Adrenergic Drugs Part 1 | Pharmacology | Dr Najeeb👨⚕️
158.6k views31062 WordsCopy TextShare
Dr. Najeeb Lectures
#drnajeeb #pharmacology #medicines #adrenergic #drugs # adrenergicdrugs
Adrenergic Drugs Part 1 | P...
Video Transcript:
foreign part of medical education that is about the autonomic nervous system and the drugs acting on the autonomic nervous system right when we talk about the pharmacology of autonomic nervous system we divide the drugs into two main groups drugs acting on parasympathetic nervous system and drugs acting on yes sympathetic nervous system right let's suppose autonomic nervous system pharmacology right primarily it is divided into two groups the drugs acting on drugs acting on sympathetic nervous system and of course drugs acting on parasympathetic nervous system now in early part of these lectures we will talk about the
drugs acting on sympathetic nervous system again the drugs which act on sympathetic nervous system are divided into two drugs which may make the action of sympathetic nervous system drugs which make mimic mean the drugs which produce actions similar to activation of sympathetic nervous system so those drugs which increase sympathetic activity in our body or those drugs which produce such effect in our body which is similar to the sympathetic activation those drugs are called sympathomimetic drugs sympatho my metric drugs some people also call these drugs adrenergic drugs foreign drugs or these are also called adrenergic Agonist
adrenergic Agonist so this group of drugs right sympathomemetic drugs or adrenergic drugs or adrenergic agonists drugs these are the this is the group of drug right which basically produces pharmacological actions which are very similar to activation of sympathetic nervous system right the second group here is the drugs which decrease the actions of sympathetic nervous system and the second group is called sympatho sympatho yes later drugs patholic drugs or they can be called anti adrenergic anti-adrenergic drugs or they can be called adrenergic antagonist drugs so we can say that basically all drugs which work on the
sympathetic nervous system they are primarily divided into two groups in pathometric drugs and sympatho lateral drugs sympathometric drugs are increasing the activity of sympathetic nervous system or they are producing the pharmacological actions which are like the stimulation of sympathetic nervous system right and sympatholic drugs are either decreasing the activity of sympathetic nervous system or they are producing pharmacological actions as if sympathetic nervous system activities blocked partially or completely is that right now to really really having a good concept of these drugs we must understand we must understand the neural physiology of sympathetic nervous system as
well as you must understand neurobiochemistry of sympathetic nervous system because primarily these drugs alter the neurophysiology and neurobiochemistry of the sympathetic nervous system so now I will talk about that how the sympathetic nervous system normally physiologically work once you have understood understood that very well that how the sympathetic nervous system can be activated what are the neuronal connection and sympathetic nervous system what are the neurotransmitters synthesized stored and released by sympathetic nervous system how those neurotransmitters work on the adrenergic receptors how that what are the different types of heteronergic receptors how those adrenergic receptors are
distributed differentially on different tissues in the body and how those sympathetic receptor brings physiological changes in the organ system first we will understand that then we'll go to the drugs now to really understand that how the sympathetic nervous system work as a component of autonomic nervous system let's go back to some of the neurophysiology we have a very good friend of us here come here please is Mr Gavin very soon he will be daktur Gavin right so this Dr Gavin will take as our example in which due to some sudden stress his sympathetic nervous system
is activated and we will see that once this sympathetic nervous system is activated what are the changes occurring in his different tissues is that right now uh first of all we will take an example that how is sympathetic nervous system can be certainly activated because all of you must be knowing already that's sympathetic system and parasympathetic system have most of their actions which are opposing to each other and sympathetic and parasympathetic nervous system are working automatically right they are most they are not under our will control right they automatically controlling some aspect of our visra
they are controlling our some of the metabolic functions and sympathetic nervous system activation actually prepares you appropriately to fight with the stress or flight or fly away from the stress again listen when you are under stress right I don't know this may be a physical stress someone is about to beat you or it may be some verbal stress or financial stress or academic stress but anyway if there is sudden increase in your stress level acute increase in your stress level sympathetic nervous system fires right and It prepares your body to fight or flight with the
stress the stress is small you're fighter if stress is too big you will fly away is that right and parasympathetic nervous system is dominantly working in your body when you are comfortable for example you are in your bed I mean in your own bed alone reading some novel which is not very stimulating right you have taken food very comfortable no stress stomach is full story is very good right there's no noise no threat financially you are not worried even your wife is not fighting with you I mean one of the unusual days you really feel
relaxed that is the movement your central nervous system is activating parasympathetic nervous system right but if sudden stress come Central over system will switch the balance it will reduce the activity in parasympathetic and increase the activity in sympathetic nervous system right so let us take example of this our friend Gavin that one what is your age 26 he can still afford more romance so one one very beautiful night moonlight he was feeling romantic feeling for another new lady but she was not available so he was alone moving on the road and thinking planning you know
men plan so many things right so he's planning and feeling good he's very confident he will do so many things sooner or later right and feeling great suddenly a very big suddenly a very big very black dog appears and dog is barking in a very hostile manner and when he looks to the dog he finds that size of the dog is progressively increasing now you understand the central number system will appreciate the stress and sympathetic system will start firing and there will be physiological changes in his body right and if dog is really big in
Black and very hostile of course the sympathetic nervous system will be activated and he will decide to run run away run not two words away right but if unfortunately dog is very small and not very hostile just irritating him maybe he attacked the dog you never know human nature he attacks the dog and dogs sympathetic nervous system is activated yeah you never know this is life you see so okay in our example we take a dog which is really big and black and after him and his sympathetic nervous system is activated and he decides to
run away right and we'll see what goes in his central nervous system and peripheral nervous system and neuronal sympathetic nervous system activity you have a seat and we deal with your central number system right actually how is sympathetic nervous system will be activated the real activity will initially start in central nervous system let's suppose here it is Central yeah nervous system you understand of course cerebral Hemisphere and midbrain ponds medulla spinal cord and cerebellum now the main Center the main Center for regulating the activity of the sympathetic and parasympathetic functions is present in the hypothalamus
now hypothalamus is located here you know here is your interior pituitary posterior pituitary now here is your hypo th thalamus right the neurons in the hypothalamus are mainly determining that well autonomic nervous system should be more having parasympathetic activity or sympathetic activity right now within the hypothalamus there is ventromedial area and you can say interior area and there is posterior area now Ostro lateral area actually if I draw the hypothalamus here now this intermedial area of hypothalamus if this area is stimulated you will have activation in parasympathetic nervous system but if this post row lateral
area in the hypothalamus is stimulated the neurons in this area you will have increased sympathetic nervous system activity is that right so basically hypothalamus is the highest Center in the center of a system which is controlling the balance between the sympathetic and parasympathetic activity is that right now of course when big black dog is after him then this part of hypothalamus should be activated so the end anterior part of hypothalamus should be having reduced activity and postol lateral sympathetic areas in hypothalamus should be having increased activity so that sympathetic fibers should be stimulated but the
thing is that how the hypothalamus know that there is stress how hypothalamus knows that there is stress and how hypothalamus knows that now I should increase the sympathetic activity actually in our central nervous system this large area which is concerned with emotions emotions and behavior and memory this area I'm showing in this diagram as limbic system in the central nervous system there are multiple areas which are together as a group called limbic system the function of the limbic system is concerned with emotions with your behavior with your recent memory and many other functions so now
when a big black dog is coming after him and dog is barking in a hostile fashion so the the barking sound through his ears through his auditory Pathways will go to the auditory contacts auditory cortexes in the temporal area so barking sound activate the auditory areas in the temporal cortex and that will give special stimulation to the limbic system then if he turns his neck and look at the dog through Visual pathway image of the dog is on the what is this occipital cortex visual cortex this will also give information that visual information is very
very hostile to the limbic system then maybe he is having some past experiences with the dogs unpleasant past experiences with the dog or maybe he has seen some movies and with dogs are really very hostile right or he has seen someone suffering with their dog bite so that memories from other part of cerebral cortex will be also activated and stimulate the limbic system so now what really happens that limbic cortex or we can say emotional cortex is collecting the information about the recent events right and when limbicortex appreciate that ordinary information is stressful visual information
is stressful and the new information which is coming that is related with past information which is also stressful then those neurons will be activated those neurons will be activated in limbic system which will stimulate yeah which will increase the activity in posterior part of hypothalamus and same neurons at the same time will inhibit the activity on the yes parasympathetic nervous system so the balance will be altered in the hypothalamic activity so what really happens whenever you are under stress from cerebral cortex information is going of course to the limbic system and when limbic system undergoes
stress right it will activate the sympathetic components and inhibit the parasympathetic component present in hypothalamus once sympathetic centers and hypothalamus are activated from there the descending Pathways will be there right multiple neurons right chain of multiple neurons we call it polyneuronal descending Pathways the descending Pathways which are made of multiple neurons so these polyneuronal descending Pathways will be activated and these Pathways will come into lower part of central nervous system and they will activate sympathetic outflow they will activate yes please sympathetic outflow so what really happened when he went under stress is cerebral cortex activated
the sympathetic centers and hypothalamus which activated the polyneuronal descending sympathetic pathway which will control the sympathetic outflow now sympathetic outflow comes out of central nervous system from spinal cord and which part of the spinal cord from thoracic part of the spinal cord and from the lumbar part of spinal cord so we can divide the spinal cord into okay this is cervical spinal cord this is suppose thoracic spinal cord and this is lumbar and this is sacral cervical fluoresic lumbar sacral so what really happens that from here the neurons will bring the information out right now
these neurons which are bringing the information out they are present from T1 up to number L2 or 3 right and these neurons and bringing the information out I will just show one pathway large and they end up into some sort of sympathetic ganglion this is sympathetic ganglion so this neuron which is present in the spinal cord you know where exactly it is present in spinal cord let me draw the section of spinal cord in the spinal cord these outgoing neurons have the cell bodies in this area and in this area this is interior harm this
is posterior horn and this is called intermediate heart or lateral heart so neurons which are coming from the top they will stimulate the neurons in the lateral horn or intermediate heart from here sympathetic outflow will go out and go to the ganglion is that right from the ganglion post-anglionic neurons will be going to the tissues now let's come back and talk about that there is lot of sympathetic outflow coming from all these areas right now one thing we should you should appreciate that sympathetic outflow is diffuse diffuse means that multiple areas will be activated because
thoracolumbar all the outflow is activated simultaneously it is not possible that Central of a system activate only fibers going from thoracic segment six and not stimulate fiber from four and five so it's a diffuse outflow is that right now how this outflow really work I will take two examples only number one suppose from this neuron fibers are going out and these fibers go to yes this is a nerve ending right this is the cell body of the neuron axon of the neuron and nerve terminal this terminal is present in a sympathetic ganglion right from the
sympathetic ganglion what really happens that post ganglionic fibers will go and they will eventually terminate on the yes on the tissue they will terminate on the tissue let's suppose this is hard so then these fibers post ganglione fibers will release neurotransmitter on the target tissue and Target tissue will have receptors here to make a very good concept we have to understand that once sympathetic descending pathways are activated and preganglionic neurons fire right most of the pre-alienic neurons are ending up into sympathetic ganglion and pathetic ganglion right are stimulated and poor skinlenic fibers will eventually end
up into Target tissue right and at the Target to show the main neurotransmitter which is released here is yes nor epinephrine but so post ganglionic fiber release norepinephrine at neuro effector tissue or at the neuro effector site but remember these sympathetic premium learning fibers they release a different neurotransmitter which neurotransmitter is released from here yes sympathetically any fibers release acetylcholine so you have to remember that nor epinephrine is released by the post ganglionic nerve ending foreign a very important thing all the neurons which come out of central nervous system are called energetic no need to
memorize the basic principle almost all the neurons which come out of central nervous system are call energetic you must be knowing that there are sympathetic preganglion coming out cholinergic parasympathetic preganglione coming out call Energy even motor neurons going to the skeletal muscle and neuromuscular Junctions they are also cholinergic so all the neurons which come out of center of the system are cholinergic so of course please in the annual sympathetic fibers are also cholinergic and here they act on cholinergic receptors right and these are nicotinical energy receptor called Energy receptors are two type nicotinic type and
muscarinic type nicotinic type then action potential is produced over here and when the suction potential arrives at neuromuscular or sorry at the neuro effector Junction this nerve terminal release is not epinephrine in this way sympathetic nervous system releases not epinephrine on the target tissue through their innervation through the nerve Supply but sympathetic nervous system has one more way to work that some of the pre-ganglionic fibers they don't go to the ganglion they go to the Adrenal medulla the sympathetic ganglion are ending up these fibers some of the what are these fibers sympathetic fibers they end
up on adrenal medulla right suppose this is Adrenal medulla and here it is adrenal gland cortex and these fibers release Here Again acetylcholine which act on the what is this Adrenal medulla cells and stimulate the Adrenal medulla cells and Adrenal medulla Cell release Adrenal medulla cells release epinephrine mainly not not norepinephrine about 80 to 90 percent it releases happy nephrine in General circulation remember sympathetic nerve endings are mainly releasing norepinephrine nerve ending n e nerve ending releases nor epinephrine and e but Adrenal medulla releases epinephrine now of course actually what is the Adrenal medulla they
say during the evolution many ganglion cells come together and lose their exons and the start releasing their neurotransmitter into blood and that is how adrenal Metalized made phylogenetically now Adrenal medulla releases epinephrine in the general circulation of course on Center on sympathetic nervous system stimulation but this epinephrine will circulate in the blood and go to stimulate adrenergic receptor wherever they are present in the body it means that let's suppose their adrenergic receptors present over here now these aerological receptor can be stimulated by the non-epinephrine coming from the sympathetic nerve ending or these adenosine receptors can
be stimulated by epinephrine which is present in general circulation so what we learned up to now we learned up to now the sympathetic nervous system releases norepinephrine through the nerve endings and it releases epinephrine into from adrenal medal line to General circulation so receptors at neuro effector sites release norepinephrine through innervation or they receive epinephrine through the general circulation am I clear to everyone there is no problem up to this now we have to come one more thing that how this nerve ending work how this neural Factor site work right how this area is functioning
but before we discuss that I will talk about The receptors right that how these receptors are present in the body once epinephrine or norepinephrine come to the adrenergic receptors receptors are stimulated and what changes come into body right after discussing that we'll come back to this specialized area this is a very very specialized area because there are about 30 drugs which work only on this nerve ending and it's neural Factor side okay I'll leave it up to you so Gavin dog is after you so you must tell me that we should discuss this area first
how this small area work I will make a big diagram explain it thoroughly right because there's so many drugs which work in this area should I explain this first or I should explain this later and just tell when epinephrine and norepinephrine is going into your blood how changes are occurring in your body so that you can fly away from the dog first you want to know this thing yes okay he want to know first this thing what's going on here right but meanwhile dog may catch you okay now let's come here let's suppose this is
right here is the cell body of post galionic neuron is that right and this is posting ionic neuron exam going on now of course this axon should must end up into tissue what I'm going to do I'm going to make the nerve ending out of proportion very large you understand it this is one of the nerve ending of sympathetic neuron and here is suppose Target tissue target cells these are Target cells on which neurotransmitter well work right so let's start discussing this area which is pharmacologically extremely important that what's going on in the nerve ending
what is going on in the synapse what's going on in this area and how drugs alter the activity here right first we will understand how the neurotransmitter is synthesized stored and released of course all of you know the main neurotransmitter at this point is norepinephrine my question goes to someone very intelligent that norepinephrine which is present here in the synaptic vesicle that norepinephrine is synthesized my question is that normal is synthesized in the cell body of the neuron and then transported here are that norepinephrine is synthesized locally in the sympathetic nerve ending question goes to
this gentleman you think norepinephrine is stored here and synthesized here it is not synthesized in the cell body okay you think it is here anyone who differs what do you think man here that's right actually most this is a basic principle most of the small molecular weight small molecular weight neurotransmitters are synthesized within the nerve and then is that right most so norepinephrine is a small molecular weight neurotransmitter so we will see how it is synthesized here let's suppose start with very basic from the git of course you take lot of amino acids right proteins
you eat a minor assets are coming here from the git minor acids are absorbed into yes please General circulation and then these minor assets are distributed to all tissues in the body am I right one of the Amina assert which is absorbed from the git that is tyrosine thank you scene is one of the amino acid now what really happens that sympathetic nerve endings are specialized in concentrating tyrosine they take there are special pumps here there's special tyrosine uptake mechanisms here in this nerve ending and what these are doing these pumps that they take extracellular
