🥇 PERITONEO 1/3. Generalidades y Divisiones. ¡Fácil de Entender!
255.34k views3815 WordsCopy TextShare
Anatomía Fácil por Juan José Sánchez
Descarga esta y cualquier diapositiva de mi canal, uniéndote a PATREON!
También puedes unirte a los ...
Video Transcript:
Hello! How are you, nice to greet you. Welcome to a new video on this channel, Easy Anatomy, by Juan José Sánchez.
Today I bring you a video that has been requested a lot. It's a video that, honestly, I had shied away from because of how long and complicated it was to approach. However, I decided to divide it into three parts as long as it is.
Yes, today we will talk exactly about the anatomy of the peritoneum. I remind you then that it is comprised of three videos and then a fourth video in which we will address a cavity or a space that is closely related to the peritoneum, which is the retroperitoneum. So, practically this would be the fourth video of this peritoneum installment.
This is your channel, Easy Anatomy, by Juan José Sanz. We begin by first talking about the generalities of the peritoneum so that you understand it roughly and what its major divisions are. Let's start by first talking about the fact that the peritoneum is a serous membrane.
There are three large serous membranes that are in the body that are the famous 3 Ps: the pleura, the peritoneum and the pericardium. The 2 or 3 serous membranes are very similar in themselves since they form a bilayer, that is, they are two layers that continue one with another. So, this serous membrane, called peritoneum, is the one that is primarily responsible for enveloping the structures found inside the abdomen.
In fact, you cut an abdomen and when you start to see the organs like that with that shiny cap, since all the organs have a kind of brilliance, it is because the membrane that is covering it is the peritoneum. Simply, the peritoneum covers the entire abdomen and retracts into the abdomen. For example, you see this cut here and you see that a membrane comes that covers the entire abdominal wall and then folds over the organs and covers the organs and covers the organ again and then turns around and continues covering the organ.
All that is the peritoneum. Now, classically it is written that the peritoneum is made up of two sheets. We talk first about a parietal sheet, which is what we call parietal peritoneum, here similar to the pleura and the pericardium, that is, parietal means in anatomy that it goes towards the walls.
So, notice here that this part of the pleura of the peritoneum is sculpted, they surround this piece, so to speak, the entire abdominal wall from the inside, the entire abdominal wall, everything you see here in blue is the parietal peritoneum. While when this membrane, instead of covering the walls of the abdomen, when this membrane stops covering them and begins to lay on top and now cover the viscera of the organs that are contained within the abdomen, it becomes visceral peritoneum, But they are not two isolated entities, they are one on top of the other, notice that the visceral peritoneum, for example, here is surrounding the liver and then here it begins to surround the stomach, here, for example, it begins to surround the vessel, which is why the visceral peritoneum is the sheet or layer of the peritoneum that surrounds the viscera or the organs and is what will make them shiny, while the parietal peritoneum is what would then wrap or cover the walls, but notice here that for example this is still parietal but when it retracts it becomes visceral, then it is the same parietal that when it retracts over an organ it becomes visceral, then this visceral, see, goes all the way around, all the way around, all the way around and here it folds back in and becomes to become parietal it continues to be parietal, parietal again visceral, visceral, visceral turns everything around, it is like a chain, it is a continuity and then the visceral will become parietal again, if we see it here from the side For example, here we see in blue the entire parietal peritoneum surrounding the diaphragm in the muscles on the wall of the abdomen. Down here it has a limit surrounding the pelvic structures but above them, that is why the pelvic structures are not considered structures that are inside the peritoneum because they are excluded by it and then here again it begins to stick to the posterior abdominal wall, that is why that would be, the parietal peritoneum would be the blue one, Now when it folds back, for example, over the liver, the stomach, the transverse colon, these are the loops of the small intestine.
Notice that when it folds over those houses it becomes visceral peritoneum, so the difference between the visceral and the parietal is that one surrounds the wall and the other is surrounding the viscera, the organs as such. In this classic cut of the anterior abdominal wall, what interests me is that you see the different layers that I have to cut in the abdomen to reach the large peritoneal cavity, first I cut the skin underneath, below the skin the subcutaneous cellular tissue, then the muscles first the external oblique, then the internal oblique, then the transversus abdominis, once I cut the transversus abdominis I find a very particular fascia called transversalis fascia, behind the transversalis fascia I find a little yellowish tissue because it is more or less fatty, it is called extra peritoneal connective