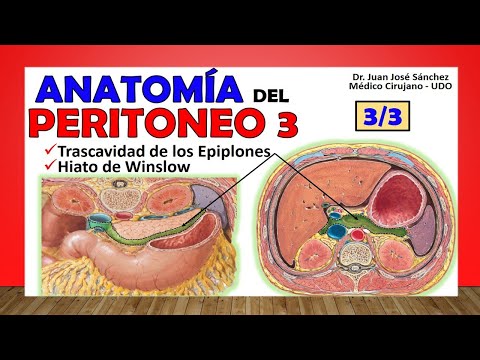
🥇 PERITONEO 3/3. Trascavidad de los Epiplones, Bolsa Omental.
79.63k views2178 WordsCopy TextShare
Anatomía Fácil por Juan José Sánchez
En la version vieja del Latarjet Testut aparece como "Trascavidad", pero en las versiones mas nuevas...
Video Transcript:
Good dear listeners of anatomy, today I bring you the latest installment of peritoneum, we have already seen peritoneum 1 where we talk about the generalities, the divisions, we have already seen the video of peritoneum 2, the video of peritoneum 2 where we address the large peritonial cavity and well, now With this we will talk about the small peritonial cavity as the famous after cavity of the omentum or omental bag is called and to this topic we will dedicate this video of peritoneum 3, reminding you that at the end of this video it is imperative, important that you watch the video of retroperitoneum and so on. finish learning this topic of peritoneum. When we talk about the after epiploic cavity it is important to recognize that it is one of the cavities into which the peritonial cavity is subdivided, there is what we call the small peritonial cavity or also called omental bag or omental bag, the famous after cavity of the oments or after the cavity of the omentum, what I point out here in green in this cross section is the great peritonial cavity, what I pointed out here in blue I am pointing out precisely the parietal peritoneum, which is what separates me from that great peritoneal cavity.
famous retroperitoneum, notice that very closely related to the large abdominal cavity we find this cavity that is in blue that is in front of the retroperitoneum which is then that after cavity of the omentums, seeing it in a lateral section here we would now see the peritoneum in black parietal separating me in front of the great peritoneal cavity, behind that parietal peritoneum to the retroperitoneum and a subdivision of that great peritoneal cavity is the after cavity of the omentums that here in this section, let's say sagittal, we can see it very well marked, notice that it is a somewhat long cavity, somewhat long for what is generally believed. We begin by first talking about the limits of that after cavity of the omentum and we take advantage of this same sagittal image a little closer to talk first about the anterior limit, the anterior limit will be given first by the lesser omentum, both ligaments that make up the lesser omentum , that is, both the hepatoduodenal ligament and the hepatogastric ligament, then we go or continue descending and we find the posterior face of the stomach, remember that this posterior face of the stomach would be covered by a thin membrane of visceral peritoneum, that would be then part of the anterior wall of that after epiploic cavity and then if we do not go further towards the right side we find, says the text, two to three centimeters of the first portion of the duodenum, that is also how it is already located, the side of the stomach is really a continuation of the stomach and would also be part of the anterior limit, if we continue descending notice that the lowest part of that anterior limit will be the posterior face of the anterior leaf of the greater omentum, remember that the greater omentum was actually formed by an anterior leaf, a posterior leaf and the anterior leaf was subdivided into two, into an anterior portion and a posterior portion, specifically that posterior portion of the anterior leaf of that greater omentum is what forms the anterior limit of that after cavity of the omentums, seeing it in this cross section, look there we would have the posterior face of the stomach, remember that all this space of the transcavity of the omentum, we go laterally and find the lesser omentum with its two ligaments as the anterior limit and if we go down a small part in the first portion of the duodenum, so that all this that you see here behind all this that the stomach would be the after cavity the pillars, even remember that this which is the greater omentum is also part of that anterior limit because this is a cavity that curves forward, anyway in this image see how we cut the greater omentum to see well the anterior limit of the stomach, first portion of the duodenum, part of it and this which would be the anterior sheet of the greater omentum that is just cut, see everything this would also be part of the previous limit. We are then going to continue talking about other biological cavities, naming their posterior limit but before they do not go away from the video [Music] I invite you to subscribe here in the lower right corner click [Music] and don't forget to like the video; Subscribe to the channel so you can have access to all its content, we already have almost every abdomen ready, right now we are going to get into retroperitoneum, you will find more than 160 videos on the channel just by subscribing below where you get the red notification .
We then continue talking now about the posterior limit of this second cavity of the omentum and well here we are seeing the second splenic cavity, so here we sort of grab the anterior limit and cut it, we practically lift it with a clamp, everything that we see behind is practically the posterior limit of this cavity, notice, upwards we say that the thoracoabdominal diaphragm that portion that would be the vertebral portion also called lumbar portion would form the beginning of that posterior limit obviously it is the parietal peritoneum that covers these structures as such because in itself the after cavity It does not have any communication with the diaphragm because it passes through the parietal peritoneum. You can see how it is shiny there because they are covering it, also downwards, well, the pancreas, almost in its entirety, is one of the most important organs that are in the back . of this after the omentum cavity.