tyrosine molecule right and pump it n so in this way all sympathetic nerve endings are very rich in tyrosine once they have taken the tyrosine then an enzyme will work on it I always think tyrosine is like Tire you know Tire in the car circular so tyrosine is also circular what I mean by circular let me draw the molecular structure of tyrosine it's not difficult again it's circular remember in Pharmacology you are not supposed to memorize and remember the molecular structures of the drug except sympathetic nervous system because in the drugs of sympathetic nervous system
there's a very big correlation between the molecular structure and function of the drug when you little change the molecular structure function of the drug changes due to that reason only in sympathetic nervous system especially adrenergic drugs you must know some idea about their structure because they function depend on that but remaining pharmacology you are not supposed to remember molecular structures now tyrosine structure tyrosine is like a tire it's a Benzene ring one hydroxylation here right what is this ch2 ch2 right what is there the methyl ethyl group here and then with that there is a
minor group here and there is carboxylation now this is basically tyrosine fundamental structure so what really happens tyrosine is pumped into nerve ending right in the nerve ending there is the enzyme the first enzyme which will work on the tyrosine what is the name of this enzyme who is going to tell me the name of this enzyme tyrosine hydroxylase that is called yes tyrosine hydroxylase so tyrosine hydroxylase work on this molecule listen keep this basic molecule in your mind this is the mother compound or I don't know father compound of the sympathetic neurotransmitters and Drug
all the basic compounds most of them are derived from this structure now first you do hydroxylation of the tyrosine so when you do the hydroxylation what really happens here a hydroxyl group is added what is added over here hydroxylation is done and hydroxyl group is added over there is one question you know epinephrine norepinephrine and dopamine and isoprenaline or isoprotelinol all of these drugs are called catecholamine also have you heard of it epinephrine or epinephrine dopamine isoproterinol all of them are also called means why we call them catecholamine question goes to that lady okay if
you want to know the answer she doesn't want to know the question anyone can answer because these again again and again when you read the books you know my duty is to make books easy for you you enjoy the books so many books they mentioned epinephrine or not epinephrine or dopamine or isoprotelinol they are catecholamines so who is going to impress me by telling why they are called catecholamines yeah you want to impress me no no I want to know why they are called catecholamines of course they have catechol ring what is catacall ring I've
given you idea please impress me category what is catacol ring listen any Benzene ring with three and four hydroxylation is called catecholine that's it yeah now you are impressing me after the time you say of course catacol has a mind group also so basically catacola means are the compound which have amino group and catechol ring what is catacol ring catechol ranges yes dihydroxy Benzene ring where one hydroxyl is at three position and four position am I right later on we will see in the lectures of drugs the how you change the height oscillations and drugs
actions change right so that is why because epinephrine norepinephrine dopamine and isoprotylinol all of them have this ring structure so they are called catechol compounds and in the end they have a minor growth so catacola means is that right but whenever we remove these category this hydroxylations we say drugs are non-catecholamines in Pharmacology we say is so you have to remember whenever we say drug is I think it's ears are removed these are the oscillations are removed anyway so tyrosine gets hydroxylated here and once it is hydroxylated the new compound is called dopa now this
compound which is hydroxylated this is called dopa this hydroxylated compound right and once dopa is produced right then what really happens in the next step is guess now next enzyme will come into action and convert the dew point to yes please dopa mean now how the dopa can be converted into dopamine it's very easy brinda what is this carbon dioxide out so when this molecule will puff out carbon dioxide it will puff out carbon dioxide it will become dopamine so the next enzyme we should be working here should be dopa decarboxylase working on the dopa
yes and removing what carboxyl group so dopa d car boxy Liz so this dopa decarboxylase right it worked on the dopa and what comes out remove the carboxyl group or carbon dioxide so look here we have lost this carboxyl group right we can make it like this it is lost carbon dioxide like a balloon of a baby it is going away and who has done this function dopa decarboxylase and now what is the structure present over there dopamine right so you take a tyrosine and hydroxylase you get dopa you take the enzyme dopa decarboxylase do
the decarboxylation of dopa and you end up with yes what is this dopamine right now as soon as dopamine is produced there is a problem if it is a if it remains here in the cytosol it will be immediately destroyed you know why it will be destroyed who knows because it will be immediately destroyed and prevent the destruction of this molecule we should pump this molecule into a membrane-bound vesicle there's a membrane bound vesicle over here right and there are special vesicular transport system and this vesicular transport system should take the dopamine and pump into
vesicle the question is that once dopamine is synthesized it is immediately pumped into what neuronal vesicles why because it will be destroyed outside who will destroy it there's a cat there cat cat let me tell you there are mitochondria here you know mitochondria's what is the relationship of mitochondria here with this discussion on the surface of mitochondria there is a very very dangerous enzyme right it is just like a cat I feel this is expressed on the surface of mitochondria and this enzyme is called oxidase this enzyme can do oxidation of mono amines now what
is monoamine yes given don't forget about the dog just yeah what is monoamines yes Ronald compounds which are neurotransmitters which are derivative of single amino acid they are mono amines right from single amino acid now what are monoamines dopamine is monoamine it is derived from tyrosine norepinephrine is monoamine because norepinephrine is derivative of dopamine epinephrine is monoamine because epinephrine is derivative of norepinephrine tyrosine make many monoamines one of my mono mind from tyrosine is dopamine other mono mind from the tyrosine is yes norepinephrine another mono mind from tyrosine is epinephrine is that right then from
another a minus a tryptophan we can make five hydroxytryptamine solutanin so tryptophan is amino acid from where we can derive slowdown in so slow down in is also monoamine is that right am I clear even neurotransmitter histidine is monoamine the derivative of histamine and what about acetylcholine yes it is not mono mind it's not derived from any amino acid right so you know what a monoamines so in many of the nerve endings in central nervous system or peripheral nervous system there is mono mine oxidase on the mitochondrion and this monomite oxidases can do catabolism of
epinephrine or epinephrine dopamine so you must know they are involved in multiple metabolic destructions of multiple neurotransmitters anyway let's come back actually if dopamine remains here attention plays dopamine epinephrine norepinephrine all of them can be destroyed by so as soon as dopamine is synthesized it is captured into vesicle so that it is not destroyed by monomial oxidase am I clear so dopamine is taken in now listen carefully if this nerve neuron is dopaminergic if it was dopaminergic there will be no further reaction dopamine will be stored and released but our neuron is not dopaminergic it
is foreign this neuron is adrenergic neuron so it means still one more work need to be done conversion of dopamine into friend so within with the wall of this membrane there is a very special enzyme here right now this enzyme is attached in the internal wall of the internal side of the vesicular membrane right what the sunshine is doing who is going to tell me it is going to do work on the dopamine one more action what is that action dopamine beta hydroxylation there will be one more hydroxylation done by this right by this enzyme
and this point this is a beta carbon so at this carbon it will add what hydroxylation and when this point gets hydroxylation now the compound is called yes please this compound is called norepinephrine so what really happens that dopant mean is acted upon by this drug Sorry by this enzyme the name of the enzyme is dopamine beta hydroxylase in some work they call it dopamine beta oxidase it's same thing but anyway majority of the authors they write it dopamine beta hydroxylase so those neurons which release norepinephrine in their vesicle this enzyme is present but those
neurons which release dopamine they don't have this enzyme am I right claro now we have converted dopamine into yes please Nar epinephrine in this way these vesicles keep on concentrating the dopamine and converting into norepinephrine and norepinephrine molecules keep on accumulating then what will happen what will happen if norepinephrine molecule keep on accumulating the osmotic power osmotic pressure in the vesicle will become very high it may automatically burst and we don't want that so this norepinephrine is complexed with some proteins inside called chromogranin or with ATP and some ascorbic acid so what happens this norepinephrine
is complexed with some internal proteins and ATP so norepinephrine molecules will be binding with them and you know osmotic pressure is directly proportional to the number of molecules not to the size of the molecule so when they are kept together like a group osmotically they act not as one two three four five they don't act as six molecules osmetically as a group they attach one molecule is stored over here right then when stimulation will come you remember that stress was appreciated here sympathetic poly neuronal descending Pathways were activated and then sympathetic outflow was activated and
then eventually these nerve endings should be activated and it should release the norepinephrine now we have to talk about how the norepinephrine is released of course it is released when action potential comes over here you know when this neurons is stimulated wave of depolarization followed by the wave of repolarization will reach here how the depolarization of this nerve ending will lead to the release of norepinephrine yes please you know when depolarization will come what it will say please go out physical excellent actually there are depolarization sensitive calcium channels present in this nerve ending this now
bending has yes please depolarization sensitive calcium channels so when depolarization is sweeping coming here deep under the voltage gated sodium channels will be opened right sodium will depolarize the influx of sodium will depolarize the membrane and when membrane intercourse depolarization the depolarization sensitive calcium channels open and when these calcium channels open a lot of calcium comes in very good so what this calcium will do my friend was telling what this calcium will do very good that incoming calcium will help the vesicle to few vesicular membrane to fuse with nerve endings membrane and both membranes should
fuse and release the content but exactly how this Fusion occur let me tell you actually on this membrane there are special type of proteins attached and these proteins which are attached here these are called synapto Braven synapto bravin and there are complementary proteins which are present over here right and these are called syntax sins so you just like actin and myosin they can as actin and myosin can interact in the same way some proteins on vesicular membrane and some other proteins on the neuronal membrane they are having a capability to interact with each other but
what really happens that syntaxin is an off State it is like this and it cannot fit but as soon as calcium comes in look here as soon as calcium come in calcium will bind here and here and both calcium will repel each other you know and this pocket will open so this will be wide open to welcome this thing just think this and after Brave in right here and here then sign up to prevent and this will interact with each other and that will lead to the fusion of this membrane vesicular membrane with the what
is this funny thing neuronal membrane right and in this way this membrane okay I'll make it thick I'll make a different color membrane this is what vesicular membrane right so this vesicular membrane will fuse with the what is this cell membrane and you know what will happen norepinephrine will be regurgitated out you call this process exocytosis right norepinephrine is released for its section right but this membrane is very specialized membrane you remember this membrane was having special transporters this membrane had special type of enzymes attached with it am I right right and many other Transporters
so as soon as this membrane of vesicle fuses with this it releases norepinephrine and you know what happens after that then this membrane when this after that this membrane will be taken back you know how it will be taken back from inside of the cell special type of proteins will bind here these proteins are called clathrines what are these right clactines will bind with this membrane and pull it back so empty vesicle will come back so that this vesicle can be used again this is very important piece piece of patch of membrane you should go
of fuse release its content and recapture back into nerve ending to be reused again of course when it comes back it is empty am I clear there's no problem here now once the norepinephrine release what it is doing there it is going to act on presynaptic membrane as well as post synaptic membrane on The receptors right now when it act on post synaptic membrane maybe this tissue has let's suppose this tissue has receptors and this receptor is adrenergic receptor now adrenergic receptors are classified as Alpha receptors and beta receptors Alpha receptors are primarily Alpha One
and Alpha 2 and beta 1 are primarily beta 1 beta 2 and a modified beta 1 which is also called beta 3 right we will discuss receptors in detail later now what really happens that most of alpha 1 beta 1 and beta 2 they are present post synaptically they're present on the tissue so let's suppose this Alpha One receptor present over here remember all the adrenergic receptors are 7 pass receptors coupled with intracellular G proteins this is Alpha One adrenergic receptor coupled with g Cube we'll discuss that later then maybe Target tissue have a different
type of hydrologic receptor and this is not Alpha One this is suppose beta 1 adrenergic receptor right and this beta monitor energy receptor is coupled usually with g s g stimulatory protein some other tissue may have yes beta 2 adrenergic receptor which are also coupled with G stimulatory and here it is beta2 adrenergic receptor and as here is Alpha 1 Alpha 2 receptors are present mostly at pre-synaptic membrane of the this is Alpha 2 adrenergic receptor which is present on presynaptic membrane so when norepinephrine is released this norepinephrine will work on yes depending upon what
receptors are present over there it may work on Alpha 2 receptors which are presynaptically present it may work on Alpha One hydrological receptors uh beta 1 hydrologic receptors are beta2 adrenergic receptors and while acting at these places it will produce its actions when these receptors are stimulated right it will produce its action what will be the action of these receptors I will discuss later right Alpha One receptors are on different tissues and they produce different action as compared to the suppose beta1 receptor but about Alpha 2 receptor I want to discuss right now whenever sympathetic
nerve endings release not epinephrine a small component of norepinephrine work on presynaptic membrane on Alpha 2 receptors these Alpha 2 receptors are coupled with g inhibitory protein and G inhibitory protein will lead to reduced cyclic amp level not going into detail but some of you may be knowing that when Gene inhibitory protein is stimulated when G inhibitory protein is stimulated it inhibits the yes adenylal cyclase and when adrenaline cyclist is inhibited that will lead to reduced production of cyclic amp right so there will be reduced production of cyclic amp plus G inhibitory protein also open
the potassium channels it opens potassium channels and intracellular potassium start moving out so what will happen when epinephrine or norepinephrine work on Alpha 2 receptors right then there is reduced cyclic empty levels and there is increased loss of potassium when cell is losing potassium it is losing positive charges it become electrically very negative so when it becomes very negative electrically it becomes hyperpolarized membrane becomes more polarized to the negative side when it becomes hyperpolarized then what happened it becomes difficult to stimulate this membrane so when it becomes difficult to stimulate further electrical stimulation of membrane
become difficult when membrane is losing too much potassium is that right it becomes too much electrically negative it becomes difficult to depolarize this is the right when it becomes difficult to depolarize so electrical is this nerve ending become inhibited and further release of norepinephrine is reduced so it means this mechanism is auto inhibitory secondly reduce cyclic amp will lead to reduced activity of protein kinase a and when activity of protein kinase is reduced right that will lead to reduced activity of these enzymes so even synthesis of neurotransmitter is reduced so what really happens that this
is an what is this this receptor act as autoinhibitory molecule that as more and more norepinephrine is released norepinephrine stimulate Alpha 2 receptors and they give inhibitory signals by losing the potassium and by by reducing the intracellular cyclic amp there's no ending become inhibited and further release of norepinephrine is reduced in this way this is an auto inhibitory lobe is there any question here then let's talk about we I will discuss this later that what are the actions on Alpha One receptors beta 1 and beta 2. once norepinephrine is done pre-synaptic and postsynaptic actions what
happens to norepinephrine it keeps on staying there or what happens to norepinephrine question goes to yes ma'am what happens to this norepinephrine yes sir yeah it is degraded okay uh my friend is telling that acetylcholine oh no my God why I still calling a talk I should say norepinephrine which is released my friend is saying it is degraded what is the enzyme which destroys it here I tell you whatever will be your answer it will be absolutely wrong because it is not degraded here but what is your answer okay listen listen carefully this this is
a major difference in adrenergic and cholinergic system when a style colon is released there is a style choline nestres there in the synaptic area and acetylcholinesterase destroys the style choline so termination of action of style choline is by destruction of acetylcholine but nor adrenergic system does not have any big amount of any enzyme to destroy norepinephrine or epinephrine or dopamine at this side right so norepinephrine is not destroyed here right what we do with it primarily it is like a ball you know ball you throw a ball it touched the air with elastics you pull
back then you again throw and pull it back you reuse this again and again it's very valuable tiny molecule you don't want to destroy it then there'll be too much energy you know you keep on getting angry for small things you're releasing nor have been a friend and then if all the norepinephrine is destroyed then you cannot afford to be angry again is that right but actually you can be angry with your why if them with your own self with your child maybe with your studies or may be angry with some fly or mosquito depends
on your personality right so why you can become angry irritated again and again you can afford so many episodes of stress in a day because more epinephrine which is released 80 of that is recaptured restored to be used again is that right so actually once it has done its action there there it bounces back and here is someone waiting for it to pull it back and there's a very special transporter here there's no need to remember that it is 7 12 pass molecule just remember there's special reuptake mechanism here this special reuptake mechanism is called
reuptake one mechanism this is also mono mine uptake system what really it does that nor epinephrine which was released here and doing its action very rapidly most of it this not epinephrine well the reuptaken by the system and it is back happily right but you know life is not that good even for the molecules who is waiting here wow so it depends on luck sheer luck that some of these molecules before they are attacked by the mouth these molecules are reuptaken back and they become really very very happy they are back to but some of
these molecules which are reuptaken if they are not rapidly Enough recaptured by the vesicle they will be treated by the small one when they will come out of Mao they are degraded they are lost right they are going into catabolic pathway am I clear so what really happens that major pathway by which adrenergic activities terminated right that is by the norepinephrine reuptake but you have to remember this is not only not epinephrine reuptake even dopaminergic neuron also recapture most of the dopamine even neurons recapture most of the serotonin why I'm stressing so much this pathway
because the many drugs which work at this point stop it we'll talk about this in the next section just after a few minutes right so this is reuptake one this is re uptake one mechanism but some of this may be some of it may be attacked by another enzyme present on postsynaptic membrane and that enzyme is not Mao there may be another enzyme here right okay what this enzyme is going to do you know what this enzyme is going to do is that it will take norepinephrine and when not epinephrine will come out it has
