Formation of Urine - Nephron Function, Animation.
1.91M views905 WordsCopy TextShare
Alila Medical Media
(USMLE topics) Renal physiology - The 3 stages of urine formation. With explanation of the counter c...
Video Transcript:
The kidneys filter blood plasma, removing metabolic wastes, toxins, and excrete them in urine. During this process, they also maintain CONSTANT volume and composition of the blood, or homeostasis. Blood enters the kidney via the RENAL ARTERY, which divides into SMALLER arteries, then arterioles.
The arterioles get into contact with functional units of the kidney called the NEPHRONS. This is where blood filtration and urine formation take place. The FILTERED BLOOD then passes through a series of veins and exits the kidney via the RENAL VEIN.
The URINE is collected in collecting ducts and leaves the kidney via the URETERS. Each kidney contains over a million nephrons. A nephron consists of 2 major parts: a glomerular capsule, or Bowman’s capsule; and a LONG renal tubule.
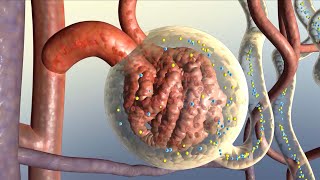
Renal tubules of several nephrons connect to a common collecting duct. There are 3 steps in the formation of urine: glomerular filtration; tubular REabsorption and secretion; and water conservation. Blood enters the Bowman’s capsule via the Afferent arteriole, passes through a ball of capillaries called the GLOMERULUS, then leaves via the Efferent arteriole.
The Afferent arteriole is significantly LARGER than the Efferent arteriole, creating a blood flow with a LARGE INLET and SMALL OUTLET. As a result, the blood hydrostatic PRESSURE in these capillaries is MUCH HIGHER than usual. Hydrostatic and osmotic pressures DRIVE water and solutes FROM blood plasma, through a FILTRATION MEMBRANE, INTO the capsular space of the nephron.
The filtration membrane acts like a sieve, allowing ONLY SMALL molecules to pass through. These include water, inorganic ions, glucose, amino acids and various metabolic wastes such as urea and creatinine; and make up the GLOMERULAR FILTRATE. The amount of filtrate produced per minute is called glomerular FILTRATION RATE, GFR.
GFR is kept at a STABLE value by several FEEDBACK mechanisms within the kidneys, known as RENAL AUTOregulation. GFR is also under SYMPATHETIC and HORMONAL control. GFR regulation is generally achieved by CONSTRICTION or DILATION of the Afferent arteriole, which causes the GLOMERULAR blood pressure to FALL or RISE, respectively.
In a healthy person, the total filtrate volume amounts to between 150 and 180 litters a day. However, only about 1% of this is excreted as urine, the remaining 99% is REabsorbed BACK to the blood as the filtrate flows through the LONG renal tubule. This is possible because the Efferent arteriole, after exiting the Bowman’s capsule, BRANCHES OUT to form a network of so-called PERItubular capillaries, which SURROUND the renal tubule.
The FIRST part of the tubule, the PROXIMAL convoluted tubule, REabsorbs about two thirds of the filtrate. In this process, water and solutes are driven through the EPITHELIAL cells that LINE the tubule, into the extracellular space. They are then taken up by the peritubular capillaries.
SODIUM REabsorption is most important, as it creates OSMOTIC pressure that DRIVES WATER; and ELECTRICAL gradient that drives NEGATIVELY charged ions. Sodium level INSIDE the epithelial cells is kept LOW thanks to the sodium-potassium pumps that constantly PUMP sodium ions OUT into the extracellular space. This creates a CONCENTRATION GRADIENT that favors sodium diffusion FROM tubular fluid INTO the cells.
Sodium is absorbed by SYMPORT proteins that ALSO bind GLUCOSE and some other solutes. Nearly ALL glucose and amino acids are REabsorbed at this stage. About half of nitrogenous wastes also REabsorb back into the bloodstream.
The kidneys REDUCE the blood levels of metabolic wastes to a SAFE amount, but do NOT completely eliminate them. Some of the REabsorption also occurs by the paracellular route through TIGHT junctions BETWEEN epithelial cells. At the same time, TUBULAR SECRETION, where ADDITIONAL wastes and other solutes LEAVE the bloodstream to join the tubular fluid, also takes place.
The processes of REabsorption and secretion continue in the nephron loop, the loop of Henle, and the DISTAL convoluted tubule. These parts of the tubule also have some OTHER important functions. The main function of the loop of Henle is to CREATE and maintain an OSMOLARITY GRADIENT in the medulla that enables the collecting ducts to CONCENTRATE urine at a later stage.
The ASCENDING limb of the loop ACTIVELY pumps sodium OUT, making the medulla “SALTY”. The DESCENDING limb is permeable to water but MUCH LESS to sodium. As the water exits the tubule by osmosis, the filtrate becomes more and more CONCENTRATED as it reaches the bottom.
The ASCENDING limb, on the other hand, is permeable to ions but NOT water. As a result, the filtrate LOSES sodium as it goes UP and becomes more DILUTED at the TOP of the loop. The medulla is in EQUILIBRIUM with the loop and hence has the SAME SALINITY GRADIENT - SALTIER at the bottom.
REabsorption and secretion in the DISTAL convoluted tubule are under control of various hormones. This is how the kidneys respond to the body’s needs and adjust the composition of urine accordingly. The COLLECTING DUCT receives tubular fluid from several nephrons.
The main function of the collecting duct is to CONCENTRATE URINE and therefore CONSERVE WATER. This is made possible by the osmolarity gradient generated by the loop of Henle. As it gets SALTIER deep in the medulla, the filtrate LOSES water as it flows DOWN the collecting duct.
The collecting duct is also under HORMONAL CONTROL so it can adjust the amount of REabsorbed water according to the body’s state of HYDRATION. For example, when the body is DEHYDRATED, MORE water is REabsorbed back to the blood and the excreted urine is more concentrated.
Related Videos

