An Approach to Erectile Dysfunction
32.64k views2225 WordsCopy TextShare
Strong Medicine
A discussion of the causes and work-up of erectile dysfunction, including an overview of the physiol...
Video Transcript:
hello this is eric strong from stanford university and strong medicine today i'll be discussing an approach to erectile dysfunction consistent with the other videos in this particular series the focus will be on the causes and evaluation of erectile dysfunction not on its treatment per se erectile dysfunction or ed is the consistent or recurrent inability to attain and or maintain penile erection sufficient for sexual satisfaction including satisfactory sexual performance ed is the most common form of sexual dysfunction in men the other forms from which it should be distinguished include low libido which is a decrease in
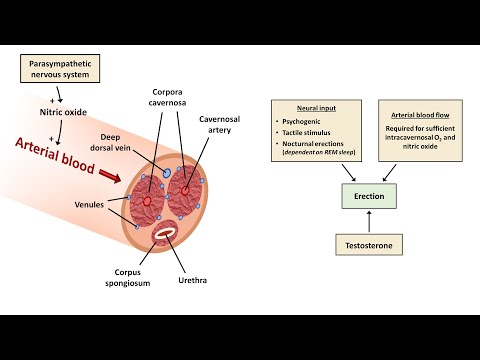
desire or interest in sex in general and premature ejaculation however these different forms of sexual dysfunction can co-exist most commonly ed and low libido to understand the causes of erectile dysfunction it's helpful to understand a little bit about the anatomy and physiology of erections here's a cross-section of the penis inside there are two parallel cylindrical structures on the dorsal side called the corpora cavernosa which consists of an interconnected cavernosa space lined by vascular endothelium and which have the ability to store blood and there is one smaller midline cylindrical structure on the underside called the corpus
spongiosum which contains the urethra when flaccid there is a balance of blood flow directly into the spaces of the corpus cavernosa via cavernosal branches of the internal pudendal artery and blood flow out of the corpus carbernosa via venials or tiny microscopic veins which coalesce into larger veins that eventually drain into the deep dorsal vein when stimulated via the parasympathetic nervous system a local increase in the release of nitric oxide has the downstream effect of relaxing penile vasculature and smooth muscle which dramatically increases the inflow of blood into the corpus cavernosa which increases its size and
rigidity this change in pressure within the penis and its change geometry results in the physical occlusion of the lower pressure venules that normally drain the cavernosa resulting in a positive feedback loop in which more blood accumulates resulting in erection when examining erection from a physiological perspective it requires several things first is neural input of some kind this can be psychogenic as in sexual arousal tactile stimulus of the penis without sexual arousal can also trigger an erection and erections can occur at night during rem sleep each of these three uses different nervous system pathways the second
thing an erection requires is as you might guess arterial blood flow this is required for the sufficient formation of nitric oxide and it's ultimately blood that fills up the cavernosa spaces resulting in an increase in penile size another component contributing to erection is testosterone its role is less than that of the nervous system and blood flow as it's possible for some men to have erections after they've undergone castration by surgical removal of the testes which results in very low levels of circulating testosterone however hypogonadal men with decreased testosterone are at a much higher risk of
erectile dysfunction which in some is correctable with testosterone replacement in summary an abnormality in any of these three general categories the nervous system the blood supply or level of testosterone can lead to erectile dysfunction when it comes to a diagnostic framework for erectile dysfunction diagnoses have been historically classified as organic which includes the three preceding categories versus psychogenic let's discuss some specifics for example neurogenic ed can be caused by spinal cord injury stroke multiple sclerosis and peripheral or autonomic neuropathy vascular causes include anything that causes the pathologic process of atherosclerosis this includes diabetes smoking hypertension
and hyperlipidemia hormonal causes of ed include any form of hypogonadism a term for states of low testosterone hypogonadism can be primary if the issue is within the testes or secondary if the issue is within the hypothalamus of the brain or the pituitary gland an endocrine organ whose hormones control the testes production of testosterone among many other functions the next category is medications each of these meds could be placed into one of the preceding categories but i think it's diagnostically helpful to consider this group separately the most common meds to be associated with ed include antihypertensives
specifically thiazide diuretics like hctz beta blockers and clonidine the aldosterone antagonist spironolactone which is commonly used in heart failure antidepressants particularly ssris and antipsychotics local factors that can cause ed can be subdivided into those of the penis and those of the pelvis penile conditions include peyronie's disease which is a localized connective tissue disease of unknown pathogenesis that results in asymmetric scar tissue within the penis manifesting as a curved penis when erect physical deformity occasionally pain and ed penile fracture is an acutely painful injury in which the covering that envelops the corpus cavernosa is ruptured typically
during forceful sexual intercourse e.d is the long-term consequence of not emergently repairing the injury pelvic factors which can lead to ed include prostate surgery and pelvic radiation last in this category is competitive cycling in which men experience long periods during which pressure is applied by the bicycle seat to the pudendal nerve and internal pudendal artery reducing nerve impulses and blood flow to the penis though the risk from cycling is low enough that it may be outweighed by the cardiovascular benefits in preventing ed the last category is for non-organic or psychogenic etiologies these include performance anxiety
a history of sexual trauma relationship problems with one sexual partner and depression some of these conditions may exist in more than one category as just one example the most prominent impact of diabetes on ed is what's listed here causing atherosclerosis but diabetes may also more directly decrease the levels of nitric oxide within the penis and can cause peripheral and autonomic neuropathy leading to neurogenic ed in addition to the aforementioned categories there are a number of well-established risk factors for ed these include advanced age alcohol and recreational drug use sedentary lifestyle chronic kidney disease and coronary
artery disease of any kind for some of these like alcohol abuse alcohol contributes to the ed and cessation of alcohol use will improve the ed for other risk factors like coronary artery disease it's not that the coronary artery disease is directly causing the ed but rather it's a marker for the presence of a systemic atherosclerosis which is what's causing the ed so not only is cid a risk factor for ed ed is also a risk factor for cad when assessing a patient presenting with erectile dysfunction the history is of paramount importance you want to ask