lost it one component you'll tell me which component is lost from this molecule yes guess it yeah I'm making the molecule and you tell me which component is lost should I yes please I have completed the molecule and you did not tell me which component is the last this hydroxyl is lost this enzyme has eaten up that hydroxyl point right not only not sorry sorry not only hydroxyl is lost rather it has added methyl group here right methyl group you know what is the advantage of adding methyl group when you do methylation of a molecule
molecule become less polar and more yes it becomes less polar is that right so hydroxyl is lost and methyl group is added what is the name of this enzyme actually just let me tell you this enzyme is in present in very high concentration in liver also this is one of the very important enzyme to destroy the catecholamines there are two enzymes which you are supposed to know for destruction of catecholamine one enzyme is monoamine oxidase and other is catacol O methyl transferase have you heard of its comt c o m t it has attacked the
catacol rain and transferred a methyl group there so it is called o methyl transferase is that right so what really happens how the action of norepinephrine is terminated most of it is recaptured and whatever is recaptured most of it is restored in the vesicle a small component may be destroyed by monoamine oxidase present in the nerve ending on mitochondrion and a part of it may be destroyed by category o methyl transferase attached with the cosine on the effector tissue and part of it may diffuse into General yes part of it may diffuse into very small
component May diffuse into General circulation and this epinephrine and norepinephrine which has gone into General circulation eventually it will be catabolized by liver or by kidney both of these tissues are very rich in monoamine oxidase and catechol O methyl transferase right this is a very basic biochemistry related with this system we'll have a break and after the break we will discuss that at every step which drugs are working and how they alter the synthesis storage release and action of adrenergic neurotransmitter right let's have a break now we have discussed in detail the structure and function
at neuro effector site of adrenergic system right now this area where adrenergic nerve ending are acting at the factor side right this area or this operators is Target for many many sympathomemetic and sympatholic drugs many drugs either increase the activity in this area or decrease the activity in this area so let's see how the drugs work in this area and start step by step first of all we'll talk about the drugs which work earliest step the drug which work at the earliest step is methyl tyrosine methyl Tyro sin methyl tyrosine mean that methyl group is
there with pyro sane right now this methyl tyrosine this is a drug what this drug will do it will enter into this nerve ending through the same pathway and once it enter what this drug is doing this drug will capture this enzyme methyl tyrosine actually methyl tyrosine is of course structurally very similar with the tyrosine and enzyme rather than working on tyrosine enzyme unfortunately or fortunately grabs methyl tyrosine and once methyl tyrosine stick to the enzyme it really stick it forever so what happens can enzyme work for the original pathway no again listen that function
of parrosine hydroxylases to convert the tyrosine into dopa but we have given a drug methyl tyrosine which is structurally analog of tyrosine and when methyl tyrosine enter into nerve ending it will also bind with the enzyme even though this enzyme binds with the methyl tyrosine but after that enzyme cannot work forward it cannot convert methyl tyrosine into any further product so we say that in the presence of methyl tyrosine enzymes are engaged into with the drug and they are no more free to convert tyrosine into dopa so normal synthesis is blocked right So eventually there
will be no tyrosine going into dopa and eventually there will be less dopamine less norepinephrine and at adrenergic neuro effector areas total norepinephrine activity will be increased or decreased it will be decreased so this drug will be sympatho later so methyl tyrosine will be working as a sympatholic drug by binding to the tyrosine hydroxylase reducing its function and reducing the synthesis of norepinephrine so this drug is inhibiting the synthetic pathway now we come to the next drug there is another drug here that drug is going to bind with this with this pump this is dopamine
transporter right that drug will bind with this pump so very angry looking drug and you know what it does it blocked this transporter it stopped this transporter if there is a drug or substance which is taken up by these now endings and inside the nerve ending if this drug inhibits these transporter right not only here this will inhibit this transporter here also when this transporter is inhibited can dopamine enter into vesicle no and if dopamine cannot enter into vesicle dopamine will be destroyed by monoamine oxidase and vesicle will be empty vegetables will be empty they
won't have norepinephrine in right and this drug work on these transporter these Transporters are transporting the dopamine into vesicle they also transport epinephrine and norepinephrine so once once you have given this drug to any person in that person's nerve endings dopamine uptake epinephrine and norepinephrine obtains uptake is blocked and all these vesicles become empty now there will be funny situation the funny situation will be action potential will come calcium will come in vesicles will move but they won't release anything because they don't have anything I mean it's a very bad you should make a movement
against this drug But first you tell me what is the name of this drug I will tell you something else before I tell you the name of drug initially this drug was there was initially this drug was used as antihypertensive drug because it was reducing the adrenergic activity in the body but later on Doctor stops using this drug you know why because many of the people who took this drug they committed suicide you know why because of course when this drug was blocking these vesicular transport now vending for not releasing epinephrine or norepinephrine so blood
pressure went down is that right but in the central nervous system adrenergic activity nor adrenergic activity and dopaminergic activity went down and these are the neurons which keeps you excited about even small things in the life and when you're not excited by anything and you are really down all the time you are going to depression so many of these patients eventually submit its side and once doctors found this this is no more uh very important antihypertensive drug but still I don't know it's very important in USMLE and other exams and cqs because if you know
how this drug work it means you really know how this nerve ending work so please tell me what is the name of this drug anyone Alpha dopa it is not Alpha dopa it was not any dopa right even though I appreciate that you know that Alpha methyl dopar reduces the blood pressure and that also produces sometimes depression but that depression is usually not well known for the suicide because Alpha methyl dupa is still used in many countries heavily because it is one of the very inexpensive drugs so it is not that drug all of you
have heard of this drug this is called this is exactly where the razor pin hit you right what is this this friend is very unfriendly this is razor pin right am I clear no problem so how the razor pin work razor pin is actively taken up into an abundance and in the nerve endings it will block the vesicular transport mechanism so vesicles cannot accumulate dopamine norepinephrine epinephrine and vesicles remain empty and whatever dopamine is there it will be destroyed by monoamine oxidase I think this is unfair with the nerve ending right we have to report
to some federal Authority and the worst thing which they do is that they produce depression is that right now we go to another drug there is another drug rather group of drugs and that drug put a sign here stop now you are going to tell me what is the name of this drug right yes this drug right so you have to tell me what is the name of this drug the major function of this drug is it does not allow the yes does not allow the vesicles to fuse with the membrane and it stops that
activity and and it blocks the release of neurotransmitter this blocks the release of neurotransmitter again let's recap methyl tyrosine blocks the synthesis of neurotransmitter rather Bean blocks the storage of neurotransmitter now this funny guy is there it does not allow the vesicles to fuse with the membrane so it reduces the release of neurotransmitter so who is going to tell me the name of this drug yes please who will tell me so you don't want to tell me the name of this drug you know that have you heard of Guana drill britalium never heard of it
okay you hear it now this drug is called egg wanna drill d r i l 100 or another friend of this drug is britalium don't worry you will hear many things in your life first time gonadril or britallium these drugs are also acting on sympathetic nerve endings and reduce the release of neurotransmitter right so what we have learned up to now methyl tyrosine reduces the synthesis of neurotransmitter right razor pin reduces the storage of neurotransmitter reduces the release of neurotransmitters so it means all of these drugs are sympathy latex right now I tell you the
real real funny guy there is another drug which does not reduces the synthesis which does not reduces the storage it does not reduces the release of the neurotransmitter mechanism but still that drug can reduce sympathetic activity by acting on this nerve ending there's a drug which does not reduce reduces synthesis storage or release of neurotransmitter but still the drugs act on the sympathetic nerve endings and reduces sympathetic activity who is going to tell me it's my time to be impressed again that does not inhibit anything okay he he said that that drug may be inhibiting
the calcium and flux uh theoretically it's good to think like that but practically it is disastrous because if a drug can block these calcium channels these calcium channels are identical in almost all the neurons in center of a system all nervous system will shut down no neurotransmission will be there so this should not be called drug that will be a big big toxin world-class toxin don't report to any terrorists yes pardon then what it is doing there excellent Dr Nakita has given a very good answer actually there is a drug you know which was which
is mimicking the original neurotransmitter but that is a false neurotransmitter as Mr Gavin he marries the very beautiful girl but later on he discovers she is not girl that's a tragedy isn't it that is you can say pseudo woman so in the same way there can be pseudo drugs pseudo neurotransmitters he may be happily doing everything and the end is disaster right same happen there is a drug okay look at this drug look at its facial expression very happy it's going to fool you you're right this drug is what you were telling Alpha methyl dopa
what is the name of this drug yes Alpha methyl dopa it is coming with the name of Aldo mat right it is one of the very commonly used anti-hypertensive drugs and of course at this stage I will not tell one of the side effect is CNS little bit depression and comb stress is positive I will not tell you just listen the mechanism how it works Alpha methyl dopa what it is doing it is active it is taken up by the membrane by the transport mechanism right of course which transport mechanism yes same which is taking
of the tyrosine right so it is taken up by the same transport mechanism in Alpha methyl dopa and it is going to fool right it will reach up to dopa now what is Alpha methyl dopa it is just a dopam molecule with methyl group right so dopar decarboxylase will be fooled it will work on Alpha methyl dopa and D carboxylase that enzyme enter into the system and dopa D carboxylase work on this and from here what will go out carbon dioxide this enzyme is working on Alpha methyl dopa right and Alpha methyl dopa will be
converted into what Alpha methyl dopamine now this is a difference please compare in your mind methyl tyrosine get engaged with enzyme and does not leave the enzyme block the enzyme but Alpha methyl dopa is a happy go lucky type thing it goes and it binds with enzyme let the enzyme work on it and it gets converted into Alpha methyl dopamine and then leave the enzyme so enzyme is a food it is working on pseudo compound enzyme is supposed to work on dopa but it is working on Alpha methyl dopa and converting not converting the dew
point to dopamine rather converting the alpha methyl dopant to Alpha methyl dopamine and then its fooling attitude continues then it fools this neural what is this uptake mechanism and Alpha methyl dopa is concentrated into what is this place yeah into vesicles and it arrives there happily instead of dopamine you find Alpha methyl dopamine what has happened Alpha methyl Dupont entered into now vending and there it got converted into Alpha methyl dopamine then Alpha methyl dopamine is also concentrated in now cell is uh vesicle is not having dopamine it is having yes Alpha methyl dopa and
full in continues look at this Joker that this enzyme will also work on that and convert Alpha methyl dopa into Alpha methyl norepinephrine it will convert Alpha methyl dopamine Alpha methyl dopamine into Alpha methyl norepinephrine now your vesicles will be full of alpha methyl norepinephrine not full of normal epinephrine so this will sit over there in the vesicle and whenever action potential comes what will be released out what will be released out of course what are whatever is stored there you are you're still now it's dancing because it is full so much and now what
is out Alpha methyl Alpha methyl North epinephrine and this does not love to bind and stimulate these cells the real action is not there Gavin you understand what goes wrong the real action is not there right so all the this narending operators is fooled right it is somehow doing a lot of hard work to reach up to the action but there is no action because it has taken a pseudo molecule that is not dopa but Alpha methyl dupa and dopa D carboxylase convert Alpha methyl dopant to Alpha methyl dopamine then this is also food and
concentrated Alpha methyl dopamine into the vesicle then this enzyme is also food and convert Alpha methyl dopamine into Alpha methyl norepinephrine and they sleep on Happily sitting there until action potential come calcium and flux occur and vesicles happily fuse but they're regurgitate this happy lady what is that Alpha methyl not epinephrine and that does not like to have the real action of these things so sympathetic activity will go down just please the normal process to occur or the address let me tell you you are thinking that methyl tyrosine is also dealing with the end methyl
tires you are thinking that tyrosine is going in and when this is also going in maybe less tyrosine is going in yeah it does when this drug is going in tyrosine uptake will be reduced but tyrosine uptake is not significantly reduced because this nerve ending has lot of tyrosine Transporters so they do not get saturated so real competition is not at this side let me tell you your question was that when this drug is going through Transporters in then tyrosine uptake will be blocked answer is no significant blockage because now bending has lot of excessive
uptake transporter machines right due to that reason a nerve ending keep on taking the tyrosine as well as keep on taking Alpha methyl dopa the real problem occur at this level that all the enzyme machinery machinery and this Machinery this become busy with a sudo pseudo substance and original substances enzymes are not available to work on them the real difference in methyl tyrosine and Alpha methyl dopius that methyl tyrosine is a lady who is not lady ethyl tyrosine is a pseudo lady it will grab you and never leave is that right but this will fool
Youth and fool someone else and fool someone else too busy is that right am I clear so which which you will like yeah at least you'll get rid of that all right but don't worry there are a lot more coming if you keep on taking the drug regularly right anyway any question up to this there's no question okay then we can move forward that there are some other drugs which are up to now all these drugs in pathology synthesis razor pin reduces the vesicular uptake mechanism reduces the transmitter release and Alpha methyl dopa is too
much funny that it uses all the pathway and in the end up and the nerve ending end up in releasing pseudo neurotransmitter am I clear so these are all sympatholic drugs acting at different sites at the nerve and then now we come to sympatholic drugs which can block The receptors because to reduce the sympathetic activity can be divided in two ways either sympathetic activity can be reduced by reducing the function of nerve ending or sympathetic activity can be reduced reduced by blocking these receptors so there are drugs which can block these receptors right now first
of all these drugs which block these receptors we call them yes adrenergic receptor antagonist intego nest right how do you define an antagonist yes I'm about to be impressed again I think yes Nikita what is antagonist how do you define antagonist for example someone is acting against you is antagonist we are talking about molecular level yeah at receptor level really okay before you tell me new Concepts I answer look this is a very simple little bit reference to the basic concept look here these are two receptors here okay I'll make it rather same color which
is there this is one receptor and there is another receptor right now listen these are similar receptors suppose these are similar receptors and they are giving intracellular signals is that right receptor has two function number one it should bind the bind the substance and then give the intracellular signaling here now imagine the difference between Agonist and antagonist Agonist will come and bind with the receptor right suppose this is The Agonist Agonist will come and bind with the receptor Plus now what Agonist is doing number one it is binding the receptor by these two side thing
it is binding with the receptor right when a substance bind with the receptor we say substance has affinity for the receptor but when it stimulates the central point right then the real message goes in and when this drug will stimulate the central point and message will go in we say it is having intrinsic activity in the receptor so this drug can bind with the receptor and stimulate the receptor when a drug bind with the receptor and stimulate the receptor we say that it has affinity for the receptor as well as it activate the intrinsic activity
for the receptor such drugs or substances which bind with the receptor and increase the action of the receptor we call them Agonist what is the difference between Agonist and antagonists look at it antagonist is binding over here right but it does not stimulate the central point so antagonist has Affinity but not intrinsic activity your understanding so what is this now antagonist because original drug under these circumstances this original drug cannot work right so actually this is antagonizing the action of the other substance right so what is the difference between Agonist and antagonist Agonist has capability
to bind and also stimulate antagonist binds but does not stimulate is that right you want an example as you understand it okay that's good uh still I tell you something I don't know why it's I'm away from my wife for last one and a half year and all examples are related with these sense my mind is really getting something okay let's suppose when your wife is very happy with you she is having affinity for you and intrinsic stimulation so it becomes Agonist woman but suppose she's angry with you very angry with you still all the
time with you but does not allow any other woman to come near so what is this she become an antagonist entity that is why you get very frustrated you are understanding that right the Affinity is there but no intrinsic activity that's what frustrate isn't it so real difference between Agonist and antagonist drug is Agonist drug bind and stimulac and tigers bind but does not stimulate and you feel miserable isn't it right do you know what is partial Agonist I think your imagination is on wings yes what is partial agonism okay that's good let's pause yeah
he's right but let me make a diagram when full agonists bind suppose it is giving double action n and of course here there is no action when it bind it does a double action so what is it full Agonist when it binds and there's no action it keeps around you but no action what is it and okay to sacrifice my diagram a little but I think it's worth it and now we make another receptor and see how the partial Agonist is working partial Agonist is some girlfriend and only in the beginning of the relationship they
will bind right and partially stimulate but there's no action here so there is an intrinsic activity but not full there's only partial intrinsic activity other is not there so what is this partial Agonist bind but stimulate partially is that right so this is partial Agonist what is partial antagonist how do you define partial antagonist I have to make another diagram no this is partial antagonist also when you have a girlfriend in early relationship right she's just checking are you worth to the father of our children or not during that time just to keep you around
she have affinity and partial Agonist activity but not the full action right but unfortunately she does not allow the other person to come and have full action foreign and does not trust you fully if she is wise right so what is this that this molecule itself is producing little stimulation but does not allow the other molecule to come and do the full stimulation so this molecule this molecule is partial Agonist as well as partial antagonist this partial Agonist because partly it stimulate and partial antagonist because it does not allow the other molecule to come and
produce full stimulation is that right okay there is another concept mixed Agonist and antagonist these are the very basic concepts in Pharma and you should be Crystal Clear what is Agonist Agonist will bind and stimulate fillet antagonists will bind but no stimulation at all miserable antagonist partial Agonist antagonist is like a girlfriend in the early time bind stimulate a little don't allow anyone to come and do full stimulation right so what is mixed Agonist antagonist so when it like um yeah actually this concept can come from here that sometimes like opioid receptor opioid receptors are