tissue, it is more or less similar to the endothoracic fascia that the thorax has, more or less like this, the extra peritonial connective tissue and then from the extra peritoneal connective tissue is what I The encounter with the parietal peritoneum is that once I cut the parietal peritoneum I can access the abdomen, so these are the different layers of the abdominal wall until we reach the parietal peritoneum. If we see it more or less live, see more or less here You can't see the skin, you can't see the subcutaneous cellular tissue but we see the external oblique, we see the internal oblique, we see the transversus abdominis, then deep to it the transversalis fascia, then the tissue that I told you is more or less like adipose like fat, which is the extra-peritoneral connective tissue, and then after we find the parietal peritoneum, once I cut this parietal peritoneum, I access the large abdominal cavity.
Let's continue talking about the generalities of peritoneum but first don't get away from this video [Music] I invite you to subscribe here in the lower right corner click [Music] and don't forget to like the videos, it's important then Subscribe to the channel below where you see that it says subscribe automatically, click and you are subscribed to the channel. We already have more than 56 thousand subscribers, more than 160 anatomical videos on the channel, all thorax, abdomen, neck or bones of the skull, upper limb, below and if there are videos that you can't find here, well, simply write to me on the channel and comment on this video so I can make the video you are requesting. Now, this superior view is of the large abdominal cavity or the large peritoneal cavity as they want to call it, of a woman I know it is a woman because we see the fallopian tubes, the ovaries, the uterus and with this I want to tell you that the sac abdominal, that is, the abdominal cavity in women is not closed because through the fallopian tubes it reaches the uterus, which reaches the vagina and thus can be communicated to the outside, in fact you infiltrate air, for example into the uterine cavity to perform certain tests that are not relevant and the air will reach the abdominal cavity, in men this is the vision of a man, notice that we do not see the uterus but only the rectum and the bladder, the man is a A little simpler in that part, the pelvic portion in men is completely closed in the abdominal cavity because there is no communication with the outside, this is a difference between one and the other.
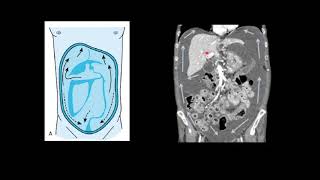
Let's talk then about the compartments of the large peritoneal cavity, which is what generally confuses students, look at all this that I 'm marking here in black is the parietal peritoneum, notice attached to the posterior abdominal wall, posterior wall, here at the diaphragm, the anterior abdominal wall, means that everything that is inside that parietal peritoneum is the so-called large peritonial cavity or they also call it the greater cavity or simply the large abdominal cavity but it turns out that within that abdominal cavity there is a smaller cavity that It would be the trans cavity or after cavity, excuse me. Here it is not trans with N, but after the omentum cavity, also called the bursa. omental or omental sac, this cavity is quite important, in fact it is a subdivision of the large abdominal cavity and that is why it is sometimes called even the minor peritoneal cavity, the large peritoneal cavity which is the green one is called the large cavity or the greater cavity, while it is behind the cavity of the omentums, they generally call it the lesser cavity or the small cavity, it is important to study it so much that I dedicate the third part of the peritoneum videos to it, in the first two videos we will talk about the great peritoneal cavity because you see that it is large, it deserves to talk about it, in the third video we will talk about it after the omentum cavity and finally there is a space that is behind that parietal peritoneum, that is, it is between the parietal peritoneum that is in the back part of the abdomen and then let's call it the musculature and the bone part of the back of the abdomen, so this space that is behind this parietal peritoneum that I am putting here in yellow is the famous retroperitoneum, the The same name tells you is the space that is behind the peritoneum, it is not considered part of the large abdominal cavity and there I dedicated a separate video to it, which is the retroperitoneum video that is also uploaded to the channel along with these, which have to See it in order peritoneum 1 2 3 and then retroperitoneum so that you can perfectly understand what retroperitoneum corresponds to.
