinephrine thyroxine cortisol human placenta lactogen Etc and all of them are team catabolic hey insulin you're anabolic right what do you mean I am anabolic on proteins on glycogen and triglycerides so I am a builder I am anabolic I'll turn the amino acids from teeny tiny stuff into big proteins I am a builder I will convert the small glucose into big glycogen because I am a builder I will convert the small free fatty acids into big triglycerides because I am a builder however the others are glucagon cortisol epinephrine thyroxine and they are catabolic so protein will become amino acids and then the amino acids via gluconeogenesis can become glucose the glycogen is broken down into glucose the triglycerides are broken down into free fatty acids anytime you do this you will secrete Ketone bodies okay meticosis so I see insulin I see glucagon epinephrine thyroxine cortisol but where is growth hormone growth hormone is unique it's kind of weird it took one item from insulin which is protein anabolic and took two items from the other team glycogen catabolic and fat catabolic that's why growth hormone will help you grow muscles bones Etc by means of its middleman insulin-like growth factor because it's anabolic just like insulin the same growth hormone is also catabolic and glycogen it will help you break down glycogen into glucose raising the level of glucose in your blood hashed tag diabetogenic because I'm anti-insulin in this matter moreover growth hormone will also help you break fat oh by breaking the fat I increase free fatty acids in the blood releasing Ketone bodies in the process that's why growth hormone is ketogenic medicine makes so much sense if explained properly hey growth hormone it's time for you to rise and shine first of all let me tell you that I am somatotropin I am a polypeptide hormone I am secreted by somatotrophs these are acidophils of the anterior pituitary and when I get secreted I am secrete in a pulsatile fashion in order to be stimulatory to perform the functions that I want but if you infuse me to a patient continuously not in a pulsatile manner I will be an inhibitor of these functions not a stimulator pulsatile stimulates but continuous inhibits and I am secreted especially when you are sleeping near the early morning hours okay growth hormone what do you do well in some manner I am pro-insulin in other manners I am anti-insulin let's start by the pro insulin actions to be honest I deserve no credit as a growth hormone who deserves the credit then my middle man sumado Maiden C which is igf-1 which was released by the liver this famous igf-1 will help you grow proteins grow muscles grow chondrocytes which are cartridges and Bone and increase the size of tissue and organ a fact that will be extremely important when we study acromegaly you'll find that patients with acromegaly have a big heart big stomach big colon and this makes them vulnerable to polyps and colon cancer how about your anti-insulin actions well I am pro-glycogenolysis and gluconeogenesis so I raise glucose in the blood this is the opposite of insulin and that's why I'm anti-insulin I am diabetogenic while insulin is trying to fight diabetes moreover I break down the fat into free fatty acids releasing Ketone bodies in the process what are the Ketone bodies acetone acetoacetic acid beta hydroxy butyric acid these are acids and of course making Ketone bodies is the quintessential anti-insulin function because remember insulin is the major anti-ketogenic hormone in the body all the other team members including growth hormone are ketogenic Pro ketosis don't forget that my growth hormone itself Works via the jackstad pathway however its Metal Man sumatumidency works by mean of receptor tyrosine kinase and enzyme receptor substrate as the rtk and the IRS we'll talk about somatomidency in more detail in the next video let me tell you something any hormone that raises sugar and free fatty acids in the blood will help you cope with stress because it's providing you with sources of energy ready energy for your brain especially glucose that's why when a hormone raises glucose and free fatty acids in the blood it's called a stress hormone I. E anti-stress hormone I. E it helps you cope with stress growth hormone actions when I was young before the union of the epiphysis with the diaphysis when the cartilage was still growing and laying down bones growth hormone boasts intracartilaginous ossification which converts the cartilage cells into bone cells by means of igf-1 so igf-1 can come from the chondrocytes yeah so now we know that the liver cells make igf-1 also cartilage cells can make igf-1 to convert the cartilage into bones moreover when your young growth hormone increases the length and thickness of your bones that's why grow taller however after the union of epiphysis with the diaphysis you cannot grow taller you can only grow thicker this is gigantism this is acromegaly when you have too much growth hormone before the union and after the fusion respectively the effects of growth hormone on metabolism are pro-insulin in one Manner and anti-insulin in two manners pause and review with any hormone that we'll talk about in the series please try to remind yourself what are the actions of the hormone and how do we regulate the hormone if you can memorize this by practicing active recall it will help you tremendously regulation of growth hormone here are the factors that raise the growth hormone and these are the factors that suppress the growth hormone production number one factors that make GH go up include growth hormone releasing hormone from the big boss decrease glucose and free fatty acid think about it if you're starving and your glucose and free fatty acids are low this triggers growth hormone to go up to raise the glucose and free fatty acids in your blood so starvation is a factor that raises growth hormone sleep is a very important factor that increases growth hormone especially in the early hours of the morning stress big time why because growth hormone is an anti-stress hormone it helps you cope with stress by raising glucose and free fatty acid in the blood sex hormones estrogen can boost growth hormone because both of them want you to grow growth hormone wants to grow your muscles estrogen wants to grow something else growth hormone wants to build up proteins so if you eat amino acids especially Arginine this triggers growth hormone to work harder to build up those amino acids into big proteins in your muscle muscles in your bones Etc growth hormone is reduced by somatostatin the universal inhibitor which is also known as growth hormone inhibiting hormone also from the hypothalamus so now we know that somatostatin comes from the hypothalamus from the pancreas and from the upper part of small intestine here is a pathology link all of these three sites that I just mentioned can suffer from a sumetostatinoma the pancreas is a classic site increased glucose and free fatty acids in the blood growth hormone wants to raise them if they are already raised why the flip should growth hormone bother it should not old age everything deteriorates with old age and growth hormone is no exception that's why as you get older you're not growing you're the opposite you're senescent you're declining obesity decreases growth hormone obesity is not good for your muscles some hormones especially some Manchester and to a certain extent cortisol might inhibit growth hormone release and if you are abusing growth hormone surreptitiously from outside why do you think your body will bother making the natural growth hormone it won't starvation boosts growth hormone release especially protein depletion such as squash your core if it happens chronically if it's just acutely carbohydrate