multiple sub like mu receptors copper receptors or Deltas after there multiple types so one receptor may be like this right other receptor may be like this now what really happens the same drug at one side right it binds it binds as well as it stimulate so it is Agonist here but the same drugs goes and bind with another receptor but or for other receptor it does not look same drug goes and bind with another receptor but it is not near to stimulate so this drug a drug a at receptor one is binding and stimulating but
at receptor 2 it is binding but not stimulating are you understanding that but binding and stimulating binding but not stimulating so same molecule at one side it is Agonist and other side it is antagonist so such are called mixed Agonist antagonist compounds mixed Agonist antagonist compound do you really want another real example that will be very sad I don't want to give your example there's a man his wife is very angry very angry and she remains his wife very very angry and not stimulating him so right but having some private time with her ex-boyfriend so
Jesus what is here antagonist is there Agonist so she has a mixed activity and of course you don't like it right so that is mixed Agonist antagonist but it is more true about men isn't it especially when I look at you hahaha right I was just kidding I know you are not like this and even if you are you'd never tell anyone I know all right so having said all of this now I'm going to tell you the adrenergic drugs which bind with the adrenergic receptors I'm going to talk about the drugs which bind with
adrenergic receptors but don't stimulate them such drugs will be adrenergic antagonist such drugs will be adrenergic antagonals and of course they should be classified as sympatho latest drugs right so sympathetic drugs some of them are going to block mainly Alpha receptors let me tell you adrenergic receptors antagonist IC receptor antagonist from where we went to the discussion of Agonist antagonist that antagonist or drug which will bind to the receptor but won't stimulate and don't let the endogenous epinephrine norepinephrine to stimuli angry wipes receptor antagonist now these drugs some of them block Alpha and some of
them block beta receptors right and Alpha blocker Alpha receptor blocker some of them block Alpha One as well as Alpha two they reduce the activity at alpha 1 and Alpha 2 and some of them only block alpha 1 reduce the activity of only Alpha One is that right and of course there are some which block yes beta 1 and beta to both they block both of them and some of them block only beta 1 beta 2 pure Blocker we don't use clinically right so I will not talk about that so a drug which will block
alpha 1 and Alpha two it means that is drug is blocking here as well as blocking here the example is yes phenoxy phenoxy benzene yes and Benzene one drug is phenoxy Benzene other is phentolamine fan Tola means these two drugs bind with Alpha One and Alpha 2 receptors and block their activity so the alpha blockers what is the difference between phenoxybenzene and phentolamine of course spellings what else what is the difference between phenoxybenzamine and phentolamine anyone who has studied some pathologist drugs no one has studied ever of phenoxyl benzamine is Two Loving molecule once it
bind with the receptors it binds it irreversibly but phentolamine binds but with high concentration of epinephrine and norepinephrine it can be displaced so the real difference is phenoxybenzamine is irreversible receptor blocker and phentola mean is reversible receptor blocker so if someone take a drug which will irreversibly block The receptors do you think we'll ever recover from the function of that tissue answer is yes because old receptors will be catabolized and eventually new receptors will be synthesized by the tissue if person survives I think it's a very basic concept listen the drugs which bind The receptors
irreversibly of course they block the activity for long time but actually the drug which complex with the receptor in a covalent fashion and block the receptor forever that receptor complex will be eventually catabolized receptors are not there forever in every tissue most of the receptors are under turnover old receptors are being catabolized and new receptors are being synthesized so actually when irreversible drug bind with the receptor or we also call it non-competitive blocker non-competitive because if you bring the competition with high dose of epinephrine or non-epinephrine still this drug will refuse to dissociate from alpha
receptor this non competitive irreversible Blocker of alpha receptors it will keep on blocking for the life of the alpha receptor not life of the person is that right until the new receptors are expressed but phentolamine it is little bit decent it binds with the alpha receptors but if High concentration of agonists come it can be displaced so this can be called competitive blocker am I clear then there are drugs which mainly block only alpha 1 receptors yes you will tell me the drugs which block only alpha 1 receptor at least tell me two names I
don't want 20 names at least tell me presocent and trousers and oh my God Prezzo send and Razzle since they are very commonly used as antihypertensive drugs prazosin is present in mini press anyway present they preferably block alpha 1 receptor very commonly used as antihypertensive agents these are alpha one receptor blockers again I want to know what is the primary difference between present and transition what is the basic the single difference you are supposed to know single again don't tell me the spellings yes what is the basic one difference between presence and transition which is
clinically relevant when you treat your patients is long Half-Life so here patient has to take maybe three tablets a day here he has to take one table at a day it's a big difference clinically for the patient because when patients take drug three times they feel more sick and feel more inconvenience so brother sin was the original Dragon later on they found prazosin which can be given once a day all right am I clear we'll discuss every drug in detail later now we come to beta blockers of course beta blockers are non non-selective beta blockers
and selective beta blocker non selective block beta 1 and beta2 both receptors and selective block only beta 1 so you will tell me non selected beta blocker don't tell me many drugs just tell me one drug propranol excellent everyone should know proprano [Music] LOL it blocks beta 1 and beta 2 both receptors of course there will be big discussion about this drug later because it's very commonly used it has a lot of indication and it is very important contraindications and side effects we'll talk about that later and there are drugs which are beta 1 blockers
they are specially used to inhibit the sympathetic activity at heart I don't want many name at least tell me one or two tell me Mito LOL never heard of them Mito Pro LOL or Teno law so these are the all drugs which bind the adrenergic receptors but they do not stimulate them they are like Angry wives right and receptors are block even for the endogenous epinephrine norepinephrine activity any question after this there's no okay then we come to the drugs okay let's come to the some drugs which are work on this system but stimulate the
system of course those will be sympatho nemetic let's recap this and then we'll go to sympathome limited drugs acting on this operators first little bit recap we were talking about sympatholic drugs sympatholic drugs can directly block The receptors or they can indirectly by acting on sympathetic nerve ending reduce sympathetic activity right now sympathetic sympatholic drugs number one now you will tell me a drug which reduces synthesis of synthesis of norepinephrine the drug is methyl tyrosine a drug which blocked the vesicular transport and storage of the neurotransmitter razor pain a drug which basically blocks the release
of neurotransmitter and Drug which work throughout the mechanism of dinner bending and come out as a pseudo neurotransmitter Alpha methyl dopa and then the drug which is in pathology drug we directly block The receptors first of all Alpha blocker non competitive Alpha blocker R which block alpha 1 and Alpha to both receptors they are phenoxy Benzene and pentolamine which is irreversibly binding right and other is reversible binding then Alpha One blocker purely presence which has a longer duration of action transition then beta blocker non-selective classical drug propranol and beta1 selective blockers remember these drugs in
high concentration also start blocking beta2 beta1 selective blockers are selective only at low Doses and low concentrations if you give atenol LOL or metoprolol in very high concentration just start blocking the beta2 also right Mouse then we come to okay let's have a break and then we'll continue right now on the same neural Factor operators we will discuss sympatho magnetic drugs the drugs which increase the sympathetic activity you know there are two ways to increase the sympathetic activity number one is some drugs go directly to the receptors on the post synaptic surface or on the
effector tissue and drugs directly stimulate the receptors if a group of drug is directly stimulating The receptors right we call them Direct sympathomimetic drugs so pathometric drugs okay let us classify them here it's in patho my Matrix drugs as a broad category these drugs produce the pharmacological actions which may make to the physiological actions of sympathetic nervous system right now these sympathomimetric drugs are direct acting and indirectly acting direct acting and end directly acting sympathomimetic drugs right direct acting mean the drugs which directly stimulate the adrenergic receptors drugs which directly stimulate the adrenergic receptors these
are adrenergic receptors agonists and indirectly acting sympathometric drugs are those drugs which act on the nerve ending sympathetic nerve ending right and alter the function of the sympathetic nerve ending right in such a way that amount of norepinephrine released by the nerve ending is more or amount of not epinephrine present in synaptic area is more than normal I will explain what are these drugs and how do they work so what are indirectly it's in pathometric drugs indirectly some pathomimetic drugs do not work directly on the receptor on the postsynaptic surface they work on sympathetic nerve
ending and alter some act function here to keep or release more norepinephrine or neurotransmitter in the synaptic cleft and of course when there's more neurotransmitter here it will act on the receptor in a more intensity so this such drugs are called indirectly acting drugs you want to learn about directly acting drugs first or indirectly active direct action first that's easy right directly acting drugs are which will stimulate these receptors directly for example this Alpha One stimulant drug Alpha One and Agonist or their alpha 1 and Alpha Two Against Two Against there are some drug which
are alpha one stimulant beta 1 stimulant and beta2 stimulant then there are drugs which are beta 1 and beta2 stimulant there are drugs which are mainly beta2 stimulant there are some drugs which are mainly stimulate alpha 1 receptor the some drugs which will stimulate Alpha One and Alpha two OK rather we should put here little bit change look here drugs which mainly stimulate only Alpha One receptor drugs with mainly stimulate only Alpha two receptors and Drug which stimulate Alpha One receptor beta 1 receptor and beta2 receptors drugs stimulate mainly beta 1 and beta 2 and
there are drug which stimulate mainly beta 1 and drugs which stimulate mainly beta2 how many categories one two three four five and six categories is that right let's move step by step first of all the drug which will stimulate Alpha One okay I will remove this area and compare and contrast them the drug will stimulate only alpha 1 receptor yeah mainly Alpha One receptor they bind with the Alpha One receptor and stimulate here right who will tell me the name of such drugs phenyl efferine have you heard of phenylephrine so phenylpherine is the drug is
mainly Alpha One stimulant is that right phenylephrine then we go to the next drug which mainly stimulate Alpha two this is Alpha One stimulant now we come to drug which Alpha two stimulant now it is very interesting to look at it that if there is a drug which is Alpha two stimulant it will stimulate here it has stimulatory action on Alpha two you know what will happen it is sympathomemetic or sympatholytic use your own head if a drug is stimulating here it means it is giving the message to the nerve ending there is lot of
neurotransmitter here nerve bending will be inhibited and release of neurotransmitter will be less so this is an unusual exception that a drug which act on presynaptic Alpha two receptors and stimulate them too much it is giving message to the nerve ending there is lot of norepinephrine here and actually norepinephrine release will be less and it will become sympatholic this is a very tricky tricky situation are you understanding me anyone who could not understand right so does this stimulate Alpha two receptors basically they inhibit the neurotransmitter release it's an unusual situation but if there's a drug
which block this which block this right to the blocker a drug can block Alpha two receptors it means nerve ending is releasing the neurotransmitter but it is itself blind it is totally blind to the amount of neurotransmitter present here because when this receptor is blocked whatever norepinephrine is released can it stimulate this receptor no when this receptor is not stimulated nerve ending receive the message that probably there is no neurotransmitter there so nerve ending will start releasing more neurotransmitter are you understanding so it's a very unusual situation when you talk about the alpha two receptor
stimulant and blocker right Alpha 2 receptor on presynaptic nerve ending are the eyes of the nerve ending by which they look at the amount of neurotransmitter at the synaptic left this is synaptic cleft neurotransmitter sensor for the auto inhibition when you have a drug with stimulate Alpha 2 receptors right then now when you stop releasing the neurotransmitter but if you have a drug which inhibits Alpha 2 receptors drug which inhibit the alpha two receptor now ending will no more inhabited and it will release excessive amount of norepinephrine now can you tell me some drug which
can stimulate Alpha 2 receptors please tell me a drug which can stimulate Alpha 2 receptor and nerve ending will be too much inhibited and it will not release neuro transmitter the drug is you know it you know it I can bet it you know it drug is Clonidine have you heard of clonidine clonidine in central nervous system at Vaso motor Center in medulla it bind with Alpha 2 receptors and stimulate them it stimulates them and nerve ending the food they think they have released too much norepinephrine they stop releasing the norepinephrine so Vaso motor Center
is inhabited when Visa motor Center is inhibited then from middle are down going sympathetic flow and whether motor sympathetic outflow all is inhibited and blood vessels dilate and blood pressure goes down so such drugs which are alpha to stimulant are anti-hypertensive like clonidine okay here I'm saying Alpha two stimulant that is but remember this is not sympathomagnetic this is an unusual sympatho Central sympatholic Central Central mean in the central number systems in patho lead tech clonidine this is unusual situation the receptor is stimulated but it inhibits the nerve ending a release or norepinephrine become less
and Vaso motor system is inhabited and blood pressure goes down is that right there are two Central there are two important Central anti-hypertensive drugs one is Clonidine right which stimulate Alpha two receptors inhibit the now adding those sympathetic nervous nerve ending of noradinergic system in Vaso motor center Visa motor Center is inhabited other centrally active drug is centrally acting antihypertensive drug is Alpha methyl dopa that also work on the vessel motor Center but in a different way Alpha methyl dopa as I told you will be taken up by the system and release as pseudo neurotransmitter
and again neurotransmission fails so clonidine reduces the discharge of normal norepinephrine from the nerve ending but Alpha methyl dopa lead to the release of pseudo neurotransmitter and reduce synthesis of original neurotransmitter Amic layer so Alpha One stimulant is sympatho memetic but Alpha two stimulate is stimulant is sympathy latex this is very unusual point then we come to a drug which can stimulate Alpha One also stimulate okay I will talk about beta1 but very little action on beta2 what is this drug it has now not first drug was having action only on Alpha One phenylephrine now
we have a drug which has Alpha One action and beta one action but not beta2 what is the drug please tell me please tell me which we are studying from last two hours the very specialty of norepinephrine is stimulate alpha 1 and beta 1 but does not stimulate beta2 significantly right nor have in a frame am I clear really okay go one more step come to another drug which will stimulate Alpha One beta 1 and now we have a drug which also stimulate beta2 right alpha 1 beta 1 and beta 2 all of them are
stimulated what is the name of this drug yes ma'am excellent it is epinephrine so my dear students the real difference in norepinephrine and epinephrine is norepinephrine has Alpha One beta one action but less beta2 epinephrine is really balanced it's simulate alpha 1 beta 1 and beta 2 all of them if you really know receptor distribution in the body but this simple thing you can tell the action of the drug of course norepinephrine does not have beta2 actions and epinephrine does have for example beta2 action is bronchodilation norepinephrine will not do bronchodilation epinephrine will beta 2
action on the liver is glycogen lysis right so this will not do glycogenolysis but epinephrine will do glycogenolysis and we'll talk these things later let's move forward now funny thing another drug which does not evolve for one action but has mainly beta 1 and beta 2 action look at it we started the drugs with main Alpha One action full Alpha One action then we came to drug which has alpha 1 and beta 1 action then into the drug which has Alpha One beta 1 and beta 2 action now we are reducing the action of alpha
one we are left with which actions mainly beta 1 and beta 2 what's the name of the drug which is mainly stimulating beta 1 and beta2 I'm about to be impressed by that lady okay this young man excellent isoproterinol very good ISO protein all you know it's so easy now if you know the beta one beta two action the body these are the actions of the piece of protein now but if you add Alpha One action to this you get epinephrine and if you have Alpha One beta one action and reduce the action of beta
2 reflection of norepinephrine is it difficult I don't know why it is so easy okay now we come to little more thing we come to drug which is mainly beta 1 action and then of course drug which is mainly beta 2 action actually we have a drug which has in a very high doses Supra physiological doses there's a neurotransmitter or hormone which has beta1 action but if those become very high then it start Alpha One action also it has little Alpha One action but in very high doses it will start Alpha One action yeah and
it has dopamine receptor action also there's a drug which stimulate dopamine receptors it can also stimulate beta 1 receptors and in very high concentration can stimulate Alpha One action what is the name of the drug dopamine very good dopa means so dopamine can stimulate beta1 receptors in the heart and increase cardiac output and dopamine at the same time can act on dopamine receptor on renal vessels and dilate them let me tell you this tricky thing listen if a patient comes to you who is undergoing severe reduction in cardiac failure there is less cardiac failure and
due to reduced cardiac failure there is so little you know blood flow to the kidney that you are about to have acute tubular necrosis you know when there is severe ischemia to the kidney you are going to have a cute tubular necrosis renal shutdown so if you have a patient with cardiac failure and Associated risk of what renal shutdown due to reduce renal blood flow you have to do two things you have to stimulate the heart you have to dilate the renal vessels simultaneously and we have a double action drug which has beta one action
on the heart and dopamine receptor stimulation on the renal vessel and you will protect increase the cardiac output and that drug will be Reno protective as well protect the kidney from acute tubular necrosis the drug is dopamine that is why in very severe shocks when cardiac output is down we give infusion of dopamine that it should stimulate the cardiac output and keep the renal vessels dilated is that right but you have to be very careful every good thing does not remain good under all circumstances if unfortunately you give excessive dose of dopamine at very high
concentration starts stimulating alpha 1 receptor and when Alpha One receptors are stimulated in the renal vessel we will again shut down so what happens you have to give moderate Doses and take very good care that infusion rate is well controlled you will study when I will teach you dopamine that dopamine has very good dopamine receptor stimulation at 2 microgram I should not go into detail of that right now just trust me at very low doses dopamine stimulate what dopamine receptors and dilate the renal vessels in moderate doses beta one action start and also become cardio
stimulant at very high doses unfortunately start stimulating Alpha One receptors and that may lead to again renal vessel Construction does that write any question after this no but if you have another patient who has no problem of renal vasoconstriction only cardiac output is down if you want to give a drug to a person to stimulate his heart you want to stimulate his heart increase cardiac output but you don't want renal dilation you don't want renal dilation because there is not so much shock that person is going into acute tubular necrosis then dopamine is not the