For example, this is a cross section that we already saw right now, what you see in blue is the posterior parietal peritoneum, I tell you that because everything that is behind it that I am putting here in green is the famous retroperitoneum , which is a space virtual, this is really a virtual space where we find the pancreas, the kidneys, many viscera that we are going to see later in the retroperitoneum video, everything that is in front of that parietal peritoneum within the large abdominal cavity is the large peritoneal load and Remember that inside the large peritoneal cavity there is a smaller sub-cavity which is the after cavity of the omentums, which well you will understand later, here what I want you to know is: how they exist or what the compartments that form the peritoneum are like, these They are the big three. Let's stay with this image for example, this entire membrane that we see here as it is attached to the posterior abdominal wall, that is what you see there transparently in the background, that retroperitoneum in fact everything you see here in the background is the retroperitoneum: kidneys, pancreas, ureters second, third and fourth portion of the duodenum, the abdominal aorta, the inferior vena cava, all are considered retroperitoneal organs or viscera because they lie behind that parietal peritoneum. Seen here now, let's talk, let's stay with the large peritoneal cavity, which is what we will dedicate these first two videos to, this large peritoneal cavity is subdivided again, what structures subdivide them?
First, what I am pointing out here is called transverse mesocolon, which is a fold of visceral peritoneum. It is another important thing every time you see a strange fold that has nothing to do with or is not the wall itself, that is visceral peritoneum, so This thing that attaches to the transverse colon is transverse mesocolon, this structure together with the transverse colon along with another structure of the peritoneum called the greater omentum or greater omentum, these three structures subdivide me in the large peritoneal cavity in a space that is above it called supra mesocolic compartment or space, see above the mesocolon and the transverse colon, which is why it receives that name, it is a superior antero space, while all the space that remains below that dividing structure is the infra mesocolic cavity or space , which would be more postero inferior, the supra mesocolic is more antero superior and the infra mesocolic is more antero posterior or inferior sorry. Well, let's first see the supra mesocolic compartment , this is all of this, notice all this, the transverse mesocolon comes here, this is the transverse colon, so everything that is above it in the supra mesocolic space will be formed first .
for the subphrenic spaces, phrenic means diaphragm, subphrenic which is below the diaphragm, then we would have the right subphrenic space and the left subphrenic space that starts from the left. I put them here in blue, this right subphrenic space will be limited posteriorly by this ligament that you see there, which is the coronary ligament. , superiorly by the diaphragm, anteriorly we find the abdominal wall, anteriorly we also find the anterior abdominal wall and the diaphragm limit the right lateral while the left lateral limit see that I am shading them in green, we are talking about the right subphrenic space is the falciform ligament of the liver, while the left here we see that the right lateral limit in this case of the left subphrenic space of the falciform ligament of the upper limit remains the diaphragm, the posterior the final part of the coronary ligament already when the ligament becomes left triangular, the anterior limit is the same, the same anterior abdominal wall and we see it here in green to the right subphrenic and see the left subphrenic as the left lateral part is quite related to the organ of the spleen, the splenic organ that I also uploaded recently a video of him on the channel, these are the first two subdivisions of the supra mesocolic space: the right sub phrenic space and the left sub phrenic space, but we also have an infra hepatic space, this infra hepatic space, obviously it would be just on the side and It is very frequently known as the hepatorenal bursa.
Its anterior limit is going to be the visceral surface of the right lobe of the liver. What happens is that here it looks superior because the liver is grabbed with a clamp, a hook, but when you let go of it This is anterior, the posterior limit is seen in the right kidney, the limit let's say that it goes further up in the lower part of the coronary ligament and its limit on the left side is going to be the entrance to the after quality of the omentums, which is the famous Winslow hiatus, which is this place where it is passing, let's say this little wire here, this level, this is the left lateral limit of that space and this would be the supra mesocolic space, let's now go to the supra mesocolic space, to study it we have to first , here would be the transverse colon, this would be the greater omentum, we lift the greater omentum, see the transverse colon, back here the structure that supports the transverse colon, which is the transverse mesocolon, then all that remains below is the space or cavity infra mesocolic that the entire small intestine is located there, rather not all but the jejunum and the ileum specifically. Now that infra mesocolic space is crossed obliquely by the root or by the mesentery itself, really, it is by the root plus the complete mesentery, then it would be divided into two spaces: one that would be superior and straight, which is the space, listen well mesenterico colic What does menenteric colic mean?