about the time course specifically the age of onset and its duration the older the patient is when ed begins the more likely it's due to vascular disease also ask about the progression and how rapid the onset was ed with an abrupt onset suggests a medication related or psychogenic cause but could also be seen following a stroke or in multiple sclerosis ask about situational factors meaning does the ed only happen in certain situations for example eddie only occurring went up with a partner but not during masturbation or ed happening while the patient is awake but the
patient still occasionally wakes up from sleep with an erection both of which suggest a psychogenic factor ask about the patient's sexual history including frequency libido presence of relationship problems with the partner and whether there is a history of sexual trauma the presence of low libido accompanying the ed suggests either depression or low testosterone but can also be seen in older age outside of those conditions if possible an interview with the patient's partner with the patient's permission of course can be helpful in identifying psychogenic factors or the presence of other forms of sexual dysfunction which the
patient may be reluctant to discuss themselves which the patient may not even fully appreciate are present a complete gu history including history of prostate surgery pelvic radiation and pelvic trauma given the strong association between ed and vascular disease ask about the patient's past medical history in particular a history of diabetes hypertension hyperlipidemia coronary artery disease and chronic kidney disease take a medication history and a substance use history regarding the focused physical exam after vitals the screen for hypertension and obesity it obviously includes a gu exam focusing on the penile shape and size the presence of
plaques that would be diagnostic of peyronie's disease and testicular size as unusually small testicles would suggest hypogonadism look for peripheral evidence of low testosterone such as gynecomastia which is the enlargement of breast tissue in a male assessed for evidence of systemic atherosclerosis such as feeling the peripheral pulses and looking for cutaneous evidence of peripheral vascular disease and assess the cremasteric reflux this is an example of a superficial reflex in which stroking the inner upper thigh results in a contraction of the ipsilateral scrotum absence of the reflex in a patient with ed suggests the possibility of
a neurogenic etiology notably a rectal exam is not indicated in the evaluation of erectile dysfunction important labs here include a hemoglobin a1c lipid panel and complete metabolic panel to screen for diabetes hyperlipidemia and kidney disease respectively check of testosterone testosterone measurement is a little tricky because the overwhelming majority of testosterone in the blood is bound to a protein called sex hormone binding globulin with a smaller fraction being bound to albumin and a small fraction circulating unbound the common options for testing testosterone include measuring total testosterone which includes all three forms or just the free unbound
form the different options each have their advantages and disadvantages and neither is uniformly preferred over the other but regardless of which of the two testosterone tests are ordered it should be measured in the morning in addition prolactin is occasionally tested but since it typically causes ed by causing hypogonadism it's not necessary to check unless you've identified a low testosterone level one additional test that is occasionally used in the evaluation of ed is nocturnal penile tumescence testing this involves placing a monitor on the penis at night which can measure the number tumescence or girth and rigidity
of nocturnal erections normal npt testing meaning that nocturnal erections are occurring normally is strongly suggestive of a psychogenic etiology of the ed when it comes to a diagnostic algorithm start with a history exam and a testosterone level if the history and exam are diagnostic of local penile disease such as peyronie's disease great the diagnosis is made and you can initiate treatment on some occasions the history and exam will be suggestive of a neurogenic cause which case you should continue with a more focused evaluation depending on which neurological disease is suggested if the testosterone is low
the next step is to measure a serum level of the hormones lh and fsh if these are high the patient has primary hypogonadism or a problem with the testes and the next step would be to determine the patient's karyotype which is an evaluation of their chromosomes for example to see if they have an extra x sex chromosome which can cause low testosterone if on the other hand lh and fsh are either low or normal at the same time that testosterone is low that's diagnostic of secondary hypogonadism which is a problem located in either the pituitary
or hypothalamus the next steps here are to check a prolactin level and consider an mri scan of the cella which is the bony structure at the base of the skull where the pituitary gland is located if the patient is on a potentially constant of medication and if this medication can be safely discontinued or changed to something else do so as a diagnostic test for everyone else or if the trial of holding the med was not helpful consider nocturnal penile tumescence testing if it's available this will not be necessary for all patients for example if the
patient's history is clearly consistent with a psychogenic etiology and if the patient clearly has major vascular disease or other significant chronic medical problems including drug and alcohol abuse npt testing may not be needed either but particularly for the relatively young patient with normal testosterone no cardiovascular risk factors and ambiguous features of the history npt testing can help distinguish organic from occult psychogenic etiologies lastly it's important to remember that ed is a major risk factor for the presence of occult cardiovascular disease therefore in parallel to an evaluation of the ed itself you should also conduct an
evaluation of cardiovascular risk including a metabolic panel hemoglobin a1c and the lipid panel and to treat any identified risk factors accordingly the key takeaway points for this video erectile dysfunction is the consistent or recurrent inability to attain and or maintain penile erection sufficient for sexual satisfaction including satisfactory sexual performance the most common causes of ed are vascular disease and medication side effects other important causes of ed are low testosterone and psychogenic factors and any evaluation for ed should also include an assessment of cardiovascular risk factors that concludes this video on an approach to erectile dysfunction
for more videos on an approach to symptoms and a large variety of other medical topics consider subscribing to strong medicine thanks for watching you
Related Videos