drug of choice you want a drug which mainly work only on beta one receptor you want a drug which mainly work on okay I will put it here drag which mainly work on beta 1 stimulant and not stimulating the dopamine receptor what is the name of the drug again listen there are two patients with reduced cardiac output in one patient you need to stimulate the heart and dilate the renal vessels to protect the kidney from acute tubular necrosis the choice of drug is dopamine another patient is reduced cardiac output you want to keep the heart
little bit stimulated but there is no problem with the kidney such such patients are classically like heart transplant patient and heart is transplanted you give some sports stimulant to the heart so that in new environment it keep on working is that right very good Dr Rose has told us this drug is dough butamine we'll study all these things in detail but right now you only remember that dopamine is cardio stimulant and renodilator Reno vessel dilator but dobutamine is mainly cardio stimulant am I clear there's no problem and then we come to a very important group
of drugs which are mainly beta2 stimulant yes salbutamol albuterol writer drain the very commonly used for specially salvation all albuter all these drugs are used as bronchodilators right so I put it here Sol buta law so all of these drugs are sympathomemetic because they increase some of the function of sympathetic nervous system in the body right but because all of these drugs are working on the receptor so we can call them directly acting sympathomimetic drug only one exception was Alpha 2 stimulant which was indirectly acting sympatholic in this whole story write remember clonidine was not
sympathomable may take it is sympatho latex even though it stimulates the adrenergic receptor am I really clear anyone who is confused raise your hand no one is confused okay now we come to the drugs which really work on presynaptic nerve ending and increase the sympathetic action right for that purpose first of all I will tell you a drug right which works here on this reuptake mechanism and this drug which what it is doing this drug is what this drug is doing it is blocking the reuptake mechanism now what will happen you are yourself intelligent that
can it go in no so it will be staying here a drug which bind with reuptake one mechanism right and whatever neurotransmitter is released the recapture of or re-uptake of neurotransmitters reduced so neurotransmitter stays here longer in higher concentration and it really works more so what we have done we have got stimulation of The receptors indirectly so you call it indirect sympatho mometic drug can you tell me the name of this drug yeah okay remove the tail and put the name what's the name of this drug pardon of course he's so intelligent he tells me
it is reuptake Inhibitors he's right these are reuptake Inhibitors I want the name of the drug yeah or toxins I think this is something all of you must know have you heard of something called cocaine of course it's drug but illicit drug what cocaine does when you take cocaine you become hyper stimulated you must be knowing Gavin right so don't laugh at him she never told me right so what happens when you take cocaine cocaine goes and bind with a sympathetic nerve and then and block the reuptake so whatever normal amount of norepinephrine is released
it stays there and stimulates in central of a system because cocaine is lipid soluble goes into central nervous system right and sympathetic Drive is more and you feel hyper stimulated and excited some people like situations like this right but cocaine does it with very strong cocaine but there are some drugs also we use I mean there are drugs they also bind it with very and slow down this reuptake the little bit block this react mechanism but little bit so that concentration of norepinephrine remains in this area little bit High right those drugs bind with these
reopter mechanism at dopaminergic neurons at noradrenergic neurons at adrenergic neurons so multiple neurotransmitters in central nervous system their concentration is increased in synapses what is the group of that drug called yeah no all of you know that all of you know that have you heard of tricyclic antidepressants this is what tricyclic antidepressants are doing tricyclic antidepressants tricyclic antidepressants what they are doing they bind with reuptake one but not as strongly as cocaine because they are not cocaine right they bind it mildly and the slightly reduced the reuptake and they keep on increasing the concentration of
these excitatory neuron in the central nervous system synapses so that you come out of depression is that right we'll talk their actions in detail when I teach you tricyclic entity depressants of course there will be time for that also one day any question up to this and I think it's very important to tell at this stage have you heard of the drug Prozac ssris what is that ssris ssris yes selectives proton in reuptake inhibitors classical example is Prozac what Prozac is doing I think what is the active drug in the project no that is the
paroxetine is related with that fluoxetine fluoxetine what is the drug in Prozac in okay yeah Paxil as peroxide 10 and fluoxetine so fluoxetine or paroxetine or relative drug they are also reuptake Inhibitors but they selectively block reuptake mechanisms only on serotonergic neurons so that that is why they are given selective serotonin reuptake inhibitor because tricyclic antidepressants are non-selective they inhibit the reuptake of epinephrine they inhibit the reuptake of norepinephrine the inhibitor reuptake of dopamine am I clear so tricyclic antidepressant act on the reuptake mechanisms in central nervous system and don't allow that released neurotransmitter to
be reuptaken concentration of adrenergic neurotransmitters and synaptic area become more and there's more action on the adrenergic receptors am I clear right and there's another way to increase the release you know how okay let me tell you you put you block this cat mouth right you put a drug right and this is like a basket and this is trapped and now when norepinephrine is coming back can it be destroyed by this so it will be accumulated here and effectively reuptaken into physical so whether all the norepinephrine which is coming normally a part of it is
destroyed by Mao and part of it is restored stored again into vesicle but if drug blocks monominoxidase system then whatever is reuptaken if of course this drug is not there whatever is reuptaken right that will be all of it will be stored there and store the neurotransmitter stored in the vesicles will be very high so with every action potential extra amount of the drug neurotransmitter is released and it becomes a sort of sympathomimetic action to mild degree what is the drug here yeah these are also antidepressant drugs because they increased neurotransmitter concentration here yeah who
is going to tell me what is the drug here any one this drug is number one Cargill I don't know from where they find this name pargai Len p a r g y l i n a how you read it per gallon and Other Drug is prenial cypromine renal Cipro men these are also monoamine oxidase inhibitors and they are also used as anti-depressants again we will discuss into detail when I will teach 20 depressants right so one way to increase neurotransmitter here is don't allow the reuptake other is allow the reuptake but don't allow intra-neuronal
destruction so everything will be stored over there right and then last group of the drugs which facilitate binding of vesicle with this membrane so they're really they increase the release of neurotransmitters there is another group of drugs which can enter into the sympathetic nerve endings and help and accelerate the fusion of vesicles with the nerve membrane and release neurotransmitter more efficiently right so what is this drug now now I think you must answer there are drugs which go into central nervous system bind with sympathetic nerve endings or we can say adrenergic and non-energic and dopaminergic
nerve endings and lead to excessive release of these neurotransmitter name of the drug is which will stimulate you a little bit yes you know it your all friends may be taking it near the exams amphetamines you never heard of it amphetamines right these are m beta means amphetamines right these are also increasing the release of adrenergic neurotransmitters and central nervous system and also with amphetamine the other drug is Tyra means please don't confuse tyramine with a tyrosine and don't confuse paramine with Alpha methyl tyrosine right Alpha methyl tyrosine inhibit that or tyrosine hydrophilase and reduces
sympathetic activity but tyramine helps the physical to fuse more efficiently with the membrane and increase pathetic activity that's all for today do you have any question no question you are talking about that is a very unusual drug that is Alpha blocker as well as beta blocker we'll talk about it when we'll discuss into detail sympatholic drugs it was just a very brief introduction to put some basic concepts in your mind we'll talk about a little bit of all that is Alpha blocker as well as beta one blocker Plus libital has one more action we will
discuss it activate the potassium channels let the potassium leak out of the myocardial cell and reduce their restroom membrane potential we'll talk about these things later right any more now today we are going to talk about the distribution of different types of adrenergic receptors on body tissues right as you must be knowing already that some tissues level for one receptors some tissues have beta 1 adrenergic receptors right and we have to see that why different tissues in the body have different type of adrenergic receptors right we were talking last time that uh Mr Gavin was
followed by a big black dark dog right and we have already discussed that his central nervous system was activated and there was Heavy sympathetic outflow and that sympathetic outflow was releasing norepinephrine from the nerve endings to multiple tissues and Adrenal medulla was releasing epinephrine in general circulation so when Mr Gavin was under stress of that dog right his biological system was under the influence of norepinephrine and epinephrine now when epinephrine and norepinephrine will act on different tissues on the body and work on the different organs on the body they should modify the performance and function
of the different tissues in such a way that those organs and tissue which help to fight the stress those organs should be stimulated and those organs which do not help to fight with the stress right those organs should be inhabited for example dog is after you you are running on the road now heart can help you by increasing cardiac output so heart should be stimulated opposite to that git at that very moment that is the not the time to digest the chicken piece you ate one hour back you have to see you have to save
your own leg piece isn't it so git act tissue activity should be increased or decreased decrease so by this example what I am saying when we are under stress and sympathetic nervous system is firing a lot of norepinephrine and epinephrine is being released in our biological system epinephrine and norepinephrine is going to work on multiple tissues through adrenergic receptors and adrenergic receptors should alter the body organs and tissue system function in such a way that those organs which help to fight the stress they should be stimulated and those organs which do not help you to
fight the stress or flight from the stress those organs and tissues should be inhabited so we can say that biological response to sympathetic stimulation right we say biological response biological response to stress right under yes please under sympathetic sympathetic activation sympathetic nervous system is activated what should be the biological response to the stress and the sympathetic nervous system activation sympathetic nervous system should sympathize with you activate the tissues which can help you to fight the stress and inhibit the tissues which do not help you to fight the stress so it means all biological responses can
be divided into basically to part right that tissues to be stimulated tissues and organs to be stimulated issues and organs stimulated right right and of course there must be tissues and organs inhabited tissues and organ function inhibited right of course the tissues and organs which are stimulated are those organs which are going to fight you stress and tissues and organs functions which are inhibited at those tissues which don't help you to fight with the stress right as we have discussed heart should be stimulated is that right so that cardiac output should be more and you
should provide more blood going to the muscle so that you can really run away from the danger or fight with the danger opposite to that as I told you gastrointestinal system at that very moment when you are under extreme stress should be inhibited right you can digest the digest absorb the G80 contents later on first you save your life is that right now how it is mediated why some tissues are stimulated how some tissues are stimulated and other tissues are inhibited this is a very interesting question that same neurotransmitter and hormone are stimulating one tissue
and inhibiting other tissue answer is very simple neurotransmitter is same on these tissues and that tissue but these tissues have stimulatory receptors and those tissues have inhibitory receptor that is for sample we don't need to be too clever for this thing it's very easy to understand that in these tissues there should be receptors which are stimulatory they are adrenergic receptor the macromolecule which responds to epinephrine and norepinephrine but they produce stimulation of the tissue and here should be such adrenergic receptors that once once they are activated they are actually leading to inhibition of the tissue
now it's so simple again how all the receptors which are stimulatory they are number one for example adrenergic receptor Alpha One adrenergic receptor they are stimulatory right beta1 adrenergic receptors are stimulatory and when we talk about Alpha two adrenergic receptor these are look these are generalizations there are few exceptions but first learn the general general principles Alpha 2 adrenergic receptors they are inhibitory to the tissues beta2 adrenergic receptors they are mostly inhibited to they are inhibitory to certain biological activities in the body so same epinephrine which will go to one tissue act on Alpha One
and stimulate that tissue and same epinephrine go to another tissue having beta2000 receptor and tissue will be inhabited let me give you classical example let's suppose this is your circulatory system right and here is a blood vessel which is going to the kidney and here is a blood vessel let's suppose which is going to the muscle it's going to the skeletal muscle now listen carefully when dog is after you you are under stress blood flow to muscle should be increased blood flow to muscle should be increased so increase blood flow so epinephrine and norepinephrine or
catecholamines should increase the blood flow to skeletal muscle so that you can run away from the dog or you can fight with the dog whatever you choose to do right but blood flow to kidney should be increased or decreased yeah I think he thinks increased right blood flow to kidney should be decreased because renal blood vessels should construct so that blood should be diverted to more important area because if you dilate the kidney blood vessel last time the student was telling that blood vessels to kidney should also dilate I ask a simple question do you
think you are going to urinate on the dog that is not a good way to fight it is that involve the big risk isn't it actually that is the not time to make the urine and things like that right you can do it later that is the time to construct your renal blood vessels save the blood and divert to the dilated blood vessels going to the muscle so blood flow should be decrease blood flow to the renal side am I clear now question is how the same neutronsmeter is dilating one blood vessel and how the
same neurotransmitter is constructing other blood pressure is that right we'll talk about the tone of vasomotor tone in this area and vasomotor tone in this area ah let me disconnect this vessel I remove this vessel vessel from the skeletal muscle and bring it down this is a blood vessel from the skeletal muscle and let's suppose I make a section of it this is the blood vessel from the skeletal muscle and these are it's smooth you know blood vessels have in their media what are these smooth muscles is that right now there are smooth muscles in
the blood vessel going to the skeletal muscle and of course let's study this blood vessel also what is this blood vessel yes renal blood vessel and of course there are smooth muscles here also present am I right now the concept which we have to develop as that under the same influence of the same neurotransmitter why the renal blood vessels construct and why skeletal muscles blood vessels yes dilate right because if we take a container if we take a container and dip these blood vessels into this container and this container is having a fluid rich in
epinephrine and norepinephrine epi nephrine yes and nor epinephrine now this lot of epinephrine and norepinephrine into this fluid both blood vessels are dipped into that this blood vessel should what construct and this should dilate to constrict this blood vessel the smooth muscles of this blood vessel should be stimulated or inhibited you have to stimulate the smooth muscle here because when you stimulate this smooth muscle they will construct right so it means that this this smooth muscle I remove one smooth muscle from here this smooth muscle of this blood vessel this should be stimulated so that
the blood vessel should construct right opposite to that the smooth muscle here the smooth muscle I show one smooth muscle big smooth muscle here uh in the skeletal muscle blood vessel right it should relax because when these smooth muscles will relax they get inhibited they will open up the vessel and more blood flow will come to the muscle so it means there should be stimulatory receptor here and there should be inhibitory receptor here so the stimulatory receptor here should be Alpha One adrenergic receptor there should be yes Alpha One adrenergic receptor when epinephrine will bind
with Alpha One adrenergic receptor there will be stimulatory signal and these smooth muscles will construct and blood flow to kidney will be reduced opposite to that this smooth muscle which is from the skeletal muscle blood vessel right we want this to relax so this smooth muscle should have stimulatory receptor or inhibitory receptor and Inhibitors separate from this group it has the beta 2. it has the beta two receptors so what really happens that when epinephrine epinephrine work on the Alpha One receptor on blood vessel smooth muscle blood vessels construct when epinephrine work on the beta
2 recept adrenergic receptors on the smooth muscle the blood vessels blood vessels dilate this is how the one neurotransmitter right epinephrine and norepinephrine right or other catecholamines by acting on Alpha One receptor they are producing vasoconstriction of renal vessel because smooth muscle then are stimulated and they construct apples to The beta2 receptors present on skeletal muscle vasculature right so when epinephrine and norepinephrine work on the beta2 receptor especially epinephrine when it work on The beta2 receptors on the smooth muscle the blood vessels blood vessels dilant so this is a very simple example that what I
was saying the hair smooth muscle will construct and that will help the biological system and their smooth muscle should relax and dilate that will help the biological system under stress so the tissues hair smooth muscle so smooth muscle here should be stimulated and there should be inhabited I hope it makes some sense now we'll apply the same principle all over the body from head to toe that how logically receptors should be distributed on different tissues later on it will become so easy that if I say drug as mainly Alpha One action you can logically think
which tissue the Alpha One action and what are the pharmacological actions if I say later on that drug has beta two actions you automatically think which tissues logically should have beta2 receptors and then you can infer the pharmacological actions so let's complete this thing come back all the tissues and organ which help to fight the stress should be stimulated and they should have stimulatory receptor Alpha 1 or beta1 all the tissues which do not help to fight with the stress should be inhabited right and they should have inhibitory adenergic receptors Alpha 2 or betato is
that right now after that we will make a general statement here right one general statement the general statement here which we are going to make is that all the tissues all the tissues to be stimulated now this is what you have to understand very clearly stimulated have Alpha One adrenergic receptors except except which tissues all the tissues to be stimulated have Alpha One adrenergic receptor except number one heart number two in the kidney juxta glomerular operators and what is this cell adipocyte now listen carefully what I really mean by this all the tissues to be
stimulated should have alpha 1 receptor except heart just glomerular operators in the kidney and deposite fat cells these are having not Alpha One they are having beta one so these tissues will have which receptors heart should have beta 1 receptors juxta yes juxta glomerular operators should have beta1 and adipocyte should have beta1 now listen actually Depot sites have beta 3 beta 3 receptors are modified beta1 that is why we can put it with beta1 beta3 receptors are on the fat cells or adipocyte they are modified yes they are modified beta1 so lesson again when sympathetic
nervous system fires in my body if I say 20 tissues are stimulated all of them will have Alpha One receptor except these three tissues which are beta 1 am I clear now we go to another General principle right and that principle is that all the tissue to be inhibited all the tissue to be inhibited should have yes should have beta 2 adrenergic receptor except following which have Alpha 2 except presynaptic nerve endings yes except pre synaptic nerve ending which have Alpha two hydrologic receptor Plus platelets platelets which have Alpha two receptors plus insulin producing cells
