Categorizing Drugs: Classes, Names, and Schedules
287.04k views1661 WordsCopy TextShare
Professor Dave Explains
How do we categorize drugs? How do we name them? This is quite a bit trickier than one might think, ...
Video Transcript:
Professor Dave here, let’s classify some drugs. Whenever we are studying something that comes in so many varieties, we need some way of classifying them, just like the way we use taxonomy to classify living organisms. With drugs, it can be a little complicated, because there are different ways we might wish to categorize them.
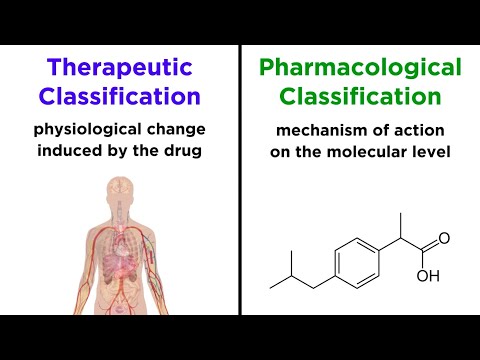
We might group them according to the type of molecule they are, or by what it does clinically, or by the mechanism of action. These methods all have their own utility, so let’s talk a bit about them now, as well as a few related topics. The main distinction we want to make is the difference between therapeutic classification, and pharmacological classification.
The first of these describes the purpose of the drug, or essentially the main physiological change that is induced by the drug on the organismal level. The second of these describes the mechanism of action, or what the drug does on the molecular level. Let’s go through some examples of each.
First, looking at therapeutic classification, let’s mention some classes of drugs that deal with the heart and blood vessels. Anticoagulants are drugs that help prevent blood clots. Antihyperlipidemics lower blood-cholesterol.
Antihypertensives lower blood pressure. Antidysrhythmics or antiarrhythmics treat an abnormal heartbeat. So as you can see, this type of classification describes the clinical purpose, or the physiological change induced by the drug, and does not describe anything about the way the drug achieves this change.
A large percentage of these categories begin with the prefix “anti”, because anti means “against”, and these categories describe the condition that the drug is working against. There are antipsychotics, antidepressants, anticonvulsants, antinauseants, and so forth. Some of their functions are immediately apparent from the name, while others require a little more background information.
Of course there are other classes that don’t begin with this prefix. Decongestants, hallucinogens, sedatives, stimulants, it’s a long list, and many or most of these will be addressed at some point in this series. By contrast, as we said, pharmacological classification describes the specific thing that the drug does on the molecular level in order to elicit the desired physiological effect.
Again focusing on the heart and blood vessels, calcium channel blockers quite literally block calcium channels in the heart, which are protein channels in the membranes of cells that regulate the passage of calcium ions in and out of the cell. Angiotensin-converting enzyme inhibitors, or ACE inhibitors, discourage the formation of angiotensin II by inhibiting the enzyme responsible for its production from angiotensin I. Beta-adrenergic blockers, or beta-blockers, inhibit proteins that are supposed to receive the hormone epinephrine, commonly known as adrenaline.
As it happens, the therapeutic effect is that the heartbeat is slowed and the blood pressure is lowered. So a specific drug could feasibly be described as either a beta blocker or an antihypertensive. The classification will simply depend on the context, and what it is that is being examined or described at any particular moment, and depending on the efficacy of a particular drug, one label may be more appropriate, or at least more commonly used.
As you can see, with pharmacological classification, we are typically dealing with the way that the drug interacts with some biomolecule, usually a protein. This protein may be an enzyme, it may be a receptor, or otherwise, but there is typically some interaction between the drug and this protein that modifies the activity of that protein. For this reason, pharmacological classification is more specific than therapeutic classification, and significant knowledge of biochemistry is absolutely crucial in order for pharmacological classification to make any sense whatsoever.
Now that we have an idea of how drugs are classified, let’s talk about how they are named. There is quite a bit of confusion amongst the public regarding drug names, and this is largely because all drugs always have multiple names. Drgs can have a chemical name, a generic name, and a trade name, or brand name.
First, the chemical name is quite straightforward. This is determined by the rules of chemical nomenclature designated by the IUPAC, or International Union of Pure and Applied Chemistry, precisely as we learned way back at the beginning of the organic chemistry series. A drug will only have one chemical name, because the rules are highly specific, and exist precisely for the purpose of giving any molecule one unambiguous name, even if it is very long and impractical for general use, such as this one.
Because of the way these names are derived, they tend to be “chemically” sounding, which causes many sectors of the public to recoil, strictly due to chemophobia, which is an irrational fear of chemicals, and chemical-sounding things. For example, this drug is called 2-acetoxybenzoic acid. X’s and Z’s are particularly scary sounding, as is the word “acid”, so some people may presume that this is a harmful chemical.
However, in the United States this drug is more commonly known by its generic name, aspirin. Generic names are typically assigned by the U. S.
Adopted Name Council, specifically for the purpose of giving drugs with long chemical names, often much longer than this one, another name that is short and easy to remember, even though it does not actually describe the composition of the molecule. There is only one generic name for any drug, so drugs are most commonly referred to by their generic names, since non-chemists, which is most of us, do not have the vocabulary required to pronounce or understand most chemical names. Generic names should be memorized, as it is rather easy to do so, and they are useful.
Now the third name is where it gets tricky. Whereas a drug must have only one chemical name and only one generic name, it can have any number of brand names. That’s because anyone who makes the drug can call it whatever they want, and the name that is chosen is completely meaningless, outside of the context of marketing.
For example, you may be familiar with a drug named Empirin. Well, Empirin is aspirin. They are completely synonymous.
But Empirin is a brand name that is trademarked, and can be advertised in any manner desired by its producers. Anyone else can mass produce aspirin and call it whatever they want as well. Another generic name for a drug that you may be familiar with is ibuprofen.
Now consider the brand names Advil and Motrin. These are also ibuprofen, and nothing but ibuprofen. The pill itself may look different cosmetically, but the active ingredient is identical.
We can say the same thing about acetaminophen and Tylenol, and countless other examples. Pharmaceutical companies rely on brand recognition as a result of advertising efforts in order to produce a bias in consumer trends towards their version of the drug, resting on the fact that most people do not realize that there is no difference, apart from dosage. A difference does arise, however, when it comes to combination drugs.
Excedrin is a mixture of acetaminophen, aspirin, and caffeine, intended to combine the effects of these three drugs to produce more effective pain relief. In addition, while the active ingredient in a brand name drug and its generic counterpart is 100 percent identical, there can potentially be a discrepancy in bioavailability, or the ability of the drug to move through the body to reach its target and elicit the desired effect. This is due to inactive ingredients which can influence the degree of absorption, and other related factors, but typically these discrepancies are minimal or even completely negligible.
Later in the series, we will discuss the legal aspects of brand name drugs vs. generic drugs, exclusive rights, price differentials, profit margins, and other key issues associated with the sale of popular drugs. Lastly, there is one more method of classification that we must learn, and it is one that is associated with drugs that have the potential for abuse.
These are drugs that have some likelihood of resulting in either physical or psychological dependency, or both. Essentially, we are talking about drug addiction. We elucidated many aspects of drug addiction in this tutorial from my biopsychology series, so be sure to check that out for more information or further clarification on certain terminology.
Otherwise, let’s simply understand that drugs with this quality are called scheduled drugs, and they are classified according to the degree of their potential for abuse. Schedule I drugs have the highest potential for abuse, followed by II, III, IV, and then schedule V drugs have the lowest potential for abuse. The greater the abuse potential, the less therapeutic application a drug typically has, so schedule I drugs include drugs like heroin, which is the most addictive substance known to man.
Schedule II drugs have some therapeutic purpose but still a very high dependency potential, such as morphine, and cocaine. Schedule III drugs include ketamine, anabolic steroids, and products with low levels of codeine. Schedule IV drugs include Valium and Xanax.
And schedule V drugs include things like cough medicines, and are often available over the counter. These have a very low dependency potential. We should note that some drugs that do cause addiction are not included in this classification, such as alcohol and caffeine.
We should also note that there can be propaganda associated with the placement of certain drugs in a particular schedule, such as marijuana and LSD qualifying as schedule I drugs, given that there is little to no evidence that these substances produce any kind of dependency that could be comparable to a substance like heroin. So with that, we are beginning to piece together an understanding of how we categorize drugs, and how we name them. As we move through this series, the categories and names of drugs will become more familiar, and gaps will get filled in as we begin to develop a broader and more comprehensive knowledge base.
But before we start that process, let’s go through some more general concepts.
Related Videos

