Rheumatoid arthritis - causes, symptoms, diagnosis, treatment, pathology
1.97M views1554 WordsCopy TextShare
Osmosis from Elsevier
What is rheumatoid arthritis? Rheumatoid arthritis is an autoimmune condition where the immune syste...
Video Transcript:
Learning medicine is hard work! Osmosis makes it easy. It takes your lectures and notes to create a personalized study plan with exclusive videos, practice questions and flashcards, and so much more.
Try it free today! In rheumatoid arthritis, “arthr-“ refers to joints, “-itis” means inflammation, and “rheumatoid” comes from rheumatism, which more broadly refers to a musculoskeletal illness. So, rheumatoid arthritis is a chronic, inflammatory disorder that mostly affects the joints, but can also involve other organ systems like the skin and lungs as well.
Alright, so a healthy joint typically has two bones covered with articular cartilage at the ends. Articular cartilage is a type of connective tissue that acts like a protective cushion - a lubricated surface for bones to smoothly glide against. One type of joint, like the knee joint is called a synovial joint.
A synovial joint connects two bones with a fibrous joint capsule that is continuous with the periosteum or outer layer of both bones. The fibrous capsule is lined with a synovial membrane that has cells that produce synovial fluid and remove debris. The synovial fluid is normally a viscous fluid like the jelly-like part of a chicken egg and it helps lubricate the joint.
To help serve these synovial cells, the synovial membrane also has blood vessels and lymphatics running through it. Together, the synovial membrane and the articular cartilage form the inner lining of the joint space. Rheumatoid arthritis is an autoimmune process that is typically triggered by an interaction between a genetic factor and the environment.
For example, a person with a certain gene for an immune protein like human leukocyte antigen, or HLA- DR1 and HLA–DR4, might develop rheumatoid arthritis after getting exposed to something in the environment like cigarette smoke or a specific pathogen like a bacteria that lives in the intestines. These environmental factors can cause modification of our own antigens, such as IgG antibodies or other proteins like type II collagen or vimentin. Τype II collagen and vimentin can get modified through a process called citrullination.
That’s when the amino acid arginine found in these proteins is converted into another amino acid, citrulline. Meanwhile, due to the susceptibility genes HLA- DR1 and HLA–DR4, immune cells sometimes are not “clever” enough, so they get confused by these changes and they no longer recognize these proteins as self-antigens. The antigens get picked up by antigen- presenting cells, and get carried to the lymph nodes to activate CD4+ T-helper cells.
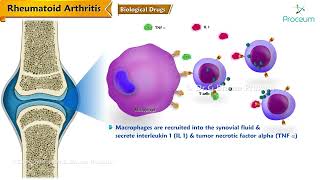
T-helper cells stimulate the nearby B- cells to start proliferating and differentiate into plasma cells, which produce specific autoantibodies against these self- antigens. In rheumatoid arthritis, T- helper cells and antibodies enter the circulation and reach the joints. Once there, T- cells secrete cytokines like interferon- γ and interleukin- 17, to recruit more inflammatory cells like macrophages, into the joint space.
Macrophages will also produce inflammatory cytokines, like tumor necrosis factor, or TNF- α, interleukin- 1 and interleukin- 6, which together with the T-cell’s cytokines, stimulate synovial cells to proliferate. The increase in synovial cells and immune cells creates a pannus, which is a thick, swollen synovial membrane with granulation or scar tissue, made up of fibroblasts, myofibroblasts and inflammatory cells. Over time, the pannus can damage cartilage and other soft tissues and also erode bone.
Activated synovial cells also secrete proteases which break down the proteins in the articular cartilage. Without the protective cartilage, the underlying bones are exposed and can directly rub against one another. In addition, inflammatory cytokines increase a protein on the surface of T- cells, known as RANKL or receptor activator of nuclear factor kappa-B ligand.
RANKL allows the T-cells to bind RANK, a protein on the surface of osteoclasts, to get them to start breaking down bone. Meanwhile, antibodies also enter the joint space. One antibody is called rheumatoid factor, or RF, which is an IgM antibody that targets the constant Fc domain of altered IgG antibodies.
Another antibody is anti-cyclic citrullinated peptide antibody, or CCP, which targets citrullinated proteins. When these antibodies bind to their targets, they form immune complexes which accumulate in the synovial fluid. There, they activate the complement system, a family of 9 small proteins that work in an enzymatic cascade to promote joint inflammation and injury.
Finally the chronic inflammation causes angiogenesis, or the formation of new blood vessels around the joint, which allows even more inflammatory cells to arrive. As the disease progresses, multiple joints on both sides of the body get inflamed and gradually destroyed. But these inflammatory cytokines don’t just stay within the tight joint space.