depletion also stimulates growth hormone release so in patients with quasher core who are protein depleted growth hormone is very high as a negative feedback as you feed them protein growth hormone will decrease back to normal here is the hormone here is the receptor this is physiology pathology can hit you here causing one disease or hit you here causing another disease this is the story of type 1 diabetes versus type 2 diabetes this is the story of central diabetes insipidus versus nephrogenic diabetes insipidus type 1 rickets versus type 2 rickets similarly if I have no igf-1 this is lacking this is called Levi dwarfism sometimes called Levi Loray dwarfism or short stature but what if the problem is not in the ligand what are the problem is in the receptor of growth hormone this is called larone dwarfism these two diseases have a genetic component for example a row is autosama recessive mostly seen in Ecuador but it's not the only cause of short stature it could be decreased igf-1 it could be decreased growth hormone from the interior pituitary or decrease growth hormone releasing hormone from the hypothalamus so why is the boy short it could be a problem in the hypothalamus a problem in the N2 pituitary a problem in the liver or a problem in the receptor regardless when this happens usually there is proportional decrease in Span and height what's my height it's from here to here from your vertex to your heel but what's the span well you need to make your arms like this left and right the span is the measure of the length from here to here in these patients there is decrease in height and decrease in Span proportionately so they look fine they are just short so when the growth hormone is low I am short but when the growth hormone is high I am tall if the growth hormone was high before the fusion of the epiphysis or I could grow thicker if the growth hormone increased after I grew up already which means after the fusion now there are some archaic terminologies in medicine the difference between pituitary dwarfism and pituitary infantilism dwarfism is just short but sexually fine maybe some delay in achieving puberty but once I achieve it I am absolutely fine I can have babies no problem whatsoever conversely pituitary infantilism is a problem in growth hormone so I am short and a problem in gonados opens so I have hypogonadism and usually cannot have babies short stature has many causes and Pediatrics that's a huge topic here I'll just give you four causes a growth hormone problem a growth hormone and gonadotropin problem a hypothyroidism congenitally and a chondroplasia in the first one I'm just short in the second one I am short and I cannot have babies in the third one I am short I cannot have babies and I have intellectual disability or low IQ it's the story of type 1 versus type 2.
pause and review all of that was hypo secretion of growth hormone now let's talk about hypersecretion if hypersecreation happen before the fusion of the epiphysis I'll get gigantism I'll be a giant but if it happened after the fusion of the epiphysis I'll grow thicker called acromegaly let's start with the giant gigantism overgrowth of all bones proportional increase in Span and height overgrowth of soft tissue so organomegaly muscle hypertrophy hyperglycemia because remember that growth hormone is diabetogenic it raises glucose in your blood and usually this is from a tumor in the pituitary secreting too much growth hormone but this tumor has other problems it's going to press on the surrounding healthy cells flattening them so what happens to the cells that secrete FSH and LH they are toast delayed puberty what happens to my thyroid troves they are toast I get decreased TSH which can affect my metabolism and brain development if this happens early enough decrease ACTH the cortical troves our toast so I get decrease of the stress hormone cortisol if the growth hormone increased happened after I already achieved my maximum height I'll get acromegaly I cannot grow taller but I can grow thicker very thick coarse facial features the jaw is extremely big it outgrows your teeth and that's why they will be increased spacing between your teeth a sign known as prognathism the jaw becomes very prominent facial features very thick and coarse the hands grow thicker the feet grow thicker my vertebrae can grow thicker causing kyphosis or a hunchback that's why the archaic terminology in medicine which is very inappropriate was ape-like face spade-like hands and Notre Dame like back of course you should never say any of this in front of patients I'm only men mentioning them because they can help you make a correct diagnosis just like the other horrendous mnemonic about the fat fertile febrile female in her 40s with 55 kids when we talked about cholecystitis extremely inappropriate but can help you save lives of course you know that we all need to treat patients with dignity what else happens in acromegaly organomegaly muscle hypertrophy in the beginning later atrophy because the outgrow their blood supply and the outgrow their nerve Supply obstructive sleep apnea why growth of soft tissue here making it more difficult for me to breathe big colon with many polyps that can increase the risk of cancer when the soft tissue in my wrist grow disproportionately it can impinge upon the median nerve causing carpal tunnel syndrome in my lower limbs tarsal tunnel syndrome too much growth hormone it's diabetogenic hyperglycemia this glucose is high in the blood eventually it will end up in the urine glucosauria glucose is osmotically active it will pull lots of water with it into the urine polyurea polydipsia as if I have diabetes don't forget that growth hormone and prolactin are similar they mimic each other I can get gynecomastia and this could be caused by an adenoma in my pituitary pressing on other structure if it presses on the gonadotropes thyroid tropes corticotropes it will lead to these symptoms if it presses on the optic chiasm it will give me bi-temporal hemianopiate how can I treat a disease caused by hypersecretion well you can either remove the tumor surgically or give medications to decrease growth hormone or at least decrease its binding to its receptor how can I decrease growth hormone release actriotide it's a somatostatin analog which is a universal inhibitor it in inhibits everything it inhibits growth hormone release but even after the growth hormone is released can you block its receptors yes Pig vasomant pegulated anti and somatotropin pig vasomant I am an antagonist to the receptor of the growth hormone a pituitary adenoma is a tumor in the pituitary that usually secretes lots of stuff could be lots of prolactin prolactinoma lots of growth hormone somatotropinoma lots of thyrotropin thyrotropinoma Etc this can lead to hypersecretion of one hormone and hypersecretion of the others due to pressure atrophy eventually if the tumor grows bigger and bigger and bigger and bigger it can destroy everything when the entire pituitary is toast it's called pan extended or inclusive hypo low pituitary function after mastering physiology it only makes sense to take care of pharmacology then download my endocrine pharmacology course at medicosisperfectsnetis. com it will teach you about the different types of insulin diabetic ketoacidosis and hyperosmolar hyperglycemic non-ketotic syndrome as for kidney physiology it's on my website too if you want to learn about many diseases check out my surgery high yield scores and emergency medicine high yield scores also downloadable at medicosisperfixnetis.
Related Videos
11:08
Insulin-like growth factor (IGF-1) - Somat...
Medicosis Perfectionalis
33,959 views
29:34
Prolactin - Prolactinoma - Hyperprolactine...
Medicosis Perfectionalis
16,725 views

