CAR T Cells: Beating Cancer with the Immune System
48.32k views1933 WordsCopy TextShare
Medicurio
Doug Olson's terminal cancer was miraculously cured through genetic modification of his own immune c...
Video Transcript:
It’s 1996. The doctor has bad news for Doug Olson. He’s just been diagnosed with chronic lymphocytic leukemia, one of the most common types of blood cancer in adults.
Fast-forward to 2010 - his cancer is still not under control despite years of chemotherapy, and he’s running out of options. He decides to join a new clinical trial testing an experimental cancer treatment: genetically modifying a patient’s own immune cells so that they can kill cancer cells. Scientists called this “CAR T cell therapy”.
Miraculously, Doug’s cancer completely disappeared. This success led to further clinical trials, research, and the approval of the first CAR T cell therapy in 2017 as well as 5 more CAR T cell therapies targeting other blood cancers. In 2020, Doug’s blood was studied again, and scientists found that his modified immune cells were still patrolling his body, killing any cancer cells that appeared again.
His doctors said his cancer was essentially cured. Remarkable, isn’t it? Right now, many of the sickest cancer patients are getting invaluable extra years of life with CAR T cell therapy.
This video will explain how this treatment works and what the future holds for this revolutionary new therapy. CAR T cells are genetically modified versions of T cells, which are immune cells with a variety of functions, one of which being the ability to target and kill infected cells. To understand how CAR T cells work, we need to first understand how T cells get activated during an infection.
T cell activation must be a tightly controlled process because unnecessary activation of T cells without infection can lead to autoimmune disease and damage to healthy tissues. To prevent this, T cells must get two signals to become fully activated. This is going to get a bit technical with lots of different receptors, so bear with me – it will help explain how the CAR T cell works.
The first signal involves the T cell receptor, a fascinating structure that T cells use to detect pathogens. Specifically, they recognize chunks of a pathogen, which are called “antigens”, like part of a protein from a virus. These receptors slightly differ in structure between T cells, which allows different T cell receptors to bind to different antigens.
These antigens aren’t just floating around though – T cell receptors are picky because they only bind the antigen if they are held by a special receptor called an MHC molecule. The MHC molecule is on another cell, like a dendritic cell or another special antigen-presenting cell. The interaction between the T cell receptor recognizing its specific antigen on the MHC molecule is the first signal, which activates the T cell receptor signaling area called CD3ζ.
The second signal is called a costimulatory signal and acts like a confirmation, double-checking that the body is indeed under attack and the T cell should be activated. This second signal is usually activation of the signaling area of a receptor called CD28, but scientists have discovered many other co-stimulatory receptors, shown here. When both signals are received, only then can the T cell activate and multiply.
One type of T cell, called a killer T cell, will now look for infected cells to destroy. How does it know which cells are infected? It uses its T cell receptor and looks for cells that have the pathogen antigen on their MHC molecules, meaning there is pathogen inside the cell, and forces the infected cell to self-destruct, a process called apoptosis.
After the infection is cleared, memory T cells will lie dormant and become reactivated if the pathogen returns. You are now immune to that pathogen. The incredible ability of T cells to recognize a particular antigen, kill infected cells with that antigen, and create long-term immunity, made scientists wonder if we could take advantage of this feature to create T cells that can recognize cancer-specific antigens, kill cancer cells, and essentially, cure cancer.
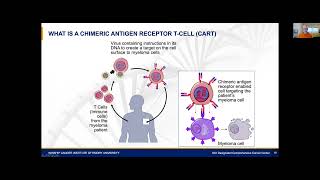
After decades of research, scientists made the idea of a modified cancer-killing T cell a reality: this is the CAR T cell. CAR is an abbreviation for "Chimeric Antigen Receptor". Much like the mythological Greek monster the Chimera, a combination of a lion, a goat, and a snake, the chimeric antigen receptor is also a combination of different receptors that allows the CAR T cell to recognize cancer proteins on the surface of cancer cells.
This interaction activates the CAR T cell to destroy cancer cells in a similar method of how killer T cells destroy infected cells. How does this work? This special receptor is made of three sections, or “domains”.
The first part is the binding domain, which is designed to bind and recognize the antigen of interest. The problem with a regular T cell receptor is that it only binds antigens if they are displayed on an MHC molecule. It cannot directly recognize a surface protein on a cancer cell.
To overcome this limitation, scientists decided to use special proteins from B cells called antibodies – specifically, the arms of the antibody, which can be designed to bind to almost any protein. By using one of those arms as the binding domain, the receptor can now recognize cancer surface proteins. When this receptor binds to the cancer protein, it needs to activate the T cell, so it needs a signaling domain.
Remember - a T cell needs both the T cell receptor signal and a second co-stimulatory signal to activate, so scientists have added the signaling domains from CD3ζ and CD28 to the end of the receptor. There’s currently ongoing research on which co-stimulatory molecule to use, with different combinations of co-stimulatory signals providing varying effectiveness in different cancer types. Lastly, to connect the two domains inside and outside the cell membrane, a transmembrane domain from another protein is used.
