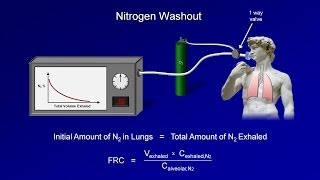
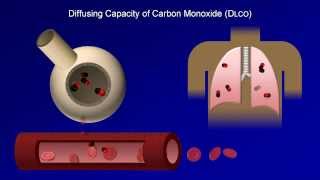
[Music] this is Eric strong from Stanford University this is the first video in a five video series on pulmonary function tests very briefly this series will begin with an introduction to pulmonary function tests or pfts next I'll discuss barometry including flow volume Loops then lung volumes including the techniques used to measure them the fourth video we'll discuss the interesting test of the lungs diffusing capacity of carbon monoxide abbreviated dlco finally the series will end with a brief summary along with some practice cases that will also incorporate some clinical history and chest x-rays to help integrate
PFT inter interpretation into a broader understanding of the pathology of the pulmonary system the specific learning objectives for this introduction will be to know the general purpose of pfts to know the different types of pfts to know the three major categories of chronic diffused lung disease and finally to understand the various subdivisions of the lung volume let me start by asking what are the purposes of pfts what are the general reasons that would lead a clinician to order them first and foremost they can be used to diagnose symptomatic disease this is by a large margin
the most common reason to order them typical symptoms or signs that might trigger pfts would be chronic dpia or cough or unexplained hypercapnia or hypoxemia particularly if any of these develop in a patient at increased risk of lung disease such as smokers and those with o occupational exposures however pfts can also be used to screen for early asymptomatic disease in patients at high risk for example patients on long-term amone which has significant pulmonary toxicity pfts can also be used for prognostication of known disease along similar lines they can be used to estimate surgical risk and
likelihood of favorable outcome in some specific circumstances such as lung resection in patients with COPD finally they can also be used to monitor response to treatment though most pulmonary diseases are best monitored by symptoms since diagnosis of symptomatic disease is why pfts are usually ordered that will be our subsequent Focus as a diagnostic tool pfts help classify defused lung disease into one of three broad categories first is obstru dve lung disease this includes COPD which means anything on the chronic bronchitis to empyema Spectrum asthma bronchiectasis which is an irreversible dilation and destruction of the bronchial
tree leading to Chronic infections and last cystic fibrosis the second category is restrictive lung disease which includes interstial lung disease chest wall pathology obesity and neuromuscular disease finally is pulmonary vascular disease which includes primary pulmonary hypertension and chronic thromboembolic disease for those viewers who already have some prior knowledge of pfts inclusion of pulmonary vascular disease in this discussion may seem unexpected since classic teaching of pfts usually omits this last category however as will be discussed in the fourth video on dlco pulmonary vascular disease can can display a specific abnormal pattern on pfts of which one
should be aware remember also that these categories are not mutually exclusive for example COPD can present with both obstructive and Vascular findings on pfts and Sarcoidosis while classically restrictive can present with any combination of all three what are the actual functions of the pulmonary system that are tested by pfts pfts actually provide information about every component of respiration it tells us about the patency of the Airways both large and small about the parena including both the alvioli and interstitium the pulmonary vasculature the Bellow and pump mechanism that is actually responsible for the changes in inter
thoracic pressure that cause air to move in and out of the lungs this includes both the diaphragm and the chest wall finally is the neural control of ventilation that is is the brain telling the lungs to breathe as frequently and deeply as it should in order to test all of these things there are different types of pfts I conceptually divide the types of pfts into two categories this is not any type of official classification just my own way of thinking about them first are the standard pfts this includes spirometry which is predominantly a measure of
air flow there are lung volumes and there is the dlco which is largely a measure of the Integrity of the Alvar capillary membrane typically when a physician nurse or respiratory therapist mentions the term pfts this set of three tests is usually what he or she is referring to in the absolutely most General sense spirometry is responsible for diag diagnosing obstructive lung disease lung volumes are responsible for diagnosing restrictive lung disease and the dlco in conjunction with other tests is responsible for suggesting the possibility of pulmonary vascular disease in addition to the standard pfts there are