17:39
Overview of the Endocrine System
Dr Matt & Dr Mike
1,985,553 views

41:08
Special Senses | Cochlea | Spiral Organ of...
Ninja Nerd
576,741 views

28:08
Hypothalamic Pituitary Hormones
Dr Matt & Dr Mike
20,352 views

6:57
How to Boost Your Growth Hormone with Slee...
Huberman Lab Clips
506,093 views

2:43:35
Body Language Expert: Stop Using This, It’...
The Diary Of A CEO
6,692,115 views

14:26
The Thyroid Gland - Thyroid Hormone (T3 & ...
Medicosis Perfectionalis
251,072 views

24:13
Endocrinology | Growth Hormone
Ninja Nerd
869,794 views

13:58
The Adrenal Cortex - Endocrine Glands - Bi...
Medicosis Perfectionalis
54,083 views
58:13
Hypothyroidism | Clinical Medicine
Ninja Nerd
140,706 views

26:12
How to Remember Everything You Read
Justin Sung
2,540,967 views

17:09
Growth Hormone 101: What it is, where it c...
Peter Attia MD
218,184 views

1:30:56
The Exercise Neuroscientist: NEW RESEARCH,...
The Diary Of A CEO
8,370,786 views
21:13
Insulin world vs. Glucagon world - A Tale ...
Medicosis Perfectionalis
50,020 views
5:56
Understanding Acromegaly
Zero To Finals
105,642 views
18:07
Pharmacology – DRUGS FOR PITUITARY AND THY...
Speed Pharmacology
256,642 views
25:30
Endocrine System Review - Pituitary, Thyro...
Medicosis Perfectionalis
43,078 views

49:16
Pituitary Disorders | Clinical Medicine
Ninja Nerd
57,258 views

21:44
The Endocrine Pancreas (Insulin, Glucagon ...
Medicosis Perfectionalis
37,625 views