10:22
An Approach to Generalized Pruritus (Itching)
Strong Medicine
17,288 views

12:29
Is erectile dysfunction all in your head? ...
Rena Malik, M.D.
313,154 views

8:03
Understanding Erectile Dysfunction (ED): W...
MedBoard
4,663 views

20:34
An Approach to Male Infertility
Strong Medicine
42,110 views

13:19
Erectile Dysfunction
CanadaQBank
3,727 views

29:04
What causes erectile dysfunction and what ...
Peter Attia MD
89,210 views

10:18
Everything you need to know about Sildenaf...
Rena Malik, M.D.
8,446,799 views

1:00:54
5.6.2020 Urology COViD Didactics - Pathoph...
Urology Residents
5,912 views

37:54
How To Treat Erectile Dysfunction Without ...
Mark Hyman, MD
1,195,946 views
![Shock Wave Therapy For Erectile Dysfunction - Fact or Fiction? | [UWave]](https://img.youtube.com/vi/DS1XqgLHOvc/mqdefault.jpg)
12:20
Shock Wave Therapy For Erectile Dysfunctio...
Indy Men's Health
410,147 views

26:23
How An Erection Works
The Infographics Show
1,544,456 views

8:34
Erectile Dysfunction & Physical Therapy Tr...
JAG Physical Therapy: Pelvic Health
888,240 views

16:39
Erectile Dysfunction: What It Really Is An...
Talking With Docs
714,611 views
6:31
Ask a Urologist: What Are the BEST PILLS f...
hims
15,964 views

7:12
6 Most Common Causes Of Low Libido In Men 😮
Dr. Sam Bailey
1,198,997 views

17:53
Treating Psychological Impotence (Erectile...
Mark Tyrrell
377,642 views

8:29
Urologist explains Premature Ejaculation |...
Doctor Eric
1,076,616 views

48:01
Erectile Dysfunction: Exploring Options fo...
Johns Hopkins Medicine
6,034 views

6:10
Do YOU have Erectile Dysfunction ? | Why i...
JHP Medical UK
1,812,089 views

15:58
An Approach to Chronic Diarrhea
Strong Medicine
150,491 views