Instead, they escape through the bloodstream and reach multiple organ systems causing extra-articular problems, meaning problems beyond the joint space. For example, interleukin-1 or -6 travel to the brain, where they act as pyrogens, inducing fever. In skeletal muscle, they promote protein breakdown and in the skin, as well as in many visceral organs, they lead to the formation of rheumatoid nodules, which are round- shaped collections of macrophages and lymphocytes with a central area of necrosis, or tissue death.
Blood vessels can also be affected. Their walls get inflamed, resulting in various forms of vasculitis and make them prone to developing atheromatous or fibrofatty plaques. In response to inflammatory cytokines, the liver also starts producing high amounts of hepcidin, a protein that decreases serum iron levels by inhibiting its absorption by the gut and trapping it into macrophages or liver cells.
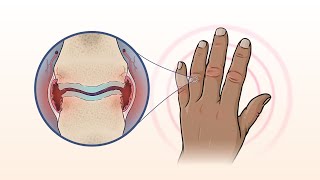
Meanwhile, within the lung interstitium, fibroblasts get activated and proliferate, causing fibrotic or scar tissue that makes it harder for the alveolar gas exchange, while also the pleural cavities surrounding the lungs can get inflamed, filling up with fluid, known as pleural effusion, and this can sometimes mess with lung expansion. Rheumatoid arthritis typically involve multiple joints, usually five or more, symmetrically, meaning the same joint groups on both sides of the body, like both hands for instance. Commonly affected joints are the small joints like metacarpophalangeal and proximal interphalangeal joints of the hands, and the metatarsophalangeal joints of the feet.
As the disease worsens, it can start to affect large joints like the shoulders, elbows, knees and ankles. During “flares” or sudden worsening of the disease, the affected joints get extremely swollen, warm, red, and painful. Over time, they become stiff, especially in the morning or after being inactive for a prolonged period of time.
People with rheumatoid arthritis may develop specific deformities, usually of the metacarpophalangeal joints in the hand, such as ulnar deviation of the fingers. Deformities are also common in the interphalangeal joints, such as the so- called boutonniere or buttonhole deformity. This occurs when the extensor tendon in the back of the finger splits and the head of the proximal phalanges pokes through like a button through a buttonhole, causing flexion of the proximal interphalangeal joint and hyperextension of distal interphalangeal joint.
Another finger deformity is the swan neck deformity, which is the opposite, so there’s hyperextension of the proximal interphalangeal joint and flexion of the distal interphalangeal joint. Now, in the knee joint, a one-way value can form, with fluid from the swollen knee filling the semi-membranous bursa. When that happens, the synovial sac can get so swollen that it bulges posteriorly into the popliteal fossa, creating a synovial fluid-filled cyst, called a Baker or popliteal cyst.
Now, extra- articular manifestations include non-specific symptoms of inflammation, such as fever, low appetite, malaise or muscle weakness, and organ- specific, manifistations include rheumatoid nodules or firm bumps of tissue, and these most commonly in the skin around pressure points, such as the elbows. More rarely, in the lungs, the heart, or the sclera of the eye. There’s also an increased risk of atherosclerosis and therefore, heart attack or stroke.
There’s also anemia, interstitial lung fibrosis and pleural effusions, which can present as progressive shortness of breath. One particularly serious condition that’s associated with rheumatoid arthritis is Felty syndrome which is a triad of rheumatoid arthritis, splenomegaly, and granulocytopenia, and it can lead to life-threatening infections. Diagnosis of rheumatoid arthritis usually involves confirmatory blood tests, like looking for the presence of rheumatoid factor and anti-citrullinated peptide antibody.
Additionally, imaging studies, such as X- ray, usually reveal decreased bone density around affected joints, soft tissue swelling, narrowing of the joint space, and bony erosions. The long term management of rheumatoid arthritis is use of disease-modifying antirheumatic medications like methotrexate, hydroxychloroquine, sulfasalazine, and which can help to suppress the inflammation. In addition, there are a variety of medications called biologic response modifiers or biologics.
Some biologics, such as abatacept, work by suppressing the activity of T cells, or others, such as rituximab suppress B cells. There are also biologics such as adalimumab, etanercept, and infliximab, that block various chemokines like tumor necrosis factor. Anakinra blocks interleukin 1 which is blocked by, and tocilizumab blocks interleukin 6.
Treatment of acute flares can be done with anti- inflammatory medications like NSAIDS as well as short term use of glucocorticoids. All right, so as a quick recap, rheumatoid arthritis is a systemic inflammatory disorder of autoimmune origin that is primarily characterized by progressive, symmetric joint destruction, especially in the wrists and fingers, but may also affect other joints and many organs, such as the skin, heart, blood vessels and lungs. It’s marked by elevated rheumatoid factor and anti- cyclic citrullinated peptide antibodies.
Related Videos
11:11
Systemic lupus erythematosus (SLE) - cause...
Osmosis from Elsevier
2,534,367 views