which are insulin producing cells insulin producing cells is a beta cells of pancreas but they have Alpha two they have Alpha two do you think and stress you need more insulin or less insulin oh my God my friend is saying that there should be more insulin so what happened dog bark at you lot of insulin come glucose go into cell you develop hypoglycemia and you become like this in front of dog it's not a very good approach isn't it because you need a lot of stressful circumstances you need your brain to work and brain needs
oxygen of course with oxygen brain needs lot of glucose and to keep the glucose supply to the brain you have to keep the blood glucose level high and for that purpose you should release more glucose from the liver and it should not release insulin and Insulin should not push the glucose into cells peripheral cells am I right so it's very logical that when you are under stress you need more glucose for the brain right do you need to release massive amount of insulin no so insulating cell should be stimulated or inhabited inhabited so naturally they
will have which cells Vision receptors inhibitory receptors what receptors are now Choice Alpha 2 or beta2 but I said in this general rule all the tissues to be inhibited have beta2 receptors accept these three so it should have Alpha two I hope this is making some sense up to now right now start studying the real tragedy which is going on dog after you and okay here you are foreign and this is the dog after you and Lucas Trail aggressive he is very happy he caught you he's about to catch you I think it should be
in action also I don't know how to make dog in action but anyway so it's rapidly coming here right it's coming to you right now we have to see from here up to here what are the changes in your body is that right by under the influence of adrenergic system right now we start from the top what about your hair under stress what should happen to your hair I'm not talking about my hair yes they stand up why how they can why here should stand up and how they can help you to fight with the
stress today yeah actually you know what happened it's a lower animal response we have evolved from lower animals you know even though we think other things all in the lower animals you have seen when uh those fight the husbands of the hands when they fight what they do they make their hair like this what they are doing they are trying to increase their apparent side and scare the other enemy so under stress in Jungle life there are two types of stress number one you are fighting with other animals so your hair should stand up right
and you try to apparently increase your size and scare the other animal and secondly another stress is really very cold weather right so the hair should stand up and air should be trapped and some temperature isolation so what really happens under stress here's stand up still is that right so again under the stress hair should stand up and you know that if this is the skin here is your what is this here follicle and here you're beautiful here right now there is a muscle here we call it this muscle should be stimulated or inhabited it
should be stimulated to erect the hair it should be stimulated can you tell me which receptor should be there Alpha One there's no need to memorize the things make the sense out of it so here are alpha one adrenergic receptors Mi clear now we come down of course under the hair but I'm always sometimes I cannot understand some women make their hair like straight up I don't know what they are either they are doing it to scare someone or just attitude attitude to self-protection right but someone should guide them that they may share some good
things okay so after that here we come down right if you come down their eyes now in the eyes there should be some changes which you which should help you to fight with the stress so let's talk about eyeball and what happens to the structures in eye to under stressful circumstances and how your energy system is operating first of all about the pupil of the eye pupil should construct or dilate dilate what is the advantage of dilating the pupil actually jungle environment the real stresses when someone attacks you in darkness right so evolution in evolution
the response has been maintained that when you are under stress in a dark environment right uh people should dilate so you can absorb more and more light and you can see more clearly for this purpose let's draw your beautiful eye here and there are two types of muscle here these are dilator pupili you know it these are radial muscles these are dilator pupili and here you have yes what are these smooth muscles which are circular these are of course it is not ciliaris how you will study pharmacology if you put ciliaras here I will tell
you later what is this Constructor PPI before you tell me something else this green muscles are Constructor pupili so there is dilator people I and there are Constructor people I right now under stress people should construct or dilate yes it should dilate right and if people should die later yes if people should dilate then just dilator pupili muscle the radial muscle the later people eye muscle should be inhibited or stimulated it should be stimulated because this red dilator people eye if it is stimulated it will pull the pupil out open right so on this on
the dilator people eye the receptor should be stimulatory or inhibitory stimulatory which receptor should be there Alpha One is that right so no need to memorize again so there are alpha one adrenergic receptor present on dilator oh sorry dilator pupili and when dilator people I are stimulated people will dilate is that right people will dilate there is some interesting physiological phenomena related with pupil dilation uh do you know that sometimes some clever woman intelligent woman there they put some substances to keep their pupil dilated why you know in models also you know this thing or
not not interested in models right why they try to keep the pupil dilated another question why women like candlelight dinner why it is romantic yes it is romantic but why every woman knows so good to have dinner with someone in Candlelight but why Candlelight why not under flashlight dinner yeah because pupil dilate it means dilation of people has something to do with romance isn't it right now he says so that people looks bigger but what what it will give a message to you if your girl has a relative people what message will come to you
let me tell you let me tell you manner visual right men are stimulated by the visual stimuli coming from the female right that is why they work so hard on makeup and other things now what really happens that during ejaculation or during orgasm parasympathetic nervous system fire or sympathetic fires it's Dr Rose is saying parasympathetic you will kill the man you know listen parasympathetic erection parasympathetic activity in maleous Direction and female it is secretions right it is sympathetic activity the real sexual actors parasympathetic activity followed by intense sympathetic outflow erection in the male is parasympathetic
female gets wet it is parasympathetic when there is an intense sympathetic stimulation male gets ejaculation female gets orgasm of course at that time pupil dialect is that right now you can make some sense right and in ancient times some women were so much desperate to impress the males that they are so much interested in the male and their people are dilated they were putting in their eyes a drop of Belladonna Belladonna that will dilate the pupil but the mechanism of a Tropa Bella Donna will discuss in some other lecture right that the layers of people
so what women do they put the drops of a Tropa Belladonna there right and that is why galadona mean beautiful woman beautiful woman was using a Tropa a trophy Belladonna a drop of a beautiful woman right so this is a very common thing that women when they are going to see their male whom they love they put some a tropical Belladonna there and people will dilate and male will feel somewhere in their message coming to their unconscious mind that she is so much happy with me right and the real situation is this that after putting
a Tropa Belladonna ciliaris muscle is paralyzed and male looks very blurred [Laughter] I don't know that may help some women to tolerate the situation right am I clear to you no problem into this right so let's come back so dilated people for the candlelight is a good thing dilated pupil for model women's to model for the fashion shows they put something to dilate that is good right so what I want you to remember that sympathetic nervous system dilates of your blood right and darkness and stress and even at intense sexual experience now let's move forward
and even in fear people dilate you know intense fear people dilate now we'll move forward what about ciliaris muscle what happens to celiers when you are under intense stress dog is after you is that right dog is after you you are under intense stress sympathetic nervous system is firing not only people should dilate but there should be one more change in the eyeball the next change in the eyeball is that you will you are supposed to focus the lens for near VN or far Vian when you are under stress you want to run away you
should focus for near VN or farvian farvian is that right so under stress and sympathetic overflow lens should be lens of the eye should be commutating for far Vian so length should be thin should be thick globular or thin lens should be globular or lung lens should be in a position or lens should be in B position it should be like this for far VM because if lens become globular if lens become globular then it is focused for near VN if lens become flattened it is focused for Varian so it means sympathetic nervous system intense
stimulation should focus the eyes for far VM so that you can really look far and run away where to run away right the thing is that how it really happens how lenses flattened this is the function of ciliaris muscle so let me tell you where is cilia so next time you do not say that Constructor people is siliaras so you should know where is silly Addison how the ciliaris work right so let me draw a diagram here this is your eyeball and here is your beautiful cornea right and here is your pupil your pupil here
now you already know that muscle here is Constructor pupili please don't confuse this with siliaras ciliaris muscle is present over here yeah ciliaris muscle is present over here now this is your lens here is your lens and these are the which ligaments suspensory ligaments of Zone yields right these are the suspensory ligaments or called zonule here is your lens now first you understand muscle work every most of the muscles when they contract they have one fixed Point another mobile end right for example when I'm Contracting biceps this is the fixed point and this point is
moving the bones is that right in the same way celerus has one fixed point ciliaris is fixed over here an interior part ciliaris is present here like a circle right it is circular muscle but in section it is looking this is anterior end of the ciliaris and this is posterior end of the ciliaris and ciliara cells fixated in the interior end and its posterior end is mobile the posterior end of the ciliarasis mobile now listen carefully when siliera's contract when ciliaris will contract posterior end will move forward and inward when sileros will contract this interior
end cannot move so posterior end when ciliaris muscle will contract and get shortened it will move forward and inward from both sides so when filaris is contracted its position becomes like this it is shortened it is shortened muscle and this posterior end is here and here suppose contacted muscle has this position and relaxed muscle as just position relaxed muscle position we can say it is a dash a and contracted muscle position is B Dash B now listen whenever ciliaris muscle will contract right uh these points where suspensory ligaments are attached they will move forward and
inward and tension on the lens will become more or less tension will become less let me explain look once siliaris is contracted right these are the points where posterior end will move right now the distance between B and B has become less but whenever ciliaris relaxes posterior and move backward and outward so whenever celiers relaxes there's more distance between a and a and that stretches the suspensory ligament so this mechanism is very important whenever ciliaras relaxes posterior and move backward and outward and stretch the suspensory ligament and when they stretch the suspensory ligament lens become
flattened and whenever ciliaris is Contracting and it moves forward and inward right distance between the ends of the ciliaras become less and suspensely ligament become loose and lens become yes globular lens become globular so in this position lands it like this right but whenever it contract suspensely ligament become loose is that right when suspensary ligament become loose lens become globular am I clear and whenever lens is globular you are focusing for near VN whenever lens is flattened you are focusing for VM now under the stress when sympathetic nervous system is firing you are under stress
as I gave you example dog is after you it is midnight and you are running right you have to focus for near Vienna for VN you have to focus for far View and to look where are the options to run away to focus for farvian you need lens globular or lens flattened and if you want lens flat end you need celeras contracted or you want ciliaras relaxed and if you want ciliaris relax ciliaras should have stimulatory receptors or inhibitory receptors should have inhibitory receptor and you remember the basic principle is all the tissue to be
inhibited have beta2 except few so which receptor should be there on ciliaris beta2 that's so simple it's very logical so ciliaris muscle should have beta2 adrenergic this chapter and now today you understand how the ciliaras work so now under stress and sympathetic overflow your hair will stand up pupil will dilate ciliaris will relax you will accommodate for far VN and now you come down other changes in the body let's come to now your oral cavity and we talk about changes in your git what are the changes now in your gastrointestinal system under what and that
sympathetic overflow right let's draw the part of gastrointestinal system and we have to see that what changes will be there now in the git there are two types of smooth muscles there are longitudinal smooth muscles and there are foreign you know there's pyloric Center and you must be knowing there's ileocecal sphincter and some of you may be knowing there is anal sphincter so these filters are there in git isn't it uh and let's suppose here I draw the longitudinal muscles actually circular muscles and longitudinal muscles are present throughout longitudinal muscles are mainly responsible for peristalsis
longitude of muscles are mainly responsible to initiate the peristalsis then circular also participate in peristalsis will not go into that detail I just want to know one thing that when dog is after you you are under stress the circular smooth muscles in the sphincter should relax or contract relax you want that you will throw something and horrify the dog very bad it's unfair with the dog dogs have human rights also don't throw things like that under stress it's not the time I mean right so Splinter should contract or relax anal sphincter should be tight under
stress even though sometimes autonomic nervous system under stress dysfunction and you pass urine out of something else right it more often happens in the baby that's a dysfunction of nervous system normally in a fully developed mature autonomic nervous system under stress sprinkles should tighten up no one should know what's going on isn't it not even dog so of course during when dog is after you or you are under stress git is not going to help you to fight with the dog so this tissue should be inhibited its activity should be inhibited to inhibit the all
activity in the git there are multiple steps first of all sprinkles should tighten up right if sphincters are tightened up so this is inhibited or stimulated they're stimulated the smooth muscle that stimulated and if this smooth muscles are stimulated there should be stimulatory receptors or inhibitory receptors stimulatory so which receptor should be there Alpha One hydrologic receptors that's great so the Alpha One adrenergic receptors arms sphincters not no no problem to remember it and what about these longer muscles longitudinal muscles longitudinal muscles responsible to initiate the peristalsis under stress you want more peristalsis or you
can digest things later on and absorb later on yeah so this muscle should be stimulated or inhabited inhabited and which receptors should be there stimulatory or inhibitory inhibitory and which receptor should be there do you think you need to really memorize it it all makes logic beta 2 and reject receptors right now we come to the blood supply to git right suppose this is the your general circulation and this is a mesenteric artery coming to git right to give the blood supply to git I cut it here and here is yes here is your blood
vessel going to git and of course this blood vessel should have smooth muscles in it s media isn't it am I right now do you think under stress you need more blood supply to git or less less because you have to see save blood from git and diverted maybe to the muscles which can help you to fight with the dog or fly away from the dog is that right so you want more blood supply coming to git and less less because if there's less blood supply there will be less secretions of less absorption we can
do these things later digestion and absorption of the chicken peas as I told you previously first we have to save our own leg piece from the dog so what really happens we have to reduce the blood supply to git to reduce the blood supply to the git smooth muscles in the media should constrict or relax they should construct if they should construct they should be stimulated or inhabited they are stimulated which receptors should be there I don't know why as people try to memorize it Alpha One adrenergic receptor it's so logical and the git in
the sphincters they should be Alpha One right in the git other muscles they can be beta too on the git blood flow mesenteric vessels they should be Alpha One they should construct under stress no problem clear color okay this was something about git and in the same way when blood supply to G8 is reduced secretions will be also reduced because glands need blood supply to produce their secretions that is why under stress your mouth become dry you know when you're under stress your mouth become dry because saliva becomes less blood vessels like slavery glands have
constructed there's no fun in explaining it anymore is that clear okay uh so we have seen the hairs will stand up pupil will dilate eyes will accommodate for far VN right and git mortality will be reduced thank God sphincters will be tightened up and blood flow through JT will be reduced to diverted to skeletal muscle any question up to here then we go down GID we have discussed let's come here there are lungs in the heart you want to discuss sympathetic activity in the lungs first or the heart first it's up to you hard first
but which comes first coming down lungs we do lungs first and then go to the sympathetic activity on the cardiovascular system so let's talk about respiratory system what are the changes and the respiratory system under sympathetic overflow one thing is very simple when sympathetic overflow is within the central nervous system that will stimulate the respiratory Center and respiratory rate will be increased this is one thing secondly Hajj when dog is after you when you are under stress you need more oxygen or less oxygen you need more oxygen right and if you need more oxygen and
you will be producing more carbon dioxide so you need to remove look now the circulatory system you have to provide more oxygen and you have to remove more carbon dioxide which is being produced when you're running in front of the dog right so in the stressor stressful circumstances we need more oxy gases going to the lungs is that right for this purpose what do you think bronchioles should constrict or dilate dilate let's see I will make a section of this part of the broncular tree I will make a section here here this is a suppose
bronchial and we wanted to open under stress so that more oxygen can be coming now let's talk about what is really there you know that there are smooth muscles in the bronchioles there are smooth muscles in the bronchial am I clear and what do you think this smooth broncular smooth muscle they should construct others should dilate so they should be stimulated or relaxed inhibited they should be inhibited and if bronchial or smooth muscle should be inhibited so that bronchial Lumen open up and more gases are coming under stress so when they are inhibited they should
have stimulatory receptors inhibitory receptor so which receptors should be there smooth muscle has beta2 receptors there's no trick in that which are two adrenergic receptors bronchial smooth muscle that which are two adrenergic receptors when these receptors are stimulated bronchioles dilate that is why in patients with asthma we give the drugs which can stimulate beta2 receptors so that beta 2 mediated bronchodilation should be seen there am I clear no problem into this now we go to your beautiful heart that what happens to your cardiovascular system righteous okay Mr Ronald has come up with the question what
about the blood vessels which are present in the bronchial mucosa and submucosa and although that area let me explain I was thinking maybe I can get away but my students are so intelligent they ask the question so let me explain it to him I was just wondering to get away without explaining but you are very clever right so here is let's suppose your smooth muscle what is this this is your smooth muscle bronchiller already we discussed we want to relax the smooth muscle we want to open the Lumen we want to open the Lumen if
we want to open the lumal Lumen one way is relaxing the smooth muscles so Nature has provided beta2 adrenergic receptor on these there are blood vessels also here there are blood vessels also here we call them what are what are these vessels yeah what type of vessels are these are the pulmonary vessels the bronchial blood vessels is a bronchial blood vessels now these blood vessels which are present in bronchial system right of course these blood vessels also have their smooth muscle here is the right they have smooth muscle in the wall now uh to increase