Then we find the left adrenal gland along with the upper pole of the left kidney, we also find the posterior part of the first portion of the duodenum and we also find the transverse mesocolon and the transverse colon itself, so notice that this duodenum like it is practically in The most antero-superior part of this after cavity of the omentum is part of both the upper postero limit and the anterior limit, so down here we continued with the transverse colon, the transverse mesocolon and here the two leaves of the greater omentum can be seen very well, This leaf would be the one we cut, which is the anterior leaf, and this one that we see over here that I am putting in green would be the posterior leaf, so specifically the anterior face or let's say the anterior part of the posterior leaf of the greater omentum would form the posterior limit. From this after cavity of the pilons, the anterior and posterior leaf generally fuse and this cavity closes, in the fetus it is a little more open but more or less as far as that after cavity of the omentums would reach, generally it is not that You can put your hand between the two omentums because most of the time this part here is sealed, it is practically already closed, if we see it from here we can see how the posterior limit here is only seen in the pancreas, specifically the parietal peritoneum that is covering the pancreas. Now, how do I enter the after cavity of the omentum?
Well, there is an opening that communicates with the large peritoneal cavity, specifically this portion here, which is the hepatorenal portion that we talked about, the hepatorenal bag, sorry that we talked about in the previous video, also called the right subhepatic space, so this part of the large abdominal cavity. It communicates or through it you enter the after cavity of the omentums through a hole that I put here in yellow, that famous hole receives a name, a very used eponym that is the winslow hiatus, just as you see it. Here described in the sheet that the theory says that I can grab two fingers and pass them through the winslow hiatus and in that way I enter the second cavity of the omentum, then that winslow hiatus which is a hole will have some boundaries; will have an anterior limit that will be given by a part of the lesser omentum, specifically the hepatoduodenal ligament, reminding you that within the hepatoduodenal ligament there is the portal triad, there is the hepatic pedicle, that is, it would be the anterior limit of that winslow hiatus, both in the portal vein, the common bile duct and the hepatic artery itself, all surrounded by the hepatoduodenal ligament that is part of the lesser omentum and forming the anterior limit of the entrance to that after cavity of the omentum.
Then as a posterior limit, see clearly, there we see the inferior vena cava limiting posteriorly, generally these two walls are attached, the anterior and posterior ones, and the vena cava is very attached to the lesser omentum, not that this is completely closed, the opening exists but when your vision is a corpse you see that these two cavities, these two walls are practically glued together and in fact that is how anatomical texts also write them . As the lower limit we are going to have the upper edge of the first portion of the duodenum, the lower limit of that Winslow hiatus, notice here how you see the anterior limit, the posterior limit, here you would see the lower limit with the duodenum, here too you see the anterior limit, there you see the posterior, here you see the inferior; He took advantage of this to show them the upper limit which is the famous spiegel lobe of the liver that we describe in the liver video, this spiegel lobe also called the caudate lobe, in fact it is said that it extends towards the cavity of the omentum and We are going to see it now in a lateral view, see this axis behind the cavity, see how the caudate lobe, which is Spiegel's, projects towards the cavity, forming the upper limit of that orifice that you see there, which is the Winslow hiatus, so Here you can see the anterior limit because you can see the portal vein, the middle hepatic artery is seen and there you can see that this would be the portal triad, the hepatoduodenal ligament, the posterior limit is not seen there, we cannot see it because it is The inferior vena cava is covered by the abdominal aorta and in the middle you can see the first portion of the duodenum, forming the lower limit of that Winslow hiatus. Now moving to the omental cavity itself, we find that it is formed by two large recesses; a superior recess which is the place where that spiegel lobe is, by the way it is smaller and goes behind the liver until it reaches the noa area of the liver, in fact what limits it above practically is that part of the coronary ligament here as It is seen from the liver, that would be from the superior recess of the after epiploic cavity and then we have the part larger than the inferior recess, here I show you the relationship that the superior recess has with that caudate lobe and in that inferior recess we see that it is mainly related to the posterior part of the stomach and the posterior part of the lesser omentum, they also describe two ligaments that are found from the posterior wall of this cavity forward, which are the famous gastro-pancreatic ligaments, a right gastro-pancreatic ligament formed by the common hepatic artery that goes to the right and downwards, we are going to see it better now in an image and here a ligament of the left gastro-pancreatic that would be formed by the left gastric artery also called coronary stomatal artery, when we see it like this we see here In the right fold by the hepatic proper and the fold that would be the left gastro-pancreatic ligament formed by the stomatal coronary artery also called gastric artery, there is also an extension of this lower recess which is the famous splenic recess which is nothing more than the place that is looking towards the spleen, that is, in the most lateral and left portion of this after epiploic cavity or more specifically the inferior recess of the after epiploic cavity, seen in this section more or less this would be the inferior recess as well as you They would be seeing it there in that way the splenic recess.
Related Videos