The segment connecting the binding and transmembrane domains is called a hinge or spacer, which allows the binding domain to be flexible when binding to the antigen, increasing its chances of successful binding. And with these three domains, we’ve got ourselves a chimeric antigen receptor that binds to cancer proteins and activates the CAR T cell. So how do we modify T cells to have these special receptors?
Since this entire receptor is a protein, we can take the different DNA sequences encoding the different parts, join them up, and deliver into T cells, usually by a disarmed virus. First, a special machine filters out white blood cells from patient blood, a process called leukapheresis. Then, in the laboratory, the T cells are isolated from the white blood cells, and genetically modified.
The modified T cells that express the receptor are selected and stimulated to proliferate into millions of cells, then transfused back into the patient to start eliminating cancer cells. This entire process takes around one month. As of 2023, there are six approved CAR T cell therapies for blood cancers.
Four of them target the protein CD19 to treat B cell leukemias and lymphomas, and the other two target BCMA to treat multiple myeloma. CD19 and BCMA are proteins also found on healthy B cells, so B cells are also destroyed during CAR T cell therapy and patients need careful monitoring and replenishing of antibodies after treatment. CAR T cell therapies are currently used only after other treatments have failed, and they still show remarkable success in these blood cancers.
For example, in a recent Phase III randomized clinical trial of 386 patients with relapsed or treatment resistant multiple myeloma, patients who received the CAR T cell therapy idecabtagene vicleucel had higher rates of patients responding to treatment, higher rates of complete cancer elimination, and a longer time being cancer free compared to current standard therapies. These impressive findings are encouraging scientists to test CAR T cell therapy as an initial treatment rather than a last resort, with promising results. We are also starting to realize that patients can be cancer free for years after CAR T cell therapy, like in Doug Olson’s case.
Scientists think that this happens when some CAR T cells turn into other T cell types or behave like memory T cells. They then patrol the body for cancer cells for many years after transfusion. This really is an incredible “living” drug!
However, this treatment isn’t without side effects. Aside from depleting B cells, activated CAR T cells can also activate other immune cells, resulting in the release of immune signaling molecules called cytokines. The widespread activation of CAR T cells and other immune cells results in cytokine release syndrome, which can range from a mild fever, which happens in most patients, all the way to organ failure, which is rare but life threatening.
The severity of this side effect is dependent on the amount of cancer originally in the body – more cancer cells will activate more CAR T cells, resulting in more cytokines released and a greater severity of cytokine release syndrome. Another rare side effect occurs when the cytokines also damage the blood-brain barrier and the brain itself, resulting in severe neurological symptoms. This is called immune effector cell-associated neurotoxicity syndrome.
These two severe side effects require careful monitoring and treatment with immune suppressants, but most patients are able to recover from this. What does the future hold for CAR T cell therapy? The most fascinating aspect of this therapy is really the potential of genetic bioengineering.
Here are some cool ideas being tested in the lab and in clinical trials. To make an even more specific CAR T cell receptor, the receptor could be modified to recognize two different proteins, and both need to be activated for killing. This is called a “Tandem” car.
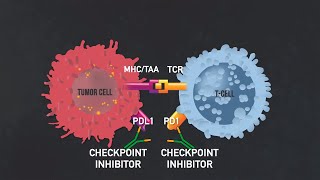
Research is also ongoing to design CAR T cells that work in solid tumors. Solid tumours are resistant to CAR T cell therapy because they can express molecules that activate off-switches on T cells. “Armored” CAR T cells are genetically modified to remove these off-switches, protecting CAR T cells from being disarmed, so they have a better chance of destroying solid tumors.
Conversely, “self-destruct” CAR T cells are genetically modified so they express an apoptosis protein that is only activated in response to a drug. The idea is, if side effects are out of control, a doctor can inject the self-destruct drug and the CAR T cells will die, stopping the side effects. Lastly, CAR T cells have to be made from a patient’s own T cells to prevent transplant rejection.
Right now, scientists are working on creating a “universal” CAR T cell that can be transfused into anyone and essentially used right off the shelf like other medications, which could dramatically reduce manufacturing time and the cost of this highly expensive therapy. These are just a sample of “power-ups” for CAR T cells, with many more being developed and researched, as well as other creative ideas such as using other types of immune cells or using CAR T cells to prevent autoimmune disease – more on this in the description below. While there are still challenges to overcome, including better management of side effects, lowering costs, and targeting more types of cancer like solid tumors, CAR T cell therapy represents a breakthrough in cancer therapy, offering hope to patients who previously had no treatment options left.
Continued research will improve this relatively new therapy into an even more effective tool in the fight against cancer. Thank you all for watching and supporting this channel. If you have requests for future video topics, I’d love to hear them!
Leave them in the comments below. And as always, see you next time on Medicurio.
Related Videos