the Lumen here you want to shrink the mucosa and some mucosars you should look if we increase the blood flow here if we increase the blood flow here then it will this area will become animators and hyperemic and this area will swell up and Lumen will be reduced but under stress you want to reduce the Lumen of bronchial tree or increase the lumen if you want to increase the Lumen there are two ways number one dilate the bronchial smooth muscle number two reduce the blood supply there because if you these blood vessels constrict bronchial blood
vessels construct blood flow to this area becomes less when blood flows this area becomes less this area is less hyperemic there's less blood flow the less secretions right area become dry and and lining of the bronchial channels become thin shrunkan is that right and Lumen will become white so we need to dilate these blood vessels or constrict these blood vessels yes we need to construct if you need to construct these blood vessels then smooth muscles in this Blood these blood vessels should be stimulated or inhibited stimulated smooth muscle will be stimulated and then it will
construct so there should be stimulatory receptors are inhibitory so which receptors should be there for one alternative reasons it's so simple the bronchial smooth muscles bronchial smoothness receptor but bronchial blood vessels most muscle has Alpha One adrenergic receptors no problem up to this now we come and talk about the cardiovascular distribution right let's talk about the heart first your beautiful heart here are your Atria and here are your ventricles right and of the heart you know that there are there what is this here [Applause] what's present over here SA node and what's present over here
AV node and what is this this bundle of hairs heavy node bundle of hairs and bundle branches and then parkinjay fibers there's no problem up to this perfectly okay now let's see what is the action of the sympathetic nervous system in the heart first of all we should know that under stressful circumstances heart should be stimulated or inhibited we need more cardiac output or less cardiac output we need more cardiac output you know cardiac output is equal to yes please is equal to stroke volume into heart rate is that right we want to increase stroke
volume when you are running in front of the dog and stressful circumstances and you're fighting you need a good cardiac output going to your skeletal muscles right so you to increase the cardiac output of course heart rate should be increased heart rate and into increase stroke volume stroke volume means the volume which is ejected by The ventricle during one pump right the that stroke volume depends on contractility mainly how well it contract now what really happens we have to stimulate the heart so first principle is there should be stimulatory receptor on heart mainly or inhibitory
receptors stimulatory receptors and which stimulatory Alpha One or beta1 yes beta 1 because we said all the tissues to be stimulated should have Alpha One except heart juxtagomerular operators and adipocytes adipocytes right so heart does has stimulatory but not Alpha One it mainly has beta 1 receptors so receptors here should be yes on SA node the beta 1 receptors right beta1 adrenergic receptor and on AV node also just a minute on AV node also there are beta 1 receptors system also there are beta 1 receptors and of course on the atrial muscle and ventricular muscle
that also beta1 adrenergic receptor so heart is well decorated by beta1 receptors so we were talking about that what is the effect of adrenergic system on the heart as we know heart should be stimulated so heart should have stimulatory receptors right either Alpha One or beta 1 but as you know all the tissue to be stimulated have Alpha One except hard Global operators and adipose cells so heart is one of the exception right so it has beta1 adrenergic receptors dominantly right so beta 100 receptors are present on the SA node AV node and on the
packages system moreover they are present on the editorial contractile myocardium and ventricular contractile myocardium now what is the effect of this on the heart when snode is stimulated what is the normal function of acetone asinode is responsible for cardiac Auto maticity how do you define automaticity automaticity is a property of a tissue to produce depolarizations spontaneously because asinode produces depolarization spontaneously it is normally the pacemaker of the heart when it is stimulated by the adrenergic norepinephrine or epinephrine acting on the beta-1 receptor pacemaker activity will increase right so heart rate will increase so there is
increased heart rate due to action here and increase heart rate is called positive chronotropic action Chrono tropic action chronotropy mean here chronotropy mean related with the normal automaticity normal automaticity so when normal automaticity of the heart is increased we say there is positive chronotropy number one number two there is also stimulation of what is this AV node when AV node is stimulated the conduction through AV naught become fast the impulses are conducted fastly from the Atria to The ventricle so we can say under the influence of adrenergic Drive adrenergist stimulation avino's conduction velocity increases and
when conduction velocity in AV node and this conduction system increases we say there is positive yes please there is positive dromotropic action this is called yes when conduction through AV node is increased we say there is positive dromo tropic action of their drug or action of the neurotransmitter or action of the hormone right how do you remember that it should be called dromotropic I always think that AV node is like a small drum between the nutrient ventricle so whenever drugs stimulate this drum there is a positive dromotropic action is that right no problem into this
then we can come to the action on the myocardium right but before we really go for that when there's positive chronotropic action plus there is positive dromotropic action both of these action lead to increase heart rate so this component is achieved by increasing by positive yes chronotropic and by positive dromo drum now we come to action on the myocardium which contracts right editorial myocardium and ventricular myocardium this myocardium has also beta1 receptors and this is also stimulated and when they are stimulated their action is contractility and with even they will special when especially when ventricular
myocardium will contract strongly when ventricular myocardial contract strongly of course that will produce more stroke volume is it right when it contracts strongly so increase contractility is called yes increase contractility is called positive I know Tropi I know Tropic action positive ionotropic action or positive ionotropy and this Factor lead to increase stroke volume so we can say when epinephrine or on catecholamines or epinephrine and norepinephrine act on the heart the increase heart rate increase the conduction through the conduction system especially every node and increase the contractuality right and the heart rate is increased and stroke
volume is increased due to increased contractility is increased cardiac output is there any question here there's no question and of course whenever cardiac output is increased systolic blood pressure goes up you know that or not we'll discuss blood pressure changes in detail when I will teach you the drugs right drugs mean catecholamines not other drugs so we were talking about the effect of sympathetic nervous system on cardiovascular system we have already discussed the effect on heart right and now we'll talk about the effect of sympathetic nervous system on the vascular system right so let's suppose
this is your gender circulation right from this General circulation the blood supply is going to Let's suppose skin here is your git right then blood supply is also going to the kidney right and of course your beloved skeletal muscle which is going to help you to fight with the stressful circumstances blood supply is going there and blood supply is of course going to yes central nervous system so we can say that blood vessels this is blood vessel going to skin so cutaneous blood flow this is mesenteric blood flow this is your renal blood flow and
this is blood flow to skeletal muscle is that right and of course here is the blood flow too central nervous system and here is blood flow too heart coronary system now we have to see what happens to all these vascular beds under sympathetic activation right again as we discussed that sympathetic nervous system is adjusting the tissues and organ in such a way that body should be more appropriately prepared to fight or flight the stress right now under stressful circumstances as that horrible dog is after you right we have to change change the blood flow in
different tissues what do you think blood flow to the skin should be increased or decreased it pardon it is decreased or increased people who believe blood flow to the skin should be decreased they should raise their hand okay people who believe blood flow to the skin should be increased they should raise their hand okay so you think you are going to blush off the blush there for the dog look blood flow to the skin should be decreased because of blood flow to the skin is increased you blush the air and blood your dog is not
going to take it and another thing if blood flow under the stress increase to the skin and if dog really bite there will be more bleeding so I'm just very stressful circumstances blood flow to the skin decreases people don't become red people become pale under fear is that right or not so blood flow to the skin should be decreasing and there are advantages when cutaneous blood flow decrease the blood which is saved can be diverted to the muscle secondly reduce blood flow to the skin is good so that if some damage to the skin occur
there should be less bleeding right of course under some circumstances blood flow to the cheeks and some areas increases those circumstances are really not that that is not that dog is after you that is some sort of romantic stress you know uh when you blush isn't that there was a time woman used to blush and skin will become red right that is for different thing I think more evolutionary that is telling to the man we have good hemoglobin we can have a baby and everything right I don't know what but anyway women blush it makes
them more beautiful more appealing is that right but these days if they don't blast no problem they blush on isn't that it works still am I right so a blushing is not really that life-threatening stress right that is some more emotional situation for which Nature has provided different neuronal connections that so that you can appropriately blush right but under real stress blood flow to the skin goes less and when you don't actually really blushing is when you are embarrassed sweetly embarrassed right but this is stressful circumstances dog is after you or some examinar is asking
you very tough questions and planning to throw you out and you feel like this you don't blush them then you pale isn't it so blood vessels to skin should constrict or dilate construct so smooth muscle of these blood vessels smooth muscle around these blood vessels should be stimulated or inhibited so which of the separate should be there Alpha One so cutaneous vessel that Alpha One adrenergic receptors right then already we have discussed blood flow to the git that should be increased or decreased yeah that should be decreased that is not the time to increase the
blood flow and to the git we should save the blood from the git and divert to the muscle so smooth muscles to dehyd vasculature smooth muscle in the mesenteric arteries should constrict or relax it should construct you know you want more blood flow less if you want less it should vasoconstrictor vasodilate it should Reserve constructs or smooth muscle should be stimulated or inhabited stimulated which receptors should be there Alpha One right adrenergic receptor what about renal blood flow you should increase blood flow to kidney or decrease blood flow to kidney right decrease blood flow to
the kidney as I told you previously you can make urine later right uh more appropriate when you are relaxed but right now you constrict the renal vessels so that blood can be diverted to the muscles is that right so for here there should be this smooth muscle should be again stimulated or inhibited so which receptor should be there Alpha One adrenergic receptor remember some people under stress pass out urine that is not kidney function that is a autonomic dysfunction precipitated under stress to the urinary bladder normally urinary bladder under stress should hold the urine it
doesn't help to pass out the urine under stress is that right that's the dysfunction Anyway come back what about skeletal muscles blood flow you want more blood flow to skeletal muscles or less more so blood vessels so skeletal muscle should construct or dilate so you need to stimulate the smooth muscles or relax so you should have stimulated scepter inhibitory which one should be there beta200 receptors so this is action of what adrenergic system sympathetic nervous system on your cardiovascular system and of course we should not forget blood flow to the brain and heart itself cerebral
blood flow should increase or decrease when you're under stress you should increase so that blood vessels dilate and produce severe headache do you think it's good when cerebral vessels dilate use precipitate headache did you know that or not all the drugs which dilate the vessels to produce headache right why let me explain and then I will say suppose this is your central nervous system here happily there these are the blood vessels going to your central nervous system right under four they are passing through these foramina these are the foramen isn't it and in these foramina
right uh you must be knowing that Dura matters there is dura metal lining Dural sleeve come here they know that the blood vessels which are entering or leaving the central nervous system in the Dural sleeve the durometer here there are very high concentration of pain receptors what are receptors here pain receptors so whenever these blood vessels dilate too much they hammer on the the dilate with every pulse the dilate and hammer on the pain receptors on Dural sleeve and you feel throbbing headache headache with every pulse isn't it so dilating vessels too much to cerebral
system is really not good thing under stress because you will have headache so what should happen to the cerebral blood vessels and if the construct you will simply with ischemia fall down you know what I'm trying to tell you blood flow to central nervous system is so important to the nature it is not left at the mercy of autonomic fluctuation this you should remember blood flow to the central nervous system is so important it is auto regulated by the central nervous system it is not left at the mercy of autonomic fluctuations Amic layer so cerebral
blood vessels do not have any significant concentration of adrenergic receptors cerebral blood vessels do not have any significant concentration of what adrenergic receptors so sympathetic fluctuations don't control cerebral blood flow cerebral blood flow is auto regulated by the metabolites produced by the brain and central nervous system is working more it produce more metabolite with dilate the cerebral vessels and some part of central nervous system which is not working much that will produce less metabolite and there will be less dilation of the cerebral vessels so I hope you'll remember it thank you for remembering it what
about coronary blood flow that should increase during the stressful circumstances are decrease that should increase so which receptor should be there alpha 1 or beta2 I'm talking about not the I'm talking about the adrenergic receptors on coronary blood vessels there should be Alpha One or beta2 either there should be none or both should be equal in number you know why coronary blood flow is again so important it should not be left at the mercy of autonomic fluctuation coronary vessel diameter is mainly regulated by the Auto regulation by the myocardial products and myocardium needs more blood
flow it produces the metabolites we dilate the coronary vessels in their branches like cerebral system coronary blood vessels are not left at the mercy of autonomic fluctuations thank God isn't it otherwise you see a girl you get tachycardia sympathetic nervous system is up and then you say oh I get myocardial infarction by the age of 30 maybe we get 40 myocardial infarctions that is not good so the blood vessels the coronary blood vessels to the heart are not left at the mercy of autonomic fluctuation and the most funny thing these blood vessels coronary blood vessels
do have adrenergic receptor but the concentration of adrenergic receptors Alpha One hydrologic receptors and beta2000 receptors are same so whenever epinephrine goes there alpha 1 receptors try to construct and beta2 receptor try to dilate so there is no significant effect but maybe in Prince metal and China you know Prince metal in China visas plastic disease of the coronary vessel probably the multiple mechanism one of the mechanism is The beta2 receptors may be less than Alpha One receptors will be inherited more we will not talk about that here to learn that in pathology what I really
wanted to tell you that cerebral circulation a cerebral vasculature and coronary vasculature again it's worth repeating is not left at the mercy of autonomic fluctuations by the nature these two vasculature have either very few adrenergic receptors and if they do have adrenergic receptors then stimulatory Alpha One hydrogenergic receptors and inhibitory beta two adenosis receptors are in same concentration am I clear any problem here no now let's move forward and learn more about the action of adrenergic drugs or adrenergic system or sympathetic nervous system on other tissues up to now what we have learned you are
under stress right so your hair stand up your pupil dilate right your mouth is dry your heart your bronchial yes these are dilated and your heart is stimulated Amorite it is stimulated increase heart rate and Vascular blood flow is also altered is that right and now we should come to some other tissues and about git we have also discussed what will be changes in the git now we'll talk about where what you want to discuss we can talk about metabolic changes in the body or you want to talk about zero genital changes in the body
under stress yeah it's your choice okay I leave tries to uh doctor Sergio Maori you want to discuss what first you want metabolic changes you shy away you know from the changes in the genital system I don't know why but we'll come to that also okay he want to know that what are the metabolic changes in the body when sympathetic nervous system is really working well right okay let's talk about few changes here is your circulatory system right here is your liver one of the very important metabolic organ and of course there must be what
is this fat cell adipocyte right and there must be muscle also skeletal muscle right first of all under stress you know one of the very important function of the liver is one of the very important function of the liver is take the glucose and convert the glucose into yes glycogen whenever you are in well-fed state and you are in welfare state you have eaten a lot glucose is going to your liver and liver cells are taking of the glucose and making the glycogen and storing the glucose do you think under stress you need to store
glucose as glycogen do you need to do you think understands stress you must do glycogenesis no glycogenesis should stop rather glycogen should break down into glucose and glucose should come to the blood am I right so glycogenesis should be inhibited so there should be stimulatory receptor inhibitory receptors so there are inhibitory receptors and which receptors should be there beta2 adrenergic receptors so liver cells of beta-2 adrenergic receptors which give inhibitory signals uh stop the glyco Genesis and that releases automatically the pathway for the breakdown of glycogen and there is glycogenolysis going on and glycogen breakdown
and glucose is coming to the blood so under stress liver is releasing what glucose to the blood so that glucose supply to the muscles and to the brain should be more under stress this is one thing secondly you know best form in which energy is stored in the body is triglycerides one glycerol with Three fatty acids in the adipocyte am I right the adipocyte there are triglycerides now do you think there is a muscle here right which will break down the triglyceride it's not muscle of course this is enzyme here this is triglyceride and there
is an enzyme here and this enzyme when it is activated this enzyme will break down the triglyceride and release free fatty acids and glycerol isn't it now and of course these free fatty acids are a very good source of energy directly plus this free fatty acid can go into liver and in the liver from fatty acid we can make glucose this pathway is called gluco neogenesis formation of glucose from new sources like formation of glucose from amino acids the formation of glucose from fatty acids right so it means the appropriate metabolic change in the body
under stress should be that there should be lipolysis there should be breakdown of the leopard there should be lipolysis and increase free fatty acid level in the blood with that there should be yes please gluconeogenesis so that fatty acids convert into glucose am I really clear so do you think this breakdown of lipids and this lipase this should be stimulated or inhabited stimulated so which the separate should be there stimulatory or inhibitory stimulatory receptors and stimulatory receptor here is yes it is it cannot be alpha one because this is an exception so it is beta1
actually it is really not beta1 it is modified beta1 and modified beta1 these days is called beta 3 adrenergic receptor immaculate no problem in understanding this right so free fatty acids are coming and going there so liver as an organ releasing the glucose it is releasing the glucose by breakdown of glycogen right which is called glyco genolysis and it is also releasing glucose by gluconeogenesis right trying to mean look at the dog how much changes he has induced in your body isn't it now so your blood glucose level will go up and blood free fatty