also specialized pfts these are tests that can be done either in the PFT lab or at the bedside usually the latter each of these is fast and inexpensive and typically used in one or two specific scenarios there are arterial blood gases or abgs which is the topic of an entirely other video series in this channel exercise oximetry refers to measuring someone's pulse oxymetry at rest and with modest activity this is a quick and cheap way to pick up mild subclinical lung disease for the 6-minute walk test the patient is simply asked to walk as far
as possible during a 6-minute period This is not helpful for the diagnosis of any specific disease but it can be used for both prognosis and to monitor response to treatment the bedside Peak flow is a measure of the maximum expiratory air flow that can be delivered in a single breath typically used to gauge the severity of an asthma exacerbation finally maximum inspiratory and expiratory pressure can provide a rough estimate of diaphragmatic strength in neuromuscular disease including predicting risk of respiratory failure during exacerbations such as an impending myasthenic crisis a topic that will come up repeatedly
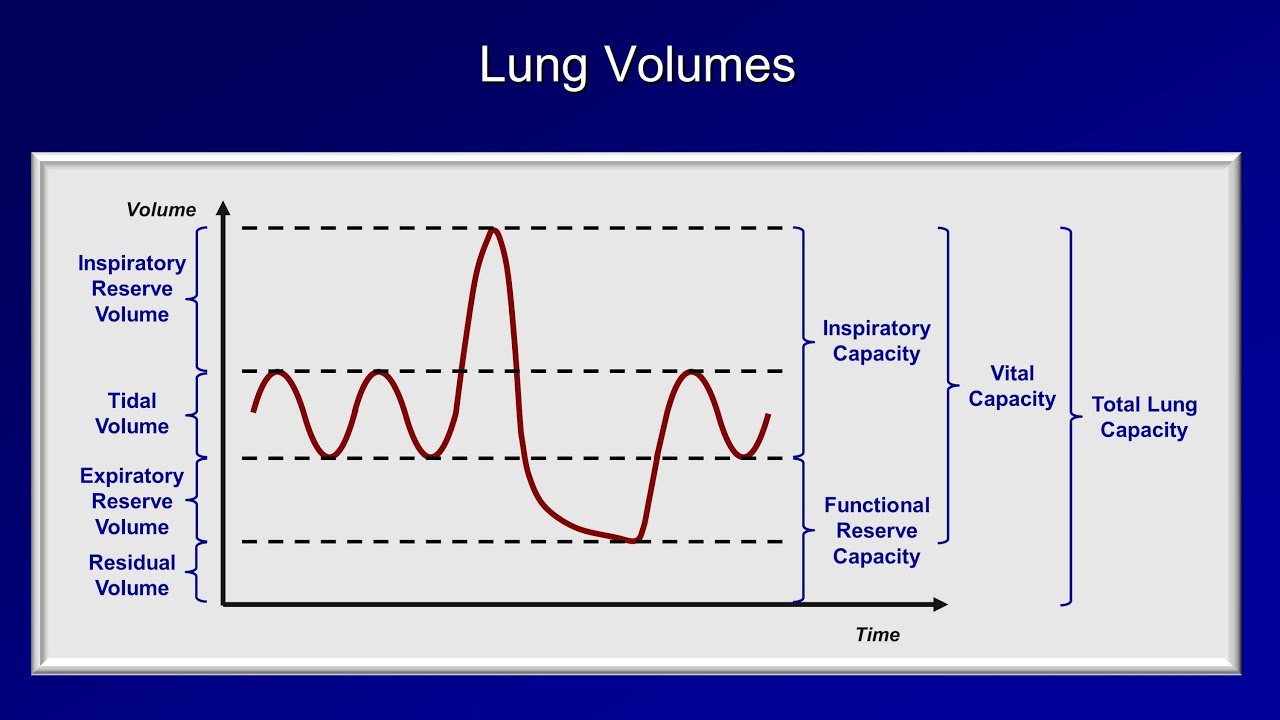
during the remaining videos is how the lung volume is divided up into different parts let me illustrate this we'll plot the volume of air within the lungs as a function of time and let's start off with a person breathing comfortably not doing anything special just sitting still breathing the volume of air exchange during each resting breath is called the tital volume while it may feel to the person that he or she is moving a significant amount of air you can see that as a fraction of the total air contained within the lung this is actually
just a small fraction imagine the patient is then specifically instructed to inhale as deeply as possible the amount of volume the person has now inhaled above the normal title vol volume is called The inspiratory Reserve volume the patient is now asked to breathe out as completely as possible the additional volume exhaled beyond what is exhaled during normal breathing is the expiratory reserve volume and finally when every last milliliter of air that can be squeezed out of the lungs has been the volume of air that is still left inside is called the residual volume while these
are the four divisions of our lung volume that add up to our maximum possible lung volume we typically don't consider the individual divisions during PFT interpretation as much as we consider specific groupings of volumes these groupings are called capacities for example the inspiratory capacity is the sum of the title volume and the inspiratory reserve volume the functional Reserve capacity is the sum of the exory reserve volume and the residual volume the vital capacity is the title volume plus the inspiratory and exory Reserve volumes and finally everything added together is called the total lung capacity I
appreciate that these eight terms seem more numerous than necessary and seem easy to get confused that will become even more true once we start referring to all of them by their acronyms all I can say is that I'm not personally responsible for the terminology and you will really need to be able to use most of these terms fluently that have a solid understanding of PFT interpretation before concluding this first video I wanted to show you an example of a PFT report so you have an idea of where the next three videos will be taking you
here's what a one-page PFT report might look like this may seem a little intimidating especially if you've never seen one before but I'll be covering what most of these numbers mean you can see that the values are reported as a percentage of that predicted given the patient's age gender and height what's considered normal varies a little between different physiologic parameters as well as between different PFT labs in general a measurement is considered normal if it falls within 80 to 120% of the value predicted for that patient or if it falls between the fifth and the
95th percentile for patients of identical iCal age gender and height in the US my impression is that most clinicians prefer the former definition of normal range over the ladder for most parameters in terms of the actual components of the report the top third is the spirometry where the key measurements are the FBC fe1 and the fb1 to FBC ratio also measured during spirometry is the patient's response to inhaled Bronco dilators and this little shape is the flow volume Loop which will be covered in the next video the second third of the PFT report is the
lung volumes of which the TLC or total lung capacity is the most important finally the last third is the diffusion capacity or dlco that concludes this introduction to pfts the next video will discuss spirometry and the flow volume [Music] Loop