which is between the mesentery and the colon then it would be the right colic mesenteric space and this would be the left colic mesenteric space which would be more than the entire space on the left side, now this left colic mesenteric space, important because the see has almost direct communication With the pelvic cavity as such, then any liquid that enters here is infectious, any substance will end up reaching the pelvic cavity, which will not happen so easily if this occurs in the right colic mesenteric. Now, in addition to being colic mesenteric spaces, we would also have the colic parietocolic spaces, see, wall parieto and colonic colic, then this would be the space or they also call it the right parietocolic slide and this would be the left parietocolic space or slide, the same thing happens as the The left pariertocolic space drains directly into the pelvic cavity. These are then the large subdivisions of the large peritoneal cavity.
We are going to talk about some minor folds or fossae that we find here at the peritoneal level, they are found in relation to the duodenum, in relation to the final part of the ileum and in relation to the sigmoid colon, Let's start first with what It is in relation to the duodenum, notice that there is a fold that is the paraduodenal fold, which is the duodenum. Here you see the third portion, here the fourth portion, which is the ascending one, so this paraduodenal fold is formed by the inferior mesenteric vein as is seen there and the left colic artery which is a branch of the inferior mesenteric artery, then we would have the superior duodenal fold which the theory says is caused or originated by a branch or the ascending branch of the left colic artery and then we would have the inferior duodenal fold which is simply a fold that comes from the third portion of the duodenum towards that paraduodenal fold, that left me a large fossa, that large fossa that I left is the paraduodenal fossa, these fossa are important because it is a place where you can accumulate fluid, now that paraduodenal fossa also leaves the entrance to one that is upwards behind the upper duodenal fold which would be the pit, this fossa is also called recess, then it would be the pit or upper duodenal recess, there would also be one downwards that It is the inferior duodenal fossa or recess. We also find a fossa that would be between the mesentery and the walls of, let's say, the posterior parietal peritoneum, which would be the parietal mesenteric fossa, which we find very frequently in the Netter book, which names it several times in several images.
We now go with those that are related to the ileum and the cecum, notice that here we have the fold and ileocecal which is a fold that connects the final part of the lion with the base of the appendix, towards the upper part we find a fossa or recess that It is the superior iliocecal fossa or recess, it is said that this fossa is below the fold of the anterior cecal artery, which is actually a fold of mesentery that comes from the mesentery to the anterior part of the cecum and through there it passes to the anterior cecal artery. In the lower part, below that ileocecal fold, a fossa is formed that would be the inferior iliocecal fossa. Now if we go in relation to the cecum, which would be this, we would have the cecal folds.
Notice there, all of this would be the cecal folds and it would be formed . a large fossa behind the cecum that would be called the retrocecal fossa at this level, the retrocecal fossa, more or less here we put our hand upwards and we can reach that cecal fossa, in relation to the sigmoid colon, notice we find a large fossa which is the intersigmoid fossa , very important because that is where the ureter on the left side runs and that is where we find the bifurcation of the primitive iliac artery into the external iliac artery and the internal iliac artery, this fold is specifically formed by the vertex of this structure which is called sigmoid mesocolon because it is a fold of peritoneum that supports the sigmoid colon, this was a let's say inferior view. Now let's go to a higher view of the pelvic portion because that peritoneum is also seen parietal, it also retracts at the pelvic level and as it unfolds at that level it also forms a fossa, notice, this is a man, this is a space, it is a fossa between the bladder and the rectum which is the bottom of the vesicorectal sac, we generally call the fornix when they are a fold of peritoneum that has a free edge, it is a vesicorectal fornix, on the sides we would have the pararectal fossae and on the sides of The bladder would be the laterovesical canals, everything changes when we see the view from the side, notice this, this would be the vesicorectal fornix between the bladder and the rectum of a man, if it is a woman everything changes, why?
because the uterus is interposed, then this space here as it enters the rectum from behind the uterus from the front is called the rectouterine fornix, well known worldwide as the Douglas fornix, on the sides we would also have the pararectal fossae that would give other spaces that would be between the bladder in front and the uterus behind, which is the vesicouterine cul-de-sac seen from the side, back here we would have the rectouterine which is Douglas's cul-de-sac, see how the parietal peritoneum folds beautifully there and one that will be between the uterus and the bladder that bottom of vesicouterine sac. This was the entire first installment of peritoneum, one of the topics that has been most difficult for me to address because of how difficult it is to explain the content. If you liked the video, don't forget to give it a like, subscribe to the channel, you can also find me on my social networks like Instagram @ juan_sanchez1315.
Related Videos