25:55
Rheumatoid Arthritis Nursing NCLEX Lecture...
RegisteredNurseRN
807,446 views
10:11
Physical Abuse and Death in Custody - Deat...
sqadia.com
1 view

12:49
#066 Anti inflammatory food diet for chron...
Dr. Andrea Furlan
3,598,902 views

13:07
Osteoarthritis vs. Rheumatoid Arthritis
Dirty Medicine
73,841 views
11:32
Tuberculosis - causes, symptoms, diagnosis...
Osmosis from Elsevier
1,791,772 views

5:28
Rheumatoid Arthritis Animation
Nucleus Medical Media
4,162,417 views
15:00
What Is Rheumatoid Arthritis? | NEJM
NEJM Group
46,685 views
![Rheumatoid Arthritis [Symptoms, Early Signs, Stages & BEST Treatment]](https://img.youtube.com/vi/CTtIMGqTwXQ/mqdefault.jpg)
22:30
Rheumatoid Arthritis [Symptoms, Early Sign...
Michigan Foot Doctors
138,435 views

12:21
Non-hodgkin lymphoma - causes, symptoms, d...
Osmosis from Elsevier
1,182,194 views

25:48
My Rheumatoid Arthritis (RA) Story
Swavy Curly Courtney
118,289 views

10:41
Bone tumors - causes, symptoms, diagnosis,...
Osmosis from Elsevier
642,877 views

7:14
Osteoarthritis - causes, symptoms, diagnos...
Osmosis from Elsevier
1,380,933 views

14:23
Vasculitis | Clinical Presentation
Medscape
360,388 views

10:31
Early Warning Signs Of Rheumatoid Arthriti...
Dr. Diana Girnita - Rheumatologist OnCall
335,914 views

14:51
Osteoarthritis and Rheumatoid Arthritis - ...
Level Up RN
192,913 views
8:27
Osteoporosis - causes, symptoms, diagnosis...
Osmosis from Elsevier
124,253 views
16:48
Rheumatoid Arthritis Pharmacology - DMARDs...
Dr.G Bhanu Prakash Animated Medical Videos
2,594 views

1:09:29
Tuberculosis
Ninja Nerd
471,101 views

15:34
Rheumatoid Arthritis Pathophysiology (sign...
Armando Hasudungan
930,507 views