Colorectal Cancer - Overview
703.35k views989 WordsCopy TextShare
Armando Hasudungan
Support me:
🖼️ Buy PDFs: http://armandoh.org/shop
💵 Patreon: http://www.patreon.com/armando
👕 B...
Video Transcript:
in this video we're going to talk about color rectal cancer this is an overview and introduction uh coloror cancer is the second most commonly diagnosed cancer and is the commonest gastrointestinal malignancy the prevalence of Choral cancer is increasing in in the younger population and this could be attributed to diet this is also the same with d verticular disease family history is strong in coloral cancer the risk factors for developing coloral cancer include age male sex smoking family history as we discussed diet high in red meat and poron fiber polyposis syndrome or fap fap and hnpcc
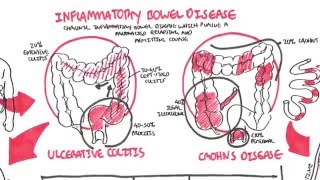
or Lynch disease other risk factors also include history of polyps certain types of polyps that is uh personal history of colon cancer and also having inflammatory conditions of the bowel including all sort of colitis and Crohn's disease the signs and symptoms or clinical presentation differ depending on where the cancer or growth occurs within the bowel of course this is just a summary people vary in their clinical presentation so here I'm drawing a colon ascending transverse descending sigmoid and the rectum cancerous tumors that occur on the right side account for 20% of cases of colon cancer
people are often asymptomatic present with weight loss and um iron deficiency people alsoe present with a palpable Mass on the on the lower right quadrant of the abdomen and this is this is because they are often asymptomatic and so the tumor can grow without notice until signs of weight loss and anemia occurs tumors occurring in the descending sigmoid area account for the majority of colon cancer 75% of cases patients can complain of dog red blood mixed in with stools plus minus clots there can be increased bow frequency abdominal pain and bloating flatulence and mucus present
tumors occurring in the rectal regions can present with deep red blood on the surface of the stool people can also have abdominal pain plus minus tanmos you can imagine a growth in the rectum would cause sensation of incomplete um evacuation the colon is an amazing organ General macroscopic differences between normal and cancerous the colon have tin coli which are separate longitudinal ribbons of smooth muscles on the outside of the ascending transverse descending and sigmoid colons the tin coli contract lengthwise to produce the HRA the bulges in the actual colon the colon is supplied by arteries
that Branch from the inferior misic artery the inferior misic artery further branches into smaller arteries which Anastos with with each other these have importance when part of the colon is is being reected because we want to maintain blood flow to the remainder of the colon when colon cancer occurs the tumus can obstruct the Lumen the chemical produced by the cancers can cause um angiogenesis formation of new blood vessels which contribute to the bleeding found in colon cancer so patients often present with rectal bleeding pathology colon cancer can come in a few pathological forms polypoid ulcerative
stenosing and infiltrative at the end of the day these different pathological types can and will eventually lead to some form of obstruction investigations the investigations performed for patients suspected of colon cancer or any form of mass includes an abdominal examination followed by a per rectal examination and this is done with the proctoscopy to check for any obvious masses and source of bleeding such as from internal hemorrhoids colonoscopy is then considered which is under general anesthesia and involves the doctor inserting a colonoscope through the back passage and visualizing the colon polyps can be taken out and
sampled to check for malignancy Barum anmr colonography can also be performed finally you have blood investigations which include lft FBC and the tumor marker for colon cancer CA once and if the cancer is diagnosed it is important to Stage the cancer staging investigations used include biopsies CT scans and pet scans for staging itself there are two forms of staging the first is the tnm staging which looks at T the primary tumor n the lymph node and M metastasis the second form of staging is Juke staging which looks at the 5e survival and there are a
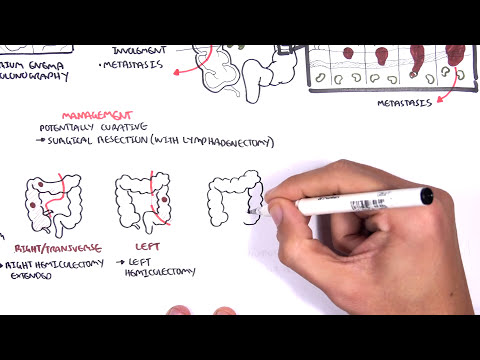
total of four stages plus stage zero stage zero is nothing really and benign the remainder of the stages it depends on how deep the tumor is going so what layers it's going into and if and if it has metastasized so stage zero there's a 90% 5year survival stage two the tumor is growing even deeper 70% 5year survival stage three about 30% stage four it's less than 10% 5year survival with metastasis management of colon cancer colon cancer is potentially Curative with surgical reection of the colon colectomy with also surgical reection of the lymph nodes lymphadenectomy surgical
rection of the colon colectomy is performed um depending on where the tumor is located on the colon and when surgically removing parts of the colon it is important to take into consideration the blood supply of that part of the colon as well as the lymph drainage of that part tumors that occur on the right side of the of the uh Lodge intestine or the or in the right Transit this area requires a right hemicolectomy extended tumors occurring on the left side require left hemicolectomy tumors occurring in the sigmoid and erectum require a high anterior section
tumors in the rectum require aper um AB abdominal peral reection also during this procedure some patients may may require having a temporary or even a permanent colostomy bag pouches which While others um get the colon joined uh to the other parts to the remaining parts of the colon eventually of course together with colectomy there is adant chemotherapy with or without radiotherapy chemotherapy usually involves five floral urasil if the cancer has metastasis Iz that organ can be potentially removed and finally there is also pallative care
Related Videos
11:04
Bladder Cancer - Overview (types, pathophy...
Armando Hasudungan
309,430 views
8:45
Colorectal carcinoma - causes, symptoms, d...
Osmosis from Elsevier
232,005 views

31:58
Colon Cancer (CRC) Risk Factors, Pathogene...
JJ Medicine
204,161 views

21:58
Colon cancer - 20 Signs & Symptoms - Clear...
Medicosis Perfectionalis
8,902 views
9:50
Colorectal Cancer Surgery: principles and ...
Oncology for Medical Students
134,280 views
16:49
Patient Teaching: Low Anterior Resection -...
TVASurg
31,825 views

22:42
I Ignored the Signs - Jason | Stage 4 Colo...
The Patient Story
568,158 views
24:15
My Stomach Pain Turned Out To Be Colon Can...
The Patient Story
378,354 views

8:02
Understanding Colorectal Cancer (Includes ...
Rhesus Medicine
70,518 views

29:05
Colon Cancer at 32 - Allison | Colorectal ...
The Patient Story
36,735 views
10:37
Understanding Pancreatic Cancer
Zero To Finals
242,291 views
5:15
What happens during and after a colonoscopy?
You and Colonoscopy
21,043,766 views

30:11
Stage 4 Survivor Stephen | Colorectal Canc...
Survivor Jelena
43,834 views

10:05
The Colon and Colon Cancer
Armando Hasudungan
210,800 views

26:05
My Colon Cancer Symptoms: Keith’s Stage 4 ...
The Patient Story
118,255 views

18:45
How I Discovered I had Colorectal Cancer |...
The Patient Story
295,130 views

28:40
Medical Gaslighting: My Colon Cancer Sympt...
The Patient Story
2,934,448 views

27:07
Colon & Rectal Cancer: What You Need to Know
Cancer Informant
46,061 views

4:18
Colorectal Cancer Staging
Surgical Teaching
23,754 views
8:59
Inflammatory Bowel Disease - Crohns and Ul...
Armando Hasudungan
1,300,805 views