7:48
Methods of Drug Administration
Professor Dave Explains
192,438 views

20:03
How to remember drug names easily
egpat
873,638 views

34:33
The Tale of Trump and the Woke Trans Mice
Professor Dave Explains
297,005 views
7:36
Antibiotic Classes in 7 minutes!!
Dr Matt & Dr Mike
1,950,217 views

1:31:26
Sabine Hossenfelder Can’t Stop Acting Like...
Professor Dave Explains
421,834 views

7:38
Introduction to Pharmacology
Professor Dave Explains
374,900 views

8:15
Pharmacodynamics: Mechanisms of Drug Action
Professor Dave Explains
350,091 views
![Antihypertensive Drug Chart: Pharmacology Made Easy [Classes, Medication Trick, Mechanism of Action]](https://img.youtube.com/vi/owcZmS5KwHw/mqdefault.jpg)
16:08
Antihypertensive Drug Chart: Pharmacology ...
EZmed
520,223 views

15:13
Every Illegal Drug Explained in 15 Minutes
The Infographics Show
425,502 views

24:28
Pharmacokinetics and Pharmacodynamics
Dirty Medicine
288,044 views

28:49
Top 200 Drugs Pharmacy Flashcards with Aud...
Amanda PharmD
600,921 views

11:45
Glucocorticoids: Mechanisms and Side Effects
Professor Dave Explains
45,026 views

43:00
Drugs of Abuse (Mechanism, Intoxication, W...
Dirty Medicine
371,635 views

53:25
Reacting to Pathetic “Answers in Genesis” ...
Professor Dave Explains
329,388 views
14:25
Pharmacokinetics: Absorption, Distribution...
EKG Science
76,102 views

22:26
Pharmacology Made Easy (Part 1) - Common M...
PicmonicVideo
1,314,998 views

35:53
My Drug Tier List 2023
Goblin
1,742,017 views
![Antibiotic Classes: Mnemonic, Coverage, Mechanism of Action [Pharmacology Made Easy]](https://img.youtube.com/vi/_-UHhkIYht4/mqdefault.jpg)
10:58
Antibiotic Classes: Mnemonic, Coverage, Me...
EZmed
1,038,698 views

8:50
Introduction, Drug Names, Medication Regul...
Level Up RN
64,277 views

2:40:46
Antiarrhythmic Drugs
Ninja Nerd
373,465 views