18:33
CAR T-cell therapy: Reprogramming the immu...
TEDx Talks
172,377 views
15:17
Understanding the Immune System in One Video
Zero To Finals
1,464,565 views
1:01:59
Update on CAR T-Cell Therapy | LRF Webinars
Lymphoma Research Foundation
13,680 views

54:43
Killing cancer with a breakthrough therapy...
60 Minutes
4,295,121 views
20:34
Helper T cells | Immune system physiology ...
Khan Academy
1,377,352 views

13:46
MHC 1 vs. MHC 2, T-Cell Activation, T-Cell...
Dirty Medicine
17,746 views
8:32
Caffeine and Adenosine Receptors
Medicurio
386,772 views

11:18
CAR-T Cells: Engineered Cancer Killers
Peter MacCallum Cancer Centre
147,742 views
22:53
How does the immune system fight Cancer
Friendly Neighborhood Immunologist
21,700 views
1:02:39
Update on CAR T-Cell Therapy | Lymphoma Re...
Lymphoma Research Foundation
2,079 views
34:54
Tumor Immunoprofiling and the Tumor Microe...
BioLegend
15,729 views

1:37:34
The Cancer Expert: "This Common Food Is Ma...
The Diary Of A CEO
6,674,984 views
1:03:49
A 2023 Update on CAR-T Therapy in Myeloma ...
HealthTree Foundation
9,933 views

17:49
5 Foods That Help Fight Against Cancer & R...
Dr. William Li
770,169 views

1:07:15
Lecture 19 Immune System
Physiology for Students
167,534 views
10:48
How The Immune System ACTUALLY Works – IMMUNE
Kurzgesagt – In a Nutshell
23,676,471 views

59:12
CAR T-cell Therapy: The Good, The Bad and ...
BMT InfoNet
19,355 views
15:51
Introduction to Immunotherapy (Immunothera...
BioLegend
86,682 views
14:38
What Goes Wrong in Cancer? A Peter Mac bio...
Peter MacCallum Cancer Centre
26,968 views

30:38
In Vivo CAR T-Cell Therapeutics With Umoja...
Life Science Connect
770 views