1:39
Micturition Reflex - Neural Control of Uri...
Alila Medical Media
451,181 views

13:58
Nephrons - Filtration and Reabsorption Basics
Siebert Science
452,926 views
3:33
How Your Kidneys Work
Nucleus Medical Media
332,874 views

Wednesday Morning Jazz - Cozy Fall Coffee ...
Autumn city

7:55
Nephron Function
Handwritten Tutorials
1,904,479 views

10:48
Regulation of Renal Blood Flow
Osmosis from Elsevier
291,863 views

2:54
Animation E1, 1.1 Ultrafiltration and reab...
Oxford Mastering Biology 牛津基礎生物學
92,839 views
43:09
Renal | Glomerular Filtration
Ninja Nerd
1,380,650 views

4:39
Kidney Failure
Nucleus Medical Media
378,280 views

11:25
Is Our World Broken?
Kurzgesagt – In a Nutshell
1,466,949 views

3:55
How do your kidneys work? - Emma Bryce
TED-Ed
2,292,296 views
28:06
Renal | Loop of Henle
Ninja Nerd
628,715 views

36:39
Renal | Filtration, Reabsorption, and Secr...
Ninja Nerd
1,058,257 views
18:38
The kidney and nephron | Renal system phys...
Khan Academy
2,859,005 views
10:18
Urinary System, Part 1: Crash Course Anato...
CrashCourse
4,818,684 views

19:52
Renin-Angiotensin-Aldosterone System (RAA ...
Siebert Science
122,544 views
9:50
Excretory System and the Nephron
Amoeba Sisters
1,281,792 views

18:07
NEPHRON Structure & Function Made Easy - H...
MEDSimplified
1,428,247 views

26:49
Renal | The Collecting Duct
Ninja Nerd
329,466 views

10:15
Countercurrent Mechanism | Loop of Henle |...
Byte Size Med
355,988 views