12:36
🥇 Anatomy of the RETROPERITONEUM. (Limits...
Anatomía Fácil por Juan José Sánchez
86,296 views
23:30
🥇 PERITONEUM 1/3. Generalities and Divisi...
Anatomía Fácil por Juan José Sánchez
255,358 views

20:47
Examen físico de abdomen COMPLETO | Semiol...
Facultad de Ciencias Médicas UNR
4,305,511 views
9:03
PERITONEO 4
leonardo coscarelli
253,994 views

19:25
🥇 PERITONEUM 2/3. Omentum, Mesos, Ligamen...
Anatomía Fácil por Juan José Sánchez
124,506 views

13:56
The Brain
Bozeman Science
5,833,907 views
16:00
🥇 Anatomy of the GALLBLADDER and THE BILI...
Anatomía Fácil por Juan José Sánchez
273,795 views
35:23
🥇 Anatomy of the ABDOMINAL AORTA. Easy Ex...
Anatomía Fácil por Juan José Sánchez
200,053 views

19:39
🥇 Anatomy of the STOMACH. Easy, Quick and...
Anatomía Fácil por Juan José Sánchez
293,178 views

15:28
Hiatus hernia anatomy
Sam Webster
3,238,415 views

18:36
🥇 PELVIC DIAPHRAGM. PELVIC FLOOR. -Muscles-
Anatomía Fácil por Juan José Sánchez
221,081 views

13:21
🥇 ARTERIES OF THE ABDOMINAL WALL. (Irriga...
Anatomía Fácil por Juan José Sánchez
81,622 views

26:39
Anatomía - Hígado (Configuración Externa, ...
Dr. Carlos Andrés García
190,308 views

17:45
🥇 Anatomy of THE URETERS. Easy Explanation!
Anatomía Fácil por Juan José Sánchez
120,067 views

9:04
🔴 ANATOMIA👉 EPIPLONES 🟩 PERITONEO 🟪
Hablemos de Anatomia y Algo Mas...
8,121 views

7:58
PERITONEO 2
leonardo coscarelli
346,693 views

17:35
Anatomía del Abdomen - Peritoneo y Cavidad...
Medizi
23,265 views

18:37
🥇 Anatomy of the DUODENUM. Easy, Quick an...
Anatomía Fácil por Juan José Sánchez
246,661 views

23:51
Lymphatic System
Siebert Science
302,887 views

20:16
🥇 ANATOMY OF THE PHARYNX 1/2, (Muscles, I...
Anatomía Fácil por Juan José Sánchez
204,726 views