acid level is also going up and now let's go to the skeletal muscle in the skeletal muscle in the skeletal muscle you know skeletal muscle also store glucose as glycogen do they have glycogen or not okay that's very good thank you for knowing it that skeletal muscle also take glucose to glycogen do you think this process should be stimulated or inhabited inhabited because skeletal muscle are under more action and if skeletal muscles are under more action they need glucose they don't need to store glucose as glycogen they need to break the glycogen back to glucose
so this process that glucose should be converted into glycogen should be stimulated or inhibited and habited so which receptors should be here beta2 very good beta2 adrenergic receptors are present on the skeletal muscle cells and that inhibits the glycogen formation and activate the glycogen breakdown so that within the skeletal muscle more glucose is available as energy for Contracting and running away from the dog right and of course another thing that when a skeletal muscles are having a lot of action depolarization repolarization you know there is electrical activity followed by mechanical activity when you are having
lot of contractions are running away from the dog your skeletal muscles new cell bodies are undergoing depolar Action potentials followed by contractions so when there are action potentials going on let's suppose this is one skeletal muscle fiber cell repeatedly action potential going on during every action potential sodium goes yes and sodium and flux produces depolarization right there's sodium influx and there is loss of during depolarization sodium goes in during repolarization potassium comes out so actually when muscle are Contracting too much what is really happening during every depolarization more sodium is going into skeletal muscle and
every repolarization which follows depolarization potassium loss is there and this imbalance is corrected by what is this sodium potassium 80 Pages which would whatever sodium has gone in they will throw that sodium out and whatever potassium has escaped out that will go in those are right now you tell me something that this process that potassium is being lost during contractions potassium is being lost it should be stopped or it should be accelerated you want to lose more potassium we should bring this potassium back should we bring back or not you know if you are running
and sodium is going in and potassium is getting lost this potassium should be brought back is it important or not if too much potassium is lost cell membranes become so electronegative that there's hyperpolarization and muscle cannot be stimulated do you think that should happen so somehow we should not allow the cell to lose its reserve of what potassium so what really happens that again there are beta2 receptors here right these beta2 receptors gives signals intracellular multiple signals which eventually lead to phosphorylation of sodium potassium they bring the changes into sodium potassium 80 phase and it
work more is very important point when you are losing gaining sodium or losing potassium balance is corrected by whom who correct the balance sodium potassium 80 pays so sodium potassium 80 pages should be stimulated and if you need to stimulate them what will happen they will throw the sodium out and they will take the potassium n so what really happens in sympathetic overflow sodium potassium 80 phases in the skeletal muscle cells are activated and skeletal muscles start taking up the potassium from the blood is that right this is another metabolic change you will learn the
significance of this phenomenon later on that in some diseases we give beta2 stimulant drug the diseases in which muscles lose excessive potassium right now in this case actually receptors are beta2 not stimulatory but inhibitory receptors are beta2 so beta2 receptors are stimulated right and here this is an exceptional situation they give intracellular signals which stimulate sodium potassium 80 phases so in rapidly Contracting muscles and muscles undergoing rapid Action potentials right keep on correcting their ionic balance I think you could not understand it clearly there should be inhibitories I understand what's going wrong with your mind
actually listen life is you can live a good life with general principles but you will come across situations where there are exceptions there are exceptions this is exception actually your mind is working so that if we have to activate sodium potassium it pays then we should have stimulatory receptor rare here Nature has played a track it is using the same receptor to breaking down the glucose from glycogen same receptor gives signals and alter that right so actually here receptor is not stimulatory it is still inhibitory but intracellular signals are going to stimulate the sodium potassium
80 phase this is one Exceptions there are other exceptions also but you don't want to talk about them right now yes you know lysis listen generally what happened the enzymes which are converting glucose into glycogen whenever those enzymes are inhibited then enzymes breaking down the glycogen are released from inhibit reaction they are activated because until glucose Supply is good and glycogen synthetases are working more then glycogen breaking enzymes are automatically inhibited but whenever you inhibit the process of glucose to glycogen then this enzymatic Pathways inhibited towards this side these enzymes which are bringing glycogen to
glucose they are released right yeah it doesn't it does not Now we move forward in a nutshell what we can say then the skeletal muscle not only blood flow is increasing to skeletal muscle rather skeletal muscles start breaking down glycogen to glucose plus skeletal muscle is also taking up the potassium from the blood is that right when you are exercising too much Now we move forward as a general what are the metabolic changes in the body under adrenergic stress metabolic changes are that glucose level in the blood will go up Three fatty acid level and
the blood will go up potassium level will eventually go down this is the right and glycogen the muscle will also break down into glucose am I clear there's any problem there's no now we move forward okay I would love to mention one more thing you know in the muscle skeletal muscle there are intrafusal fibers and extra fusel fibers extra futile fibers are the fibers which contract and introfusal fibers are like muscle spindles you know that these muscles spindle they are responsible to maintain the balance and sensitivity of this contractile operators these are also having beta2
receptors and that inhibits the function of muscle spindles listen carefully if I'm keep keeping my hands steady then there's a muscle tone on Agonist and antagonist and that tone is equal on agonic flexor then extensors are equal tone and I'm keeping my hand steady the tone is maintained well with the help of muscle spindles muscle spindle adjust the sensitivity of the contraction of muscles now when adrenergic activity become too much and beta2 receptors are stimulated on muscle spindles muscles spindle become inhibited and dysfunctional then they become dysfunctional you cannot maintain flexor and extensor tone equal
so sometimes Flex extensor tone become more sometimes flexor tone become more than you correct it by so they start undergoing tremors so that is why under sympathetic overflow or under fear or under anger you have Tremors or even when you are having some drugs which are beta2 stimulant like solvitable in Albuterol these drugs also produce tremors am I really clear right any question after this now we have discussed this and if Dr Sergio Maori allows us we can talk about the sympathetic action on urogenital system yes doctor should we discuss okay thank you for granting
information right so uh you want me to discuss male gentle system first or female no no I'll leave the choice with Dr Sergio Maori that's action of autonomic nervous system ladies first always I never knew he was such a good taste Okay so we should make a uterus there because you cannot imagine a woman without uterus isn't it okay I will use the different color right so here we have uterus of a lady and of course vagina and now we have to see what is the action of autonomic nervous system on the this Euro this
part of the eurogenital system first of all you must know that ladies have smooth muscles here in the myometrium you know myometrium right foreign first of all about the myomaterial smooth muscle my material smooth muscle should contract or they should have stimulatory receptors or inhibitory receptor when they have sympathetic overflow and female has a sympathetic overflow and remember during orgasm there is an intense sympathetic overflow female should have in the myometrium ah stimulatory receptors are inhibitory receptor no one want to talk about it it is still taboo yeah stimulatory right a why is female should
have stimulatory receptors on myometrium because during the orgasm you just should have little contraction to take up the semen the right to facilitate upward movement of the sperms right now uh according to your theory there should be stimulatory receptors and which stimulatory receptors should be there my friend okay you want to have alpha 1 receptors over there and if alpha 1 adrenergic receptors are present over there your thinking is that that whenever female will have orgasms uterus will contract may be violently and take up the some material up so this makes some sense but there
is one problem eventually the result is female will become pregnant sooner or later and once you become pregnant and pregnant women you know they become angry very soon one of the very important reason is men are unfortunately not really you know when female pregnancy advances and they start looking around right so she's angry and if a pregnant woman undergoes anger burst and uterus contract this beautiful baby will come out and threaten to come out before time do you think it's a good news right it's a very bad news do you think if you trust Contra
every time a pregnant female undergo stress and uterus contracts right is the good news no female is a wonderful organism she is responsible to maintain our speeches right baby should be upside down I think you don't know about exceptions right Okay so yeah you are worried about baby I'm worried about women right so we are talking about we are talking about that you want to have a uterus which has a lot of Alpha One receptors on myometrium and whenever she gets angry uterus contract and babies products of conceptions are scented threatened to come out do
you think it's a good situation no so which receptors should be there so that whenever women get angry sympathetic overflow occur uterus at least relax and her baby should not suffer so you think now another theory has come from another person and the theory is this that we should have inhibitory receptor and inhibitory receptor will be beta2 adrenergic receptor right now let me tell you the beauty of the nature right the beauty of the nature is as you know female are very clever what they do they express those receptors which they really need female who
is not pregnant actually in the nucleus of the this myometrical cell there are Gene for Alpha receptor as well as Gene for beta2 receptor when female is not pregnant and estrogen progesterone changes the cyclical right during her monthly Cycles then alpha 1 receptors are expressing and she is making more alpha 1 receptors and less beta-2 reporter so in non-pregnant geotras even the alpha 1 and beta2 receptors both are present in the Miriam but the dominant receptors are Alpha One so that uterus can contract appropriately and enhances the probability of pregnancy conception is that right but
when female becomes pregnant you know the female behavior before pregnancy and after pregnancy is different many of the wise men know that because her behavior is appropriate for sufficient perpetuation before pregnancies female behavior is to get the right man right and after pregnancy is once she is pregnant her main concern is your pregnancy should go smoothly uneventfully and she should become a great mother that is how they are designed by the nature not only psychologically but even at the uterus level right so what really happened when they are not pregnant Alpha One receptors are the
dominant receptors expressed on the my material smooth muscle but when females become pregnant hormones change you know extreme progesterone level become high and they are no more cyclical that signal goes and changes the genomic expression in my material cell they switch off the Alpha One receptor genes and activate the genes for beta2 receptors and pregnant females uterus has more beta-2 receptors than miamito cell than Alpha One receptor Mi clear so that whenever she gets angry it does not threaten the baby am I right and this thing this all why I explained so much because it
has some clinical relevance my friend the relevance is that when there is female is threatening to undergo premature labor now sometimes they they have premature contraction and there's premature labor right for example just on 25th week or 27th week you just start Contracting as a doctor you would like to increase the contractions of uterus or you want to relax the uterus and inhibit the contractions relax and which receptor is there to relax as uterus so which drug should be given drug deal which is better to stimulant actually there's a drug called rightodrine which is beta2
receptor Agonist so females who threaten to not female female deuters which threatens to start labor prematurely one of the treatment is you give the female injection of right or drain ritodeine will go and stimulate yes which are two receptors on Mayo material cells and beta2 inhibit mediated relaxation of my material cell will occur and premature contractions will stop am I clear no problem up to this so this was something about the uterus about the secretions in vagina I will not go into detail except that uh male erection and female secretions in vagina both are functionally
and neurologically operated in the same way then male get excited or stimulated sexually they develop erection in their organ when female get stimulated or excited sexually they produce more secretions in their both these mechanisms in male and female are stimulated by parasympathetic nervous system they are stimulated by parasympathetic nervous system but in male ejaculation and in female orgasm is mainly mediated by sympathetic nervous system and for sympathetic nervous system we'll talk later in detail when we talk about the male urogenital system so this was something about the uterus and vaginal secretions and we have to
talk about urinary bladder also isn't it there what about urinary bladder okay here you have I think I should remove this it is disturbing your attention now will make a urinary bladder and we'll see what really happens to yeah it's beta2 delivery is operated by different mechanism uh females don't deliver the baby due to sympathetic activation there were different mechanisms oxytocinism release we'll discuss it in Guinea of one day right now we have to make a this is urinary bladder right and now in urinary bladder there are muscles here these muscles of urinary bladder are
called detruser do you know that or not user and of course there is oh my god there should be internal urethral sphincter also very very important foreign here is your your internal urethral surfender right now this is your internal urethral sphincter and this is your right now we have to talk about two things number one when you are under stress and dog is after you or any big thing what do you think you want to pass during or you want to retain during while you're running it's not really very appropriate to pass the urine so
if you want to hold your urine uh what do you think the truth or should contract or relax relax of course the truth or should relax and sphinct Richard contract it means the trousal muscle should be inhibited and Splinter muscle should be stimulated am I right so when you detruser should be relaxed so that it does not push the urine forward so there should be stimulatory receptors here are inhibitory inhibitory which inhibitory will be there yeah there are beta2 so actually if the truth or have which are true adrenergic receptors but during stressful circumstances sphincter
should be tight so if symmetry should be stimulated or inhibited and it should be stimulated then stimulatory receptor or inhibitory receptor stimulatory receptor which one should be there Alpha One I don't know how you know it so well now there are alpha one adrenergic receptor right so it's very easy to understand that in the urinary bladder has Alpha One receptor so that when you are under stress detruser should relax and sphincter should contract but of course there are examples when someone understands passes the urine out or she passes urine out specially in children that is
a this function of autonomic nervous system immacula sometimes autonomic nervous system also gets confused right and loser contract and spend to relax an unfortunate situation develop right so this was something about what neurogenital system about the male urogenital system uh I told you ejaculation is yes sympathetic mediated right so during ejaculation the smooth muscles and the prostate and vast difference and other areas because they have to ejaculate the semen those smooth muscle should contractor relax they should contract if those muscle has to contract in the male genital system then those smooth muscles should have stimulator
receptors or inhibitory receptors stimulator receptor which stimulatory receptors should be there yes Alpha One there's no problem so there's no fun in remembering that prostate has Alpha One receptor prostate has Alpha One receptor logically it should have Alpha One hydrologic receptor because prostate smooth muscle the was different smooth muscle need to contract to expel the male uh you can say semen so there should be Alpha One receptors over there that is why men are really not very happy with Alpha One blocker drugs there's no need to explain it you understand why they are not happy
with Alpha One blocking drug that's good so Ronald understand that and now the last thing which I should not forget I told you that all the tissues to be stimulated have Alpha for one receptors except heart which have beta1 juxta glomerular operators and adipocyte I did not discuss extra glomerular operators let's talk about that isn't it and in the kidney one kidney has how many extra glomerular operators actually with every nephron there is one juxta glomerular operators so this is one Nephron right and you must be knowing that this is your what is this afferent
arterial some smooth muscle from my front arterial and some special cells from here macular densa with some other cells called laser cell all of these together make this operators which is called juxta glomerular operators major function of juxtagomerular operators is to release what they release renin and you must be knowing that renin will go into blood convert angiotensinogen into Angiotensin 1 which will pass through the pulmonary capillary and exposed to pulmonary capillary endothelium which will have enzyme Angiotensin converting enzyme which will convert Angiotensin 1 into angiotensin two and Angiotensin 2 will lead to vasoconstriction plus
Angiotensin 2 will lead to the release of aldosterone which will lead to the retention of salt and water so do you think when you are under stress for example dog is after you you want to take your blood pressure up or down up so it means angiotensin two should be more it means eventually renin should be more secondly under stress you should retain salt and water because interesting stress in Jungle life there are chances you will get damage and you may bleed so you have to start retaining salt and water to keep your volume protected
in future right so aldosterone has to be more so under stressful circumstances uh renin should be released more so that eventually vessels should constrict under the influence of Angiotensin too and kidney retains salt and water under the influence of Elder stay around so ran in just a glomerular operators should be inhibited or stimulated stimulated so stimulatory receptors inhibitory receptors which stimulatory receptors beat our not alpha one I told you all the tissues to be stimulated should have Alpha One except hard juxtapur operators and adipocyte so there are beta 1 adrenergic receptor present over there I'm
just talking about a lot of operators again it's important to remember why sometimes as anti-hypertensive drug you may take Propranolol or you may take Atenolol they block the beta-1 receptor here and reduce the renin output and they have many other actions also we'll talk that later when we study the drugs is there any question no class dismiss thank you
Related Videos
3:56:09
Adrenergic Drugs Part 2 | Pharmacology | D...
Dr. Najeeb Lectures
163,341 views
2:43:06
Cholinergic Drugs | Pharmacology | Dr Najeeb
Dr. Najeeb Lectures
303,781 views

1:45:41
Autonomic Pharmacology | Adrenergic Agonists
Ninja Nerd
346,101 views

1:05:39
Sympathomimetics (Adrenergic Agonists)—Epi...
Medicosis Perfectionalis
65,972 views

3:49:35
Antihypertensive Drugs | Pharmacology | Dr...
Dr. Najeeb Lectures
512,867 views
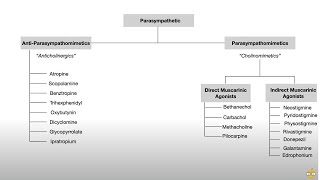
33:57
Autonomic Nervous System (Pharmacology, Re...
Dirty Medicine
661,385 views
1:57:49
AntiCholinergic Drugs | Parasympatholytic ...
Dr. Najeeb Lectures
118,940 views

1:59:15
Autonomic Pharmacology | Adrenergic Antago...
Ninja Nerd
184,446 views

10:08
'Trump Will Invade Europe': Jeffrey Sachs'...
moneycontrol
594 views
10:20
Adrenergic Receptors - CHEAT SHEET!
Dr Matt & Dr Mike
394,202 views
1:12:23
Normal Blood Glucose | Hyperglycemia | Hyp...
Dr. Najeeb Lectures
256,756 views

8:48
"Heart of Compassion" for Palestine: Pope ...
Democracy Now!
6,127 views

17:51
Pharmacology - ADRENERGIC RECEPTORS & AGON...
Speed Pharmacology
2,246,654 views

4:31:14
Antianginal Drugs Pharmacology | Dr Najeeb🩺
Dr. Najeeb Lectures
114,387 views

32:46
Pharmacology | Autonomic Nervous System | ...
Mental Dental
236,434 views

1:05:50
Neurology | Adrenergic Receptors
Ninja Nerd
517,628 views

3:03:35
Diuretics | Pharmacology | Dr Najeeb
Dr. Najeeb Lectures
1,158,216 views

12:40
'Israel Doesn't Want Peace': Jeffrey Sachs...
Times Of India
138,885 views
55:49
Diabetic Ketoacidosis | Symptoms | Causes ...
Dr. Najeeb Lectures
105,796 views
3:51:05
Penicillin | Antibiotics | Mechanism of Ac...
Dr. Najeeb Lectures
153,561 views