19:25
🥇 PERITONEUM 2/3. Omentum, Mesos, Ligamen...
Anatomía Fácil por Juan José Sánchez
124,506 views

1:08:24
PIEDRAS EN LA VESÍCULA: síntomas, diagnóst...
Dr. Mijail Tapia
370,963 views
![Exploración de Tórax y Ruidos Respiratorios [ Detallado ]](https://img.youtube.com/vi/zI2fvTLPwpA/mqdefault.jpg)
9:17
Exploración de Tórax y Ruidos Respiratorio...
Departamento de Integración de Ciencias Médicas
110,039 views
13:31
Muscular system - Anatomical terminology f...
Kenhub - Learn Human Anatomy
189,955 views

20:06
Roque Dalton
Secretaría de Proyección Social
6,958 views

12:36
🥇 Anatomy of the RETROPERITONEUM. (Limits...
Anatomía Fácil por Juan José Sánchez
86,290 views
25:05
Anatomía del Abdomen - Pared abdominal (MÚ...
Medizi
46,647 views

7:59
PERITONEO 1
leonardo coscarelli
607,757 views
9:22
🥇 TOPOGRAPHIC DIVISION OF THE ABDOMEN, (A...
Anatomía Fácil por Juan José Sánchez
518,581 views
13:16
🥇 PERITONEUM 3/3. Transcavity of the Omen...
Anatomía Fácil por Juan José Sánchez
79,610 views

8:31
🚩🚩Anatomía y movimiento del diafragma
Movimiento Articular
76,238 views
35:23
🥇 Anatomy of the ABDOMINAL AORTA. Easy Ex...
Anatomía Fácil por Juan José Sánchez
200,058 views

20:45
🥇 HEART Anatomy 1/5 - Generalities, Faces...
Anatomía Fácil por Juan José Sánchez
812,776 views

14:50
🥇 MÚSCULOS DE LA PARED ANTEROLATERAL DEL ...
Anatomía Fácil por Juan José Sánchez
333,507 views

8:18
ZONAS, CUADRANTES O REGIONES DEL ABDOMEN
VITAL SUPPORT SAS
42,692 views
49:43
Anatomía Normal de la Cavidad Peritoneal-TC
Postgrado Radiología UNAH
3,170 views

16:33
🥇 Anatomy of the PLEURA. Easy, Quick and ...
Anatomía Fácil por Juan José Sánchez
219,764 views

19:08
🥇 Anatomy of the YEJUNO-ÍLEON, (Small Int...
Anatomía Fácil por Juan José Sánchez
162,383 views

30:54
🥇 COXAL BONE - ILIACO BONE, Anatomy. Easy...
Anatomía Fácil por Juan José Sánchez
457,971 views

17:35
Anatomía del Abdomen - Peritoneo y Cavidad...
